
Enterosorption in the treatment of patients with chronic endometritis
This was a prospective controlled comparative open-label study of the use of the enterosorbent polymethylsiloxane polyhydrate (Enterosgel) in patients diagnosed with chronic endometritis.Manukhin I.B., Kraposhina T.P., Kerimova S.P., Khovanov A.V.
Objective. To analyze the effectiveness of modern enterosorption aimed at restoring the reproductive potential of patients with missed abortion and the patients who are at risk for this condition.
Materials and methods. The effectiveness of enterosorption was evaluated using the surrogate parameter, namely, normalization of the endotoxin level in the general hemocirculation, development and successful outcome of the subsequent pregnancy. The endotoxin level was used as the primary endpoint due to the fact that there was a relationship between endotoxinemia and changes in the level of proinflammatory cytokines in the peripheral bloodstream with the persistent infectious agent in the genital tract; this relationship was shown to affect the chronization of the inflammatory process in the uterine cavity. To describe the quantitative variables, we used the median, upper and lower quartiles in the Me (LQ;UQ) format. The indicators among two and three or more groups were compared using the Mann–Whitney and Kruskal–Wallis tests, respectively.
Results. The enterosorbent Enterosgel was shown to be effective and safe in restoring the reproductive potential of this group of patients, whose level of endotoxin in peripheral blood and cytokines of the first phase of the immune response (IL-1β, IL-6, and TNF-α) was corrected. The most significant results were obtained after the treatment of patients diagnosed with missed abortion who followed a treatment regimen polymethylsiloxane polyhydrate + synbiotic.
Conclusion. The obtained data indicate that it is advisable to suppress the inflammatory process in the uterine cavity using broad-spectrum antibiotics and to correct the state of anti-endotoxin immunity with the help of enterosorbent Enterosgel.
Keywords
missed abortion
endotoxin aggression
early cytokines
chronic endometritis
Enterosgel
Normalization of increased endotoxin levels and restoration of the enterohematic barrier (gastrointestinal mucosa) are currently the promising areas in the development of pharmacological care for various diseases [1, 2]. Intestinal adsorbents (enterosorbents) are the medications that provide an adequate response to both of the above-mentioned components of the pathogenesis of diseases. The possibilities of enteral detoxification have been increased due to the appearance of the modern enterosorbent polymethylsiloxane polyhydrate (Enterosgel, produced by LLC TNC SILMA, Russia, marketing authorization No. 000036). The medication demonstrates a sorption activity against the endotoxin of gram-negative bacteria (lipopolysaccharide), and it simultaneously sorbs low-molecular substances, such as medical preparations, in a relatively small amount [3, 4]. Therefore, it can be recommended as a method for treating gestational pyelonephritis and postpartum purulent-septic complications [5].
Missed abortion is a polyetiological nosology, which is often caused by prolonged persistence of a causative agent in the mucous membrane of the uterine cavity with the subsequent development of an inflammatory process, namely, chronic endometritis. This inflammatory process is accompanied by multiple secondary morphofunctional changes that lead to disorders of cyclic transformation and receptivity of the endometrium. It should be noted that chronic endometritis is confirmed histologically in 72% of patients with diagnosed sexually transmitted infections and in 68% of patients with tuboperitoneal infertility [6].
In the last decade, some researchers have published the data on the role of endotoxin in the chronicity of inflammatory processes. Endotoxin is involved in the regulation of various body systems and it determines the fundamental level of physiological activity of these systems in regularly changing external conditions. Endotoxin is able to perform this function due to a wide range of biological properties and the ability to interact with various receptors. The elimination of endotoxin from the body to a greater extent is due to binding to liver histiocytes; this interaction results in the activation of the production of tumor necrosis factor-alpha, interleukins and interferons. They, in turn, have a general non-specific resistance of the body: antitumor, antibacterial and antiviral immunity [7–2]. If the cytokine levels of the first phase of the immune response and anti-endotoxin immunity do not correspond to normal levels, it can be suggested that the inflammatory process in the uterine body mucosa is chronic.
The objective of our study was to analyze the role of endotoxin and anti-endotoxin aggression at early stages of gestation during the development of chronic endometritis, which may result in missed abortion. Our research was also aimed at determining the methods for correcting anti-endotoxin immunity.
