
Undifferentiated connective tissue dysplasia in women of reproductive age: cross sectional study
Grudnitskaya E.N., Nebyshinets L.M.
Objective: The aim of the study was to identify the prevalence of undifferentiated connective tissue dysplasia (UCTD) and association with a burdened obstetric history (BOH) of miscarriage in women of reproductive age, who residents of the Minsk region (the Republic of Belarus).
Materials and methods: From March 2022 to May 2022, a cross sectional study was carried out. It included 384 women aged 22–46 years, who were admitted to healthcare facility “Maternity hospital of the Minsk region” (the Republic of Belarus) with purpose of pregravid preparation. According to the results of comprehensive evaluation, the presence of UCTD, prevalence of clinical signs of UCTD and association of UCTD with BOH were identified.
Results: Among women of reproductive age in the Minsk region, UCTD was identified in 35.7% of women (95% CI 30.9–40.7). In the group of patients with UCTD, BOH of miscarriage was 3.5 times more often – in 19/137(13,4%) women compared to women who had no UCTD – in 11/247 (4.5%); OR 3.5 [1.6; 7.5].
Conclusion: High prevalence of UCTD and association with BOH of miscarriage was identified in women of reproductive age, who are residents of the Minsk region. Based on the results of this study, formation of a comprehensive program for identifying UCTD at the stage of pregravid preparation needs to be determined.
Authors' contributions: Grudnitskaya E.N. – the concept and design of the study, material collection, statistic data processing; article writing; Nebyshinets L.M. – critical review of the article regarding the important intellectual context; approval of the final version of the article for publication.
Conflicts of interest: The authors have no conflict of interest to declare.
Funding: The study was carried within the State program of scientific researches of the Republic of Belarus “Translational medicine”, assignment No. 3.47 «To develop the method of preventive healthcare for spontaneous abortions and preterm births in pregnant women with connective tissue dysplasia”, state registration No. 20220318, implementation term 01.01.2022–31.12.2024.
Gratitude: The authors of the article express gratitude to Sergei L. Voskresensky, Professor, Dr. Med. Sci., Chief Researcher at the Research Laboratory of the Research Institute of Experimental and Clinical Medicine, Belarusian State Medical University, for this his consulting assistance.
Ethical Approval: The study was approved by Ethics Committee of Belarusian Medical Academy of Postgraduate Education (Protocol No. 1 of 06.02.2020).
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Grudnitskaya E.N., Nebyshinets L.M. Undifferentiated connective tissue dysplasia in
women of reproductive age: cross sectional study.
Akusherstvo i Gyneсologiya/Obstetrics and Gynecology. 2024; (5): 100-106 (in Russian)
https://dx.doi.org/10.18565/aig.2024.65
Keywords
undifferentiated connective tissue dysplasia
recurrent miscarriage
phenotypic signs of UCTD
Investigation of the prevalence of undifferentiated connective tissue dysplasia (UCTD) among women of reproductive age is an important area of medical research, since UCTD belongs to the group of connective tissue diseases that involve different body systems, including respiratory, digestive, osteoarticular, muscular, cardiovascular, endocrine, urinary and reproductive systems. It is not always clear, what causes UCTD. However, it is believed that connective tissue dysplasia may occur due to genetic mutations or exposure to various environmental factors [1]. The course of pregnancy in women with UCTD can be accompanied by the development of various pathological conditions, which in turn can lead to premature termination of pregnancy at different gestational age [2, 3].
Understanding the prevalence of UCTD among women of reproductive age is important for improving clinical practice, especially with regard to the diagnosis and treatment of women planning pregnancy.
The aim of the study was to identify the prevalence of UCTD and association with a burdened obstetric history (BOH) of miscarriage in women of reproductive age, the residents of the Minsk region (the Republic of Belarus).
Material and methods
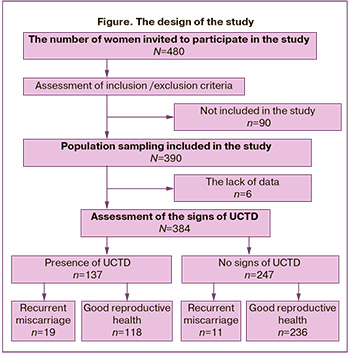
The design of the study: a cross-sectional study with random sampling was carried out from March 2022 to May 2022. The study included 384 women aged 22–46 years, who were admitted to healthcare facility “Maternity hospital of the Minsk region” (Republic of Belarus) with purpose of pregravid preparation and were invited to participate in the study (Figure).