The primary results were evaluated on the basis of normalization of the elevated level of endotoxin in the gram-negative flora, which was determined using the micro-LAL test, as well as the level of proinflammatory cytokines IL-1β, IL-6, tumor necrotic factor-alpha (TNF-α). The secondary results were evaluated based on the development and course of the subsequent pregnancy, which ended in childbirth. The follow-up period was 2 years.
Materials and Methods
During the controlled comparative open-label study, there was an assessment of effectiveness, tolerability and safety of enterosorbent Enterosgel in patients diagnosed with chronic endometritis after missed abortion. The study included 128 patients of reproductive age (25.50 (19.00; 32.00) years): 98 patients of the main group who experienced missed abortions up to 12 weeks’ gestation and 30 women of similar gestational age who were hospitalized for elective artificial abortion composed the control group (Fig. 1). The main group was divided into three subgroups (Fig. 1).
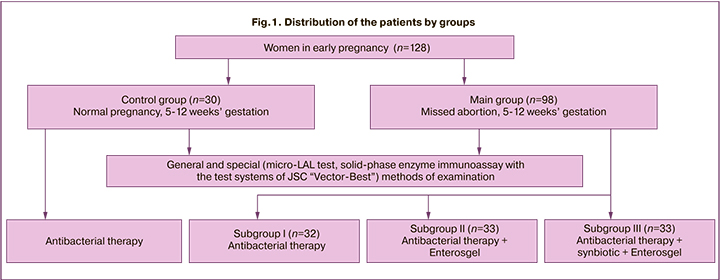
The first subgroup included 32 patients diagnosed with missed abortion. The patients of this subgroup received the treatment which is administered to patients after medical termination of pregnancy in accordance with the Order of the Russian Ministry of Health No. 572n dated November 1, 2012 “On approval of the procedure for providing medical care in the profile Obstetrics and Gynecology (except for the use of assisted reproductive technologies)” for the prevention of postoperative complications. This therapy included injectable 3rd generation broad-spectrum antibiotic cephalosporin (ceftriaxone) taken intramuscularly 1 g once a day for 7 days and metronidazole 250 mg 3 times a day for 7 days.
In the second subgroup, 33 patients diagnosed with missed abortion were administered the same treatment as in the first subgroup, but they also took Enterosgel sorbent (1 sachet of 15 g) 3 times a day for 2 weeks.
The third subgroup consisted of 33 patients with a similar diagnosis as in the previous two subgroups. They were administered a treatment similar to that of the second subgroup, and additionally they were prescribed a new generation synbiotic which was recommended to be taken for 14 days, 1 capsule per day. The synbiotic included prebiotic oligofructose 63 mg and lyophilizate of probiotic bacteria: Lactobacillus helveticus 9.00x108 CFU, Lactococcus lactis 9.00x108 CFU, Bifidobacterium longum 6.75x108 CFU, Bifidobacterium breve 4.50x108 CFU, Streptococcus thermophilus 4.50x108 CFU, Lactobacillus rhamnosus 4.50x108 CFU, Lactobacillus casei 2.25x108 CFU, Lactobacillus plantarum 2.25x108 CFU, Bifidobacterium bi dum 2.25x108 CFU.
The patients with chlamydia infection were prescribed antibacterial therapy, namely doxycycline at a dose of 100 mg twice a day for 10 days. If a smear revealed a fungal infection, it was additionally recommended to take fluconazole 150 mg orally once. The patients with confirmed viral and bacterial infection were treated with suppositories of human recombinant interferon alpha-2b at a dose of 500,000 IU twice per rectum for 10 days in combination with broad-spectrum antibacterial drugs.
The study inclusion criteria were reproductive age of women and 5–12 weeks’ gestation. Informed consent to participate in the study was obtained from all the patients. Patients with uterine malformations, genital hypoplasia, endocrinopathies with a high level of androgen hormones and blood clotting disorders were excluded from the study. Also, the inclusion criterion was a normal karyotype based on the results of a cytogenetic study of the aborted materials.
The patients with gestation more or less than 5–12 weeks were not eligible for the study; the patients with diseases of other organs and systems, when gestation poses a risk to the life of the mother did not participate in the study. The exclusion criteria were the absence of a constructive dialogue with the patient, psychological and emotional disorders that prevent the signing of the informed consent, genetic and autoimmune disorders of the mother or father, acute infectious processes in the mother, as well as the refusal of the mother to participate in the study after signing the informed consent.
The examination of the patients included taking a medical history, laboratory (clinical, biochemical, bacterioscopic) analyses. Among the special methods used in the research, there was PCR-diagnosis of genital infections, the study of endotoxemia and anti-endotoxin immunity, determining the so-called early cytokines. A histological study of the obtained material was carried out after medical termination of missed abortion.
The quantitative assessment of the endotoxin content in the total blood flow was determined using a micro-LAL test (Limulus Amebocyte Lysate test), which is based on the ability of the hemolymph of the Limulus Polyphemus crustacean to coagulate upon contact with endotoxins of various origins [7, 11, 13]. Endotoxin is measured in endotoxin units per milliliter (EU/mL). One endotoxin unit (EU) was defined as 0.2 ng of EC-2.
The levels of proinflammatory cytokines IL-1β, IL-6, and TNF-α in the total blood flow were determined using the method of solid-phase enzyme immunoassay with the test systems of JSC “Vector-Best” (Russia): Interleukin-1-beta, ELISA-best, Interleukin-6-ELISA-BEST, and alpha-TNF-ELISA-BEST [14].
Statistical analysis
To describe the quantitative variables, we used the median, upper and lower quartiles in the Me (LQ;UQ) format. The indicators among two and three or more groups were compared using the Mann–Whitney and Kruskal–Wallis tests, respectively. The statistical significance of the differences among the groups for binary and nominal scales was determined using the Pearson’s χ2-test in the case of independent samples, and using the McNemar’s test in the case of dependent samples. To compare the two periods, the analysis of the dependent indicators was carried out on the basis of the nonparametric Wilcoxon method. The results were considered statistically significant at the level of 0.05. Statistical processing of the data was performed using Statistica 10 and SAS JMP 11 software packages [15–18].
Results and Discussion
Taking patients’ medical history made it possible to reveal the past diseases that could affect the processes of the formation and functional development of the female reproductive system.
The data on extragenital pathologies of the patients diagnosed with missed abortion and patients with normal gestation are shown in Figure 2.
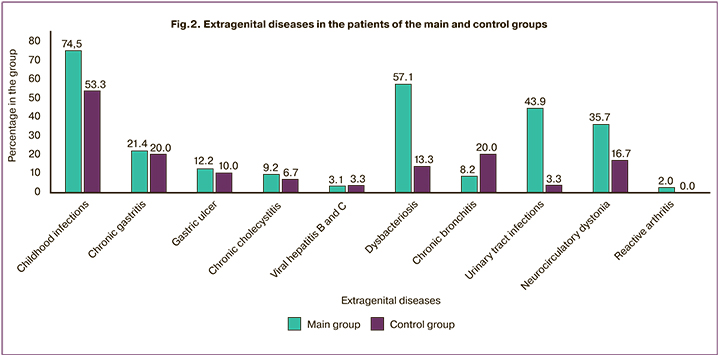
The data presented in Figure 2 show that inflammatory diseases of the urinary system (p<0.001), childhood infections (p=0.03) and dysbacteriosis (p<0.001) were more often revealed in the history of patients of the main group in comparison with the frequency of the same diseases in the control group.
On the basis of these findings, it can be assumed that there is a probability of their impact on the immune homeostasis in the patients included in the main group.
In both groups, the frequency of neurocirculatory dystonia, chronic gastritis, viral hepatitis, ulcer disease, and chronic bronchitis did not differ significantly (p>0.05).
The analysis of the patients’ medical history revealed that inflammatory processes of the genital tract occurred more frequently in patients of the main group than in the control group. Among the patients diagnosed with missed abortion, colpitis in combination with cervicitis was detected in 29.6% of cases, inflammation of the cervix in combination with bacterial vaginosis was revealed in 22.4% of patients, inflammation of the vaginal mucosa in combination with bacterial vaginosis was detected in 30.6%, and inflammation of the cervix and appendages were combined in 17.3% of cases. The frequency of similar disorders and their combinations was different in the group of patients with normal pregnancy and it was 26.7%, 23.3%, 36.7%, 13.3%, respectively.
The analysis of gynecological history of the patients with missed abortion showed that they previously experienced endometriosis, endometrial polyps, endometrial hyperplasia; the rate of these diseases was 27.6%, 13.3% and 13.3%, respectively. These indicators are higher in comparison with similar disorders in the group of healthy patients (20.0%, 0.0% and 3.3%, respectively). The indicator endometrial polyp was found to have a statistically significant difference in the main group compared to the control group (by 13.3%; p=0.04) [13].