When dealing with patients, the authors adhered to the ethical principles, which were developed by The World Medical Association (WMA) in the Declaration of Helsinki in 1964 and revised in October 2013 in Brazil in October 2013. The study was approved by the Ethics Committee of Belarusian Medical Academy of Postgraduate Education" (Protocol No. 1 of 06.02.2020) in the frames of implementation of research and development on topic “To develop the method of prevention spontaneous abortions and preterm births in pregnant women with undifferentiated connective tissue dysplasia”.
Inclusion criteria in the group with UCTD were the women with at least 6 external and/or visceral signs of UCTD with involvement of 3 or more different organ systems in the body. The following signs were taken into account: cutaneous (thin skin that can be easily damaged; loose, flaccid, dry skin; tensile strength of skin (>3 cm); atrophic striae; skin wound healing with formation of cigarette paper-like atrophic scars; keloid scars; brittle nails; crumpled ears), skeletal (dolichostenomelia; arachnodactyly; funnel chest, type 1; spinal deformity (scoliosis); retrognathia; arched palate; nasal septum deviation; delayed growth and crowding of teeth; X-shaped curvature, articular (joint hypermobility; subluxations and dislocations repeated in one or more than one joint), cardiovascular (mitral valve prolapse; chronic hypotension, arterial hypertension; varicose veins of lower extremities, vulva, pelvis at a young age), ophthalmic (myopia; retinal detachment; astigmatism), genitourinary (nephroptosis; genital prolapse), gastrointestinal (incompetence of the gastric cardia; kinking of the gallbladder), hemorrhagic (coagulopathies; excessive bleeding).
Inclusion criteria for both groups were 18–49 years of age, 2 and more clinically confirmed pregnancies that ended with term births, or 2 and more spontaneous abortions, readiness of participants to follow all study procedures, signing of informed consent to participate in the study.
Exclusion criteria were pregnancy at the time of admission to hospital, monogenic connective tissue disorders, refusal to answer the questions, undergo physical or instrumental examination, the presence of factors that increased the risk for a woman or prevented implementation of the conditions or completion of the study; unwillingness of a woman to participate in the study or difficulty in understanding informed consent, the purposes or requirements of the study.
Out of 480 women of reproductive age, who were invited to participate in the study, 390 women agreed to participate and met inclusion criteria, and had no characteristics for exclusion criteria. Among women, who underwent examination, 6 women answered the questionnaire partially. Thus, the data of 384 women were used for analysis. The mean age of women enrolled in the study was 33.02 (4.5) years.
The primary investigated outcome was the prevalence of UCTD among women of reproductive age. The secondary investigated outcome was relationship between UCTD and recurrent miscarriage, prevalence of the signs of UCTD in women of reproductive age.
Clinical and instrumental research methods were used, including anamnesis collection and investigation of complaints, general medical and gynecological examination, anthropometry, including measurements of body weight (kg), height, length of the hand, foot, arm span, upper and lower segment length (cm), assessment of body mass index. Aortic root measurement was performed by transthoracic echocardiography using the leading-to-leading edge technique and the inner edge-to-inner edge technique during systole (the maximum values of the diameter of the left ventricular outflow tract was obtained) [4]. The diagnosis of UCTD was made according to the National Clinical Guidelines of the Belarusian Scientific Society of Cardiologists “Diagnostics and Treatment of Hereditary and Multifactorial Connective Tissue Disorders”, taking into account the identified clinical symptoms [5].
Z-criterion was used for assessment of the expansion of aortic root (the difference between individual and normal values of aortic diameter). Z-score ≥2 indicated the value exceeding the normal value. To calculate z-score, the following formula was used:
Z = (IAD-NAD)/SE,
where IAD represents individual aortic diameter (cm);
NAD – normal aortic diameter (cm);
SE – standard error calculated for the regression model (0.261) [5].
NAD for adults was calculated using the Devereux formula (2012) [4]:
NAD=2.423+(age (years)*0.009)+ (BSA*0.461)-(Gender [M=1; F=2]*0.267),
where standard error of the mean was 0.267.