The results of the polymerase chain reaction (PCR) which was aimed at determining the species of microorganisms from the cervical canal indicated a high frequency of causative agents associated with sexually transmitted infections (STIs) in patients diagnosed with missed abortion. The frequency of their detection was the following: Chlamydia trachomatis – 10.2% of patients, Mycoplasma genitalium – 18.4%, Neisseria gonorrhoeae – 1%, Trichomonas vaginalis – 2%, Herpes simplex virus (HSV) (type 1, type 2) – 3.1%, Cytomegalovirus (CMV) – 3.1%, Human papillomavirus (HPV) – 21.4%, Ureaplasma urealyticum – 27.6% (p<0.01). Similar indicators in the control group were significantly lower: HPV – 6.7%, Ureaplasma urealyticum – 3.3%, Chlamydia trachomatis – 0.0%; Mycoplasma genitalis, Neisseria gonorrhoeae, Trichomonas vaginalis, HSV type 1 and HSV type 2 as well as CMV were not detected.
The results of PCR which was aimed at determining microbiocenosis in samples obtained from the uterine cavity in the main cohort of patients revealed the persistence of intrauterine causative agents in 100% of cases. Chlamydia trachomatis was diagnosed in 38.9% of patients, Ureaplasma urealyticum – 24.4%, Mycoplasma genitalium – 19.5%, Neisseria gonorrhoeae – 1.0%, Klebsiella – 75.5%, Enterococcus faecalis – 55.1%, HSV type 1 and HSV type 2 – 7.1%, CMV – 2.0%.
The data of histological analysis showed that 88.8% of women in the main cohort of patients were diagnosed with chronic endometritis with a long-running process, which is characterized by fibrosis and sclerosis of the walls of the uterine spiral arteries and leukocyte infiltration. Acute endometritis was observed in 11.2% of patients [13].
PCR results showed that causative agents in the uterine cavity were mainly bacterial in patients diagnosed with missed abortion during exacerbation of chronic endometritis (n=87) which was confirmed histologically. The frequency of the revealed agents was the following: Chlamydia trachomatis – 43.7% of patients, Ureaplasma urealyticum – 26.4%, Mycoplasma genitalium – 21.8%, Neisseria gonorrhoeae – 1.1%, Trichomonas vaginalis – 0.0%, Klebsiella – 82.8%, Enterococcus faecalis – 58.6%, HSV type 1 and type 2 – 3.4%, CMV – 0.0%, HPV – 0.0%. The patients of the main cohort diagnosed with morphologically confirmed acute endometritis (n=11) showed findings that were different from the patients with chronic endometritis: Chlamydia trachomatis – 0.0%, Ureaplasma urealyticum – 9.1%, Mycoplasma genitalium – 0.0%, Neisseria gonorrhoeae – 0.0%, Trichomonas vaginalis – 0.0%, Klebsiella – у 18.2%, Enterococcus faecalis – у 27.3%, HSV type 1 and HSV type 2 – 36.4%, CMV – 18.2%, HPV – 0.0%. It should be noted that the persistence of a viral and bacterial microcosm with a predominance of HSV over CMV was detected in the uterine mucosa of this cohort of patients. The results of our research are consistent with the data obtained in the study conducted by N.A. Sementsova (2013) [19].
Descriptive statistics of quantitative variables for the categories Personal Data and Results are presented in Table 1.
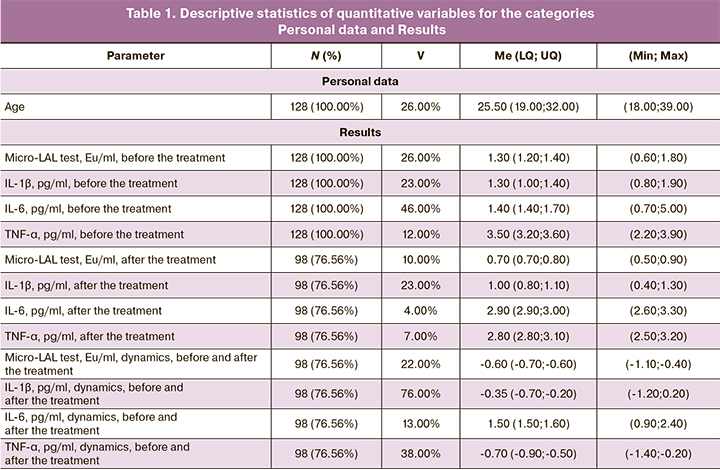
The results presented in Table 1 suggest that three indicators out of thirteen variables have the lowest percentages of data completeness, ranging from 98 (76.56%) to 98 (76.56%): TNF-α, pg/ml, dynamics, before and after the treatment; IL-6, pg/ml, dynamics, before and after the treatment and IL-1β, pg/ml, dynamics, before and after the treatment. These findings were sufficient to conduct a statistical analysis of the data and to draw statistical conclusions. The coefficient of variation ranges from 4 to 76%, which indicates a high level of heterogeneity of some indicators under study. The most homogeneous indicators were IL-6, pg/ml, after the treatment; TNF-α, pg/ml, after the treatment; Micro-LAL test, Eu/ml, after the treatment; the most heterogenous indicators were IL-1β, pg/ml, dynamics, before and after the treatment; IL-6, pg/ml, before the treatment; TNF-α, pg/ml, dynamics, before and after the treatment.