BSA stands for body surface area (m2).
BSA was estimated using Du Bois D. and Du Bois E.F. formula (1916) [6]:
BSA=0.007184*Height (cm)0.725*Weight (kg)0.425.
The diagnosis of recurrent miscarriage was made based on 2 or more clinically confirmed spontaneous abortions before 22 week’s gestation in medical history [7].
Statistical analysis
The sample size was calculated using the formula:
N=(Z1-α )2 Р((1-Р))/D2,
where N represents the sample size,
Z1-α = 1.96 (α=0.05),
Р – the prevalence of UCTD among women of reproductive age;
D – absolute error [8].
The prevalence of UCTD in population is 1:5 or 20% (or 0.2) [1]. UCTD prevalence data among women of reproductive age varies from 20%–30% [9] to 60%–80% [10]. In the absence of exact information, the expected prevalence rate was considered to be equal to 50% [8].
The sample size was increased by 25% given the fact that a part of women, who were invited to participate in the study, could refuse to be enrolled or could be excluded from the study [8]. The sample size comprised 480 women.
Statistical data processing was performed using software programs Statistica 12.0 (StatSoft, USA), Microsoft Office Exсel 2016, MedCalc 15.8 (MedCalc Software, Belgium). Quantitative indicators that have a normal distribution are represented as the mean (M), standard deviation (SD), qualitative and ordinal indicators are represented in percentage (%). The Shapiro–Wilk test was used to check the compliance of quantitative indicators with the normal distribution. Pairwise comparisons for categorical data in the groups were performed using Fisher's exact test. Estimation of odds ratio (OR) and its statistical significance was based on the values of the 95% confidence interval (CI). The method of Wilson was used for computing 95% CI of the proportion. In conducting a hypothesis test, statistically significant differences were considered to be at р<0.05.
Results and discussion
Out of 384 examined women of reproductive age, UCTD was identified in 137. The prevalence of UCTD was (137/384)*100%=35.7%. To extrapolate the obtained sample results to the entire population of women of reproductive age in the Minsk region, confidence interval with continuity correction for the proportion was calculated (the interval for the prevalence indicating the UCTD prevalence in population with 95% probability). The range of true prevalence of UCTD in women of reproductive age in the Minsk region with 95% probability was 30.9–40.7%. Therefore, the prevalence of UCTD in women of reproductive age in the Minsk region was 35.7% (95% CI 30.9–40.7). The obtained results demonstrated that the prevalence of UCTD among women of reproductive age is higher than in population. Currently available data indicate that the prevalence of UCTD depends on the age and gender of the individuals who undergo examination. The criteria for UCTD may be absent in childhood and manifest by the age of 40 years in 80% of cases [11]. The mean age of women included in the study was 33.02 (4.5) years, when manifestation of the signs of UCTD is increasing. According to literature, UCTD occurs in females and in first-degree relatives (mother, sister), and is identified in 93.4 and 84.6% of cases, and the course of pregnancy and delivery is associated with threatened miscarriage at 22 weeks’ gestation in 42% of cases [9].
Based on the results of assessment of reproductive anamneses, out of 384 women included in the study, 99% of women reported two or more failed pregnancies (25.8%) (95% CI 21.5–30.5). According to ESHRE Guidelines (2022), only the cases of clinically confirmed pregnancy based on ultrasound or pathological examination should be taken into account for making the diagnosis of “recurrent miscarriage” (RM) [7]. Unaccounted losses included the cases of implantation failure in IVF protocols, ectopic pregnancies, and trophoblastic disease. Based on clarification of anamnestic data it was found that RM was in 30 women. The prevalence of RM was equal to (30/384)*100% = 7,8%.
To extrapolate the obtained sample results to the entire population of women of reproductive age in the Minsk region, confidence interval with continuity correction for the proportion was calculated. The true range of patients of reproductive age in the Minsk region was 5.4–11.1% with 95% probability. Thus, the prevalence of RM in women of reproductive age in the Minsk region was 7.8 % (95% CI 5.4–11.1).
The obtained data correlate with published data on increasing risk of development of a number of diseases in patients with UCTD. In particular, investigation of the prevalence of UCTD in the adult patient population with gastroesophageal reflux disease showed that 45.7% of patients had phenotypic and visceral manifestations of UCTD, and the probability of developing gastroesophageal reflux disease in patients with a dysplastic-dependent phenotype increased by 3.7 times [12].
Some researchers classify UCTD as a “dangerous condition in women” due to the lack of diagnostic standard and development of a number of associated conditions/diseases [13].
The clinical manifestations of UCTD do not meet the criteria for known hereditary diseases/monogenic syndromes, but they can partially overlap or look like genetic syndromes. We assessed the phenotypic signs of UCTD that were found in women of reproductive age in the Minsk region, who were planning pregnancy, and represented the data in the Table.
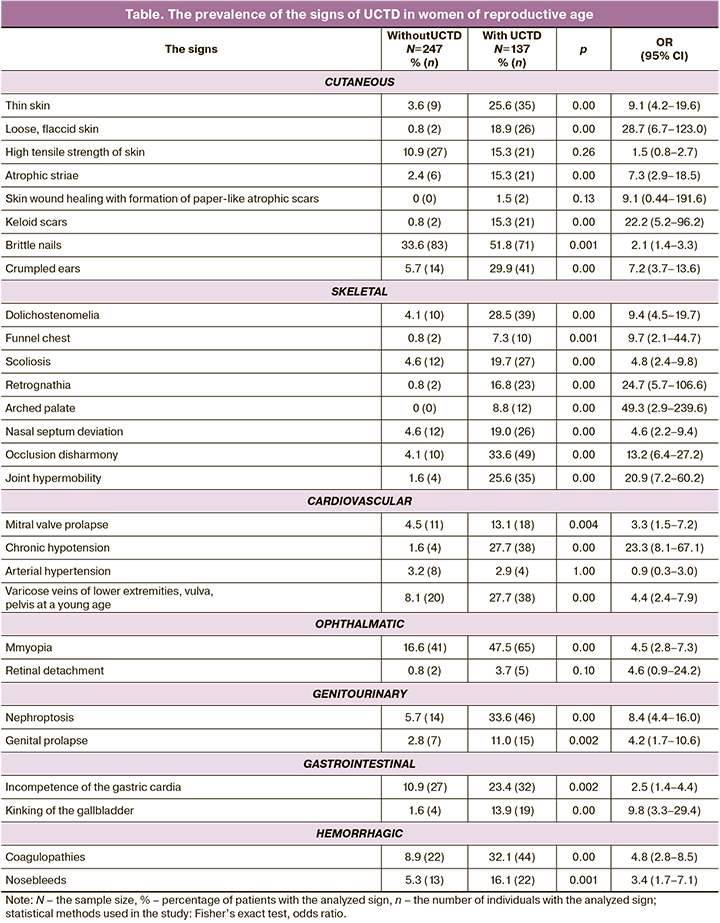
There were no statistically significant differences in 4 phenotypic signs: high tensile strength of skin, skin wound healing with formation of paper-like atrophic scars, arterial hypertension and retinal detachment.
Despite the statistical significance of differences in 8 signs (loose, flaccid skin; keloid scars, funnel chest; retrognathia; arched palate; occlusion disharmony; joint hypermobility; chronic hypotension, there is uncertainty in their identification in the group of women with UCTD due to a large scatter of data in the range of the values of confidence interval.
Among the identified phenotypic signs in women of reproductive age with UCTD, statistically significant were the following: thin skin, atrophic striae; brittle nails; crumpled ears; dolichostenomelia; spinal deformity (scoliosis); nasal septum deviation; occlusion disharmony; mitral valve prolapse; varicose veins of lower extremities, vulva, pelvis at a young age; myopia; nephroptosis; genital prolapse; incompetence of the gastric cardia; kinking of the gallbladder; coagulopathies; nosebleeds. Out of seventeen signs, five signs were most often in women with UCTD, such as brittle nails, myopia; nephroptosis; occlusion disharmony; coagulopathy.
The obtained data correlate with the results reported in literature. Most of researchers consider that vascular, valvular, ophthalmic, thrombohemorrhagic, cutaneous and skeletal signs stay ahead of other signs [1, 5, 14, 15].