 The results of the micro-LAL test show that the level of lipopolysaccharide in the systemic blood flow in patients with normal pregnancy (n=30) does not exceed the generally accepted normal indicator (up to 1.0 Eu/ ml [7]) and it was 0.70 (0.60; 0.70) Eu/ml.
The results of the micro-LAL test show that the level of lipopolysaccharide in the systemic blood flow in patients with normal pregnancy (n=30) does not exceed the generally accepted normal indicator (up to 1.0 Eu/ ml [7]) and it was 0.70 (0.60; 0.70) Eu/ml.
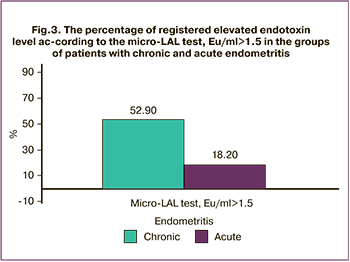
According to the results of the micro-LAL test, women with verified chronic endometritis had an increased level of endotoxin in blood plasma, namely, 1.30 (1.30; 1.40) Eu/ml, which is statistically significantly different from that in the control group (p<0.001). The studies demonstrate that lipopolysaccharide level in the blood exceeded 1.5 Eu/ml in 52.9% of patients diagnosed with chronic endometritis compared to patients with acute endometritis (p<0.01) (Fig. 3).
When determining proinflammatory cytokines in the blood circulation, it was found that indicators of IL-1β, IL-6 corresponded to 1.35 (1.30;1.50) pg/ml and 1.40 (1.30;1.50) pg/ml in the patients of the main group, respectively; and indicator IL-1β was 0.80 (0.80; 0.88) pg/ml, IL-6 was 2.90 (2.40; 3.68) pg/ml in the patients of the control group (p<0.001; p<0.001). It is worth noting that IL-6 suppressing the excessive production of IL-1β and TNF-α, is reduced by 2.2 times in the patients of the main group in comparison with those of the control group; this is observed in the case of long-term persistence of infection [14].
After medical termination of pregnancy (mifepristone 200 mg per os once; after 24–48 hours – misoprostol 200 mg sublingually once), the patient was administered the above-mentioned therapy. The patients of the main group were divided into three subgroups depending on the treatment regimen after emptying the uterine cavity [14].
After the treatment, the patient’s immune status was assessed again. The results confirmed that all women in the main group were able to achieve normal indicators of anti-endotoxin and general immunity, but their indicators were statistically significantly different depending on the use of a particular therapy regimen. In the third subgroup, the patients showed more remarkable changes in immune homeostasis, which was at the level of the upper limit of the control group (Table 2).
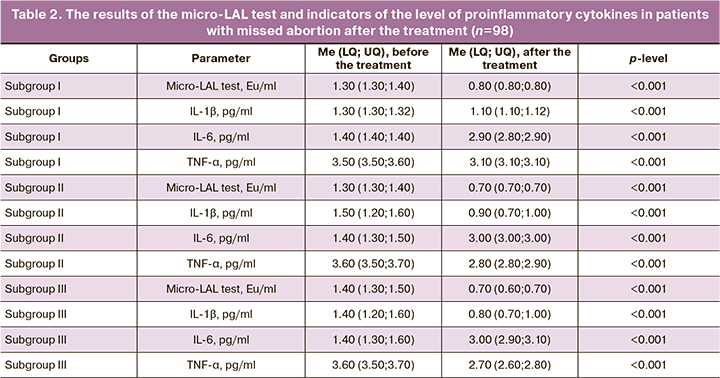
On the basis of the data presented in Table 2, it is possible to draw a conclusion that during the time period under review, there are statistically significant changes in all the indicators in the category Results. The most significant changes can be found for indicator IL-6, pg/ml (on average by 1.5 pg/ml; p<0.001), for indicator IL-1β, pg/ml (on average by 0.2 pg/ml; p<0.001), for indicator micro-LAL test, Eu/ml (on average by 0.5 Eu/ml; p<0.001).