Conclusion
As a result of our study it was established that UCTD can be found in every third woman of reproductive age, the residents of the Minsk region – 35.7% (95% CI 30.9–40.7) of women. It was found that there is a relationship between UCTD and recurrent miscarriage which occurred in women with UCTD 3.5 times more often – in 19/137 (13,4%) women versus women without UCTD – in 11/247 (4.5%); ОШ 3,5 [1.6;7,5].
Given the high prevalence of UCTD in women of reproductive age and serious risks of pregnancy, the introduction of standardized methods for diagnosing UCTD into clinical practice at the stage of pregravid preparation is of great importance. It will allow timely detection of disorders and take preventive and therapeutic measures. Early diagnosis of UCTD plays a key role in reducing the risks of obstetric complications, such as miscarriages and preterm births.
Further research in this field may help to develop effective management strategies for women with UCTD, taking into account their reproductive life plans.
References
- Недифференцированные дисплазии соединительной ткани (проект клинических рекомендаций). Терапия. 2019; 5(7): 9-42. [Undifferentiated connective tissue dysplasia (the project of guidelines). Therapy. 2019; 5(7); 9-42. (in Russian)]. https://dx.doi.org/10.18565/therapy.2019.7.9-42.
- Фадеева Т.С., Молоканова М.В., Павлов О.Г. Влияние степени тяжести недифференцированной дисплазии соединительной ткани на течение беременности. Вестник новых медицинских технологий. Электронное издание. 2019; 3: 12-7. [Fadeeva T.S., Molokanova M.V., Pavlov O.G. The influence of the severity of undifferentiated connective tissue dysplasia on pregnancy. Journal of New Medical Technologies, eEdition. 2019; (3): 12-7. (in Russian)]. https://dx.doi.org/10.24411/2075-4094-2019-16395.
- Смирнова Т.Л., Герасимова Л.И., Сидоров А.Е., Чернышов В.В., Губанова Е.А. Особенности течения беременности и родов у женщин с синдромом недифференцированной дисплазии соединительной ткани. Практическая медицина. 2018; 16(6): 39-44. [Smirnova T.L., Gerasimova L.I., Sidorov A.E., Chernyshov V.V., Gubanova E.A. Features of the course of pregnancy and childbirth in women with syndrome of undifferentiated connective tissue dysplasia. Practical Medicine. 2018; 16(6): 39-44. (in Russian)]. https://dx.doi.org/10.32000/2072-1757-2018-16-6-39-44.
- Devereux R.B., de Simone G., Arnett D.K., Best L.G., Boerwinkle E., Howard B.V. et al. Normal limits in relation to age, body size and gender of two-dimensional echocardiographic aortic root dimensions in persons ≥15 years of age. Am. J. Cardiol. 2012; 110(8): 1189-94. https://dx.doi.org/10.1016/j.amjcard.2012.05.063.
- Министерство здравоохранения Республики Беларусь, Белорусское научное общество кардиологов, Белорусский государственный медицинский университет. Диагностика и лечение наследственных и многофакторных нарушений соединительной ткани. Национальные клинические рекомендации. Минск; 2014. 75c. [Ministry of Health of the Republic of Belarus, Belarusian Scientific Society of Cardiology, Belarusian State Medical University. Diagnosis and treatment of hereditary and multifactorial connective tissue disorders. National clinical guidelines. Minsk; 2014. 75p. (in Russian)].
- Du Bois D., Du Bois E.F. A formula to estimate the approximate surface area if height and weight be known. Arch. Intern. Med. 1916;17: 863-71.
- ESHRE Guideline Group on RPL; Bender Atik R., Christiansen O.B., Elson J., Kolte A.M., Lewis S., Middeldorp S. et al. ESHRE guideline: recurrent pregnancy loss: an update in 2022. Hum. Reprod. Open. 2023; 2023(1):hoad002. https://dx.doi.org/10.1093/hropen/hoad002.
- Холматова К.К., Горбатова М.А., Харькова О.А., Гржибовский А.М. Поперечные исследования: планирование, размер выборки, анализ данных. Экология человека. 2016; 2: 49-56. [Kholmatova K.K., Gorbatova M.A., Kharkova O.A., Grjibovski A.M. Cross-sectional studies: planning, sample size, data analysis. Human Ecology. 2016; (2): 49-56. (in Russian)].