Three subgroups of the patients of the main cohort in the period before and after the treatment were compared using quantitative indicators. The results of the statistical analysis of the comparison are presented in Tables 3 and 4.
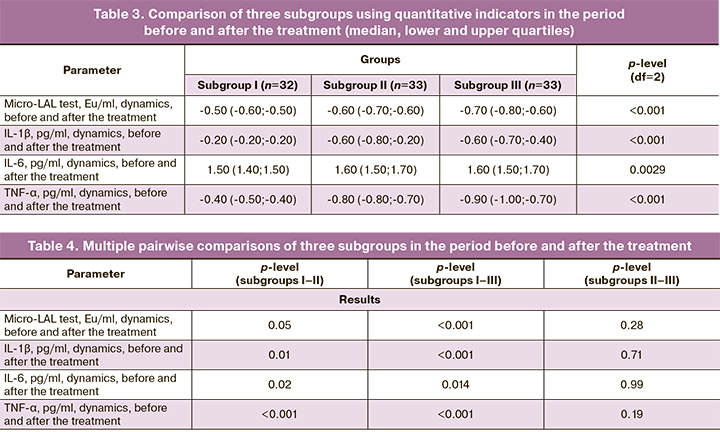
According to Tables 3 and 4, it can be concluded that there is a statistically significant difference in all the indicators of the category Results in three groups. The most significant differences were found for indicator TNF-α, pg/ml, dynamics, in the first subgroup in comparison with the third subgroup (on average by 0.5 dynamics; p<0.001); for indicator IL-1β, pg/ml, dynamics, in the first subgroup in relation to the second subgroup (on average by 0.4 dynamics; p<0.001); for indicator micro-LAL test, Eu/ml, dynamics, in the first subgroup in comparison with the third subgroup (on average by 0.2%; p<0.001).
Follow-up of the patients of the main group in dynamics showed that subsequent pregnancy which ended in childbirth at the end of the course of treatment and the rehabilitation period was observed in 6 women of the first subgroup, in 19 women of the second subgroup, and in 30 women of the third subgroup. The rest of the patients were not followed up due to the end of the study.
There were no side effects associated with the use of Enterosgel throughout the follow-up period in the main and control groups.
Conclusion
The obtained data indicate that it is advisable to suppress the inflammatory process in the uterine cavity using broad-spectrum antibiotics and to correct the state of anti-endotoxin immunity with the help of enterosorbent Enterosgel. The most optimal treatment regimen for the establishing a subsequent pregnancy, its course, and outcomes was the one that included 3rd generation broad-spectrum antibiotic cephalosporin, Enterosgel enterosorbent, and synbiotic; this regimen made it possible to reduce the number of reproductive losses in the future. The study showed good tolerability, efficacy and safety of enterosorbent Enterosgel in the complex therapy of patients with chronic endometritis.
References
- Павлов А.И., Хованов А.В., Хаваншанов А.К., Фадина Ж.В., Шамес А.Б. Место современной энтеросорбции в лечении и профилактике алкогольной болезни печени (обзор литературы). Эффективная фармакотерапия. 2019; 15(18): 36-41. [Pavlov A.I., Khovanov A.V., Khavanshanov A.K., Fadina Zh.V., Shames A.B. The place of modern enterosorption in alcoholic liver disease treatment and prevention (Literature review). Effective pharmacotherapy. 2019; 15(18): 36-41 (in Russian)].
- Павлов А.И., Хованов А.В., Фадина Ж.В. Борьба с эндогенной интоксикацией и восстановление кишечного барьера как цели назначения энтеросгеля при диарее неинфекционного генеза. Эффективная фармакотерапия. 2019; 15(2): 54-62. [Pavlov A.I., Khovanov A.V., Fadina Zh.V. Endotoxicosis and the intestinal barrier restoration as the goal of treatment of diarrhea of non-infectious genesis in the appointment of Enterosgel. Effective pharmacotherapy. 2019; 15(2): 54-62 (in Russian)].
- Howell C.A., Mikhalovsky S.V., Markaryan E.N., Khovanov A.V. Investigation of the adsorption capacity of the enterosorbent Enterosgel for a range of bacterial toxins, bile acids and pharmaceutical drugs. Sci. Rep. 2019; 9(1): 5629. https://dx.doi.org/10.1038/s41598-019-42176-z.
- Howell C., Markaryan E., Allgar V., Kemppinen A., Khovanov A., Pandya P. et al. Enterosgel for the treatment of adults with acute diarrhoea in a primary care setting: a randomised controlled trial. BMJ Open Gastroenterol. 2019; 6(1): e000287. https://dx.doi.org/10.1136/bmjgast-2019-000287.
- Серов В.Н., Сухих Г.Т., ред. Клинические рекомендации. Акушерство и гинекология. 4-е изд. М.: ГЭОТАР-Медиа; 2014. 1024с. [Serov V.N., Sukhikh G.T., ed. Clinical guidelines. Obstetrics and gynecology. 4th ed. revised and additional. M .: GEOTAR-Media; 2014.1024 p. (in Russian)].
- Лызикова Ю.А. Хронический эндометрит как причина нарушений репродуктивной функции у женщин. Проблемы здоровья и экологии. 2015; 3: 9-16. [Lyzikova Yu.A. Chronic endometritis as a cause of disorders of the female reproductive function. Health and environmental issues. 2015; 3: 9-16. (in Russian)].
- Энукидзе Г.Г., Аниховская И.А., Марачев А.А., Яковлев М.Ю. Антиэндотоксиновое направление в лечении хронического воспаления и женского бесплодия. Серия: Новые лечебно-диагностические технологии. Т.3. М.: КДО-тест; 2007. 80с. [Enukidze G.G., Anikhovskaya I.A., Marachev A.A., Yakovlev M.Yu. Anti-endotoxin direction in the treatment of chronic inflammation and female infertility. Series: New medical and diagnostic technologies. Vol. 3. Moscow; 2007. 80 p.(in Russian)].
- Jacob A.J., Goldberg P.K., Bloom N., Degenshein G.A., Kozinn P.J. Endotoxin and bacteria in portal blood. Gastroenterology. 1977; 72(6): 1268-70.
- Яковлев М.Ю. Кишечный липополисахарид: системная эндотоксинемия – эндотоксиновая агрессия – SIRS – полиорганная недостаточность как звенья одной цепи. Бюллетень Волгоградского научного центра Российской академии медицинских наук и администрации Волгоградской области. 2005; 1: 15-8. [Yakovlev M.Yu. Intestinal lipopolysaccharide: systemic endotoxinemia – endotoxin aggression – SIRS syndrome and multiple organ failure as links of the same chain. Byulleten VNTs RAMN. 2005; 1: 15-8. (in Russian)].
- Khafipour E., Krause D.O., Plaizier J.C. A grain-based subacute ruminal acidosis challenge causes translocation of lipopolysaccharide and triggers inflammation. J. Dairy Res. 2009; 92(3): 1060-70. https://dx.doi.org/10.3168/jds.2008-1389.
- Бондаренко В.М., Лиходед В.Г., Яковлев М.Ю. Определение эндотоксина грамотрицательных бактерий в крови человека. Журнал микробиологии, эпидемиологии и иммунобиологии. 2002; 2: 83-9. [Bondarenko V.M., Likhoded V.G., Yakovlev M.Yu. Determination of endotoxin of gram-negative bacteria in human blood. Journal of Microbiology. 2002; 2: 83-9. (in Russian)].
- Zhang H.Y., Han D.W., Su A.R., Zhang L.T., Zhao Z.F., Ji J.Q. et al. Intestinal endotoxemia plays a central role in development of hepatopulmonary syndrome in a cirrhotic rat model induced by multiple pathogenic factors. World J. Gastroenterol. 2007; 13(47): 6385-95. https://dx.doi.org/10.3748/wjg.v13.i47.6385.
- Манухин И.Б., Крапошина Т.П., Керимова С.П. Эндотоксинемия и антиэндотоксиновый иммунитет у пациенток с неразвивающейся беременностью в I триместре. Российский вестник акушера-гинеколога. 2019; 19(3): 17-21. [Manukhin I.B., Kraposhina T.P., Kerimova S.P. Endotoxemia and antiendotoxin immunity in patients with anembryonic pregnancies in the first trimester. Russian Bulletin of the obstetrician-gynecologist. 2019; 19(3): 17-21. (in Russian)].