- Айрапетов Д.Ю. Значение недифференцированной дисплазии соединительной ткани в формировании женского бесплодия. Акушерство и гинекология. 2008; 2: 47-9. [Airapetov D.Yu. Value of undifferentiated connective tissue dysplasia in the development of female infertility. Obstetrics and Gynecology. 2008; (2): 47-9. (in Russian)].
- Сметанин М.Ю., Пименов Л.Т., Чернышова Т.Е., Кононова Н.Ю. Оценка обеспеченности витамином D у женщин репродуктивного возраста с дисплазией соединительной ткани. Терапия. 2019; 7: 81-3. [Smetanin M.Yu., Pimenov L.T., Chernyshova T.E., Kononova N.Yu. Assessment of vitamin d in women of reproductive age with connective tissue dysplasia. Therapy. 2019; (7): 81-3 (in Russian)]. https://dx.doi.org/10.18565/therapy.2019.7.81-83.
- Смольнова Т.Ю., Адамян Л.В. Динамика фенотипических признаков синдрома дисплазии соединительной ткани в различные возрастные периоды. Актуальность проблемы в акушерстве и гинекологии. Акушерство и гинекоогия. 2013; 4: 74-9. [Smolnova T.Yu., Adamyan L.V. Time course of changes in the phenotypic signs of connective tissue dysplasia at different ages: the urgency of the problem in obstetrics and gynecology. Obstetrics and Gynecology. 2013; (4): 74-9. (in Russian)].
- Джулай Т.Е., Джулай Г.С. Прогностическое значение диспластозависимых фенотипических и висцеральных проявлений при гастроэзофагеальной рефлюксной болезни, ассоциированной с дуоденогастроэзофагеальным рефлюксом. Экспериментальная и клиническая гастроэнтерология. 2022; 200(4): 41-7. [Dzhulay T.E., Dzhulay G.S. Predictive value of dysplastic-dependent phenotypic and visceral manifestations in gastroesophageal reflux disease associated with duodenogastroesophageal reflux. Experimental and Clinical Gastroenterology. 2022; 200(4): 41-7. (in Russian)]. https://dx.doi.org/10.31146/1682-8658-ecg-200-4-41-47.
- Фадеева Т.С. Дисплазия соединительной ткани: новые горизонты проблемы: монография. Чебоксары: ИД «Среда»; 2018.76с. [Fadeeva T.S. Connective tissue dysplasia: new horizons of the problem: monograph. Cheboksary: Publishing House "Sreda"; 2018. 76p. (in Russian)].
- Смирнова Т.Л., Герасимова Л.И. Особенности клинических проявлений синдрома недифференцированной дисплазии соединительной ткани. Доктор.Ру. 2018; 8: 40-4. [Smirnova T.L., Gerasimova L.I. Specific clinical features of undifferentiated connective tissue dysplasia syndrome. Doctor.Ru. 2018; (8): 40-4. (in Russian)]. https://dx.doi.org/10.31550/1727-2378-2018-152-8-40-44.
- Сметанин М.Ю., Пименов Л.Т., Чернышова Т.Е. Гормональный профиль и показатели минерального обмена у женщин с дисплазией соединительной ткани. Практическая медицина. 2018; 1: 140-3. [Smetanin M.Yu., Pimenov L.T., Chernyshova T.E. Hormonal profile and indicators of mineral metabolism in women with connective tissue dysplasia. Practical Medicine. 2018; (1): 140-3. (in Russian)].
Received 20.03.2024
Accepted 07.05.2024
About the Authors
Elena N. Grudnitskaya, PhD, Associate Professor, Associate Professor of the Department of Obstetrics and Gynecology, Institute of Advanced Training and Retraining of Healthcare Personnel, Belarusian State Medical University, 220013, Republic of Belarus, Minsk, P. Brovki str., 3, bldg. 3, +37529560-53-61, grudnickaja@mail.ru,https://orcid.org/0009-0003-5268-4029
Larysa M. Nebyshynets, PhD, Associate Professor, Head of the Department of Obstetrics and Gynecology, Institute of Advanced Training and Retraining of Healthcare Personnel, Belarusian State Medical University, 220013, Republic of Belarus, Minsk, P. Brovki str., 3, bldg. 3., +37529634-93-23, larisa_minsk08@mail.ru,
https://orcid.org/0009-0002-3966-4173
Similar Articles