- Керимова С.П., Манухин И.Б., Крапошина Т.П. Иммунный гомеостаз у больных с неразвивающейся беременностью. Современная наука: актуальные проблемы теории и практики. Серия: Естественные и технические науки. 2019; 9: 139-43. [Kerimova S.P., Manukhin I.B., Kraposhina T.P. Immune homeostasis in patients with non-developing pregnancy. Modern science. Actual problems of theory and practice. Natural and Technical Sciences. Moscow. 2019; 9: 139-43. (in Russian)].
- Халафян А.А. SТАТISТIСА 6. Статистический анализ данных. 3-е изд. М.: Бином-Пресс; 2007. 512с. [Khalafyan A.A. STATISTISA 6. Statistical data analysis. 3rd ed. M.: Binom-Press; 2007. 512 p. (in Russian)].
- Вуколов Э.А. Основы статистического анализа. Практикум по статистическим методам и исследованию операций с использованием пакетов Statistica и Excel. М.: Форум: ИНФРА-М; 2004. 462с. [Vukolov E.A. Fundamentals of statistical analysis. Practical work on statistical methods and research of operations using the packages “Statistica” and “Excel”. M.: Forum; 2004. 464 p. (in Russian)].
- Боровиков В.П. STATISTICA. Искусство анализа данных на компьютере (+ CD-ROM). 2-е изд. СПб.: ГПП Печатный Двор им. А.М. Горького; 2003. 688с. [Borovikov V. STATISTICA: The Art of Data Analysis on a Computer (with CD-ROM), 2nd Edition. St.-Petersburg; 2003. 688 p. (in Russian)].
- Реброва О.Ю. Статистический анализ медицинских данных. Применение пакета прикладных программ STATISTICA. М.: МедиаСфера; 2002. 312с. [Rebrova O. Statistical analysis of medical data. Application of the STATISTICA application package. Moscow: Media Sphere; 2002. 312 p. (in Russian)].
- Манухин И.Б., Колесов А.А., Семенцова Н.А., Чабонян А.Г. Профилактика привычного невынашивания у пациенток с неразвивающейся беременностью на фоне хронического эндометрита. Акушерство и гинекология. 2013; 5: 76-80. [Manukhin I.B., Kolesov A.A., Sementsova N.A., Chabonyan A.G. Prevention of recurrent miscarriage in patients with non-developing pregnancy during chronic endometritis. Obstetrics and gynecology. Moscow. 2013; 5: 76-80. (in Russian)].
Received 17.11.2020
Accepted 13.01.2021
About the Authors
Igor B. Manukhin, Dr. Med. Sci., Professor, Head of the Department of Obstetrics and Gynecology, Faculty of General Medicine, A.I. Evdokimov Moscow State University of Medicine and Dentistry, Ministry of Health of Russia. E-mail: katemanu2008@mail.ru. ORCID: 0000-0001-9333-8024.127473, Russia, Moscow, Delegatskaya str., 20.
Tatyana P. Kraposhina, Cand. Med. Sci., Assistant of the Department of Obstetrics and Gynecology, Faculty of General Medicine, A.I. Evdokimov Moscow State University of Medicine and Dentistry, Ministry of Health of Russia. E-mail: martinas2008@mail.ru. ORCID: 0000-0001-8839-1138.
127473, Russia, Moscow, Delegatskaya str., 20.
Saida P. Kerimova, postgraduate student of the Department of Obstetrics and Gynecology, Faculty of General Medicine, A.I. Evdokimov Moscow State University of Medicine and Dentistry, Ministry of Health of Russia. E-mail: ksp-91@list.ru. ORCID: 0000-0003-3546-6866.
127473, Russia, Moscow, Delegatskaya str., 20.
Alexander V. Khovanov, Ph.D., “TNK SILMA” LLC. E-mail: hovanov@enterosgel.ru.
115573, Russia, Moscow, Shipilovskaya str., 50-1-2.
For citation: Manukhin I.B., Kraposhina T.P., Kerimova S.P., Khovanov A.V. Enterosorption in the treatment of patients with chronic endometritis.
Akusherstvo i Ginekologiya / Obstetrics and gynecology. 2021; 1: 110-118 (in Russian)
https://dx.doi.org/10.18565/aig.2021.1.110-118
Similar Articles

