
Ki-67 expression levels in mature cystic teratomas and ovarian cystadenomas: morphological characterization of proliferative activity
Ibragimova U.D., Asaturova A.V., Kozachenko I.F., Badlaeva A.S., Rogozhina A.S., Adamyan L.V.
Benign ovarian tumors occur significantly more frequently than malignant tumors. Distinguishing between benign, borderline, and malignant ovarian neoplasms is crucial, as they have substantially different clinical and biological profiles and require distinct management strategies. The Ki-67 index, a universal marker of cellular proliferation, reflects the level of mitotic activity within the tumor tissue.
Objective. To evaluate the proliferative activity of cells in mature cystic teratomas and benign cystadenomas of the ovary using immunohistochemical assessment of the Ki-67 index.
Materials and methods. This study enrolled 189 patients aged 18–45 years with histologically confirmed benign ovarian tumors (mature cystic teratomas and cystadenomas). Standard histological examination and immunohistochemical staining with monoclonal antibodies against Ki-67 were performed to quantify the percentage of immunopositive nuclei within distinct tissue components of each tumor. Continuous variables are summarized as mean ± standard deviation (SD).
Results. All tumors examined exhibited markedly low levels of proliferative activity. The mean Ki-67 index was 8.9% in the epithelium of mature cystic teratomas, 0.4% in glial inclusions of teratomas, and 1.1% in the cystadenoma epithelium. The Ki-67 index in the epithelium of mature cystic teratomas was higher than that in cystadenoma epithelium and the glial component of teratomas.
Conclusion. Mature cystic teratomas and ovarian cystadenomas are characterized by low proliferation activity. The Ki-67 index reflects the distinctive cellular activity within the various tissue components of these tumors and may serve as a morphological indicator of their biological behavior.
Authors' contributions. Adamyan L.V., Asaturova A.V., Kozachenko I.F. – conception and design of the study; Asaturova A.V., Ibragimova U.D., Kozachenko I.F., Badlaeva A.S., Rogozhina A.S. – data collection and processing; Asaturova A.V., Ibragimova U.D. – statistical analysis; Ibragimova U.D., Asaturova A.V., Kozachenko I.F. – drafting of the manuscript; Adamyan L.V. – editing of the manuscript.
Conflicts of interest. The authors have no conflicts of interest to declare.
Funding. There was no funding for this study.
Ethical Approval. The study was reviewed and approved by the Research Ethics Committee of the V.I. Kulakov NMRC for OG&P, Ministry of Health of Russia.
Patient Consent for Publication. All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement. The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Ibragimova U.D., Asaturova A.V., Kozachenko I.F., Badlaeva A.S., Rogozhina A.S., Adamyan L.V.
Ki-67 expression levels in mature cystic teratomas and ovarian cystadenomas:
morphological characterization of proliferative activity.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (5): 133-139 (in Russian)
https://dx.doi.org/10.18565/aig.2026.59
Keywords
Ki-67
immunohistochemistry
proliferation index
mature cystic ovarian teratoma
ovarian cystadenoma
benign ovarian tumors
Benign ovarian tumors (BOTs) are more prevalent than malignant tumors, accounting for 62–80% of all ovarian neoplasms [1, 2]. Among BOTs, mature cystic teratomas and serous/mucinous cystadenomas are frequently encountered in gynecological practice. These neoplasms are characterized by morphologically mature tissue composition and generally follow a favorable clinical course. International epidemiological data indicate that mature cystic teratomas are the most common germ cell tumors of the ovary, with an estimated incidence of 1.2–14.2 cases per 100,000 women per year, accounting for approximately 11% of all ovarian neoplasms [3].
Accurate differential diagnosis of benign, borderline, and malignant ovarian tumors is critically important for determining management strategies and predicting clinical outcomes. Accordingly, objective biomarkers are needed to reflect the proliferative potential of tumor cells and assist in confirming the benign nature of neoplasms.
Immunohistochemical detection of the Ki-67 antigen is widely employed to assess the proliferative activity of tumors at diverse anatomical sites. The Ki-67 protein is expressed in the cell nuclei during all phases of the cell cycle, except for G0. Consequently, the percentage of Ki-67-positive cells (Ki-67 index) serves as a reliable measure of the proliferating cell fraction [4]. In gynecologic oncology, Ki-67 is extensively used to characterize tumor cell proliferation. Malignant neoplasms generally exhibit higher Ki-67 indices than benign neoplasms. For example, malignant ovarian tumors typically demonstrate elevated Ki-67 expression, whereas benign ovarian tumors are characterized by markedly low values [5–8]. The Ki-67 index has been extensively investigated in ovarian neoplasms and has demonstrated clinical utility for tumor stratification [9–12]. Therefore, a quantitative assessment of Ki-67 expression may complement the conventional morphological evaluation of tumor tissue.
Mature cystic teratomas and ovarian cystadenomas are morphologically benign neoplasms. Mature teratomas contain fully differentiated derivatives of all three germ layers and lack the immature neuroectodermal components that define malignant (immature) teratomas [13–15]. Cystadenomas are cystic tumors lined by a single layer of epithelium devoid of cellular atypia and do not infiltrate surrounding tissues [16]. However, even histologically benign tumors can exhibit variations in cellular activity. Measuring the Ki-67 index across distinct tissue components of such neoplasms provides deeper insight into their biological characteristics and enables confirmation of the absence of foci with increased proliferation, which might suggest malignant transformation or tissue immaturity [17].
Objective: to evaluate the proliferative activity of cells in mature cystic teratomas and benign cystadenomas of the ovary using immunohistochemical assessment of the Ki-67 index.
Materials and methods
The study enrolled 189 patients of reproductive age (18–45 years) who were admitted to the Gynecology Department of Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology between 2022 and 2024 with a diagnosis of cystic ovarian mass (cystadenoma and/or teratoma). All participants provided written informed consent prior to their enrollment. All patients underwent surgical removal of the ovarian tumor, and the specimens were subsequently classified as mature cystic teratoma or benign cystadenoma based on histological examination. Preoperative and postoperative management followed the institutional standards of care.
The surgical specimens were pathologically examined. Tumor samples were fixed in neutral-buffered formalin and embedded in paraffin. Histological sections (4 µm thick) were stained with hematoxylin and eosin for morphological assessment. Detailed microscopic characterization confirmed the benign nature of each tumor and identified all the constituent tissue components. Mature teratoma was diagnosed when derivatives of all three germ layers were present without evidence of immature neuroectodermal structures. Cystadenoma was diagnosed when a cystic tumor lined by a single layer of epithelium without cellular atypia, stromal invasion, or infiltration of adjacent tissues was identified. Cystadenomas were further classified by epithelial type and the architectural configuration of the cyst lining.
Proliferative activity was assessed by immunohistochemical staining for Ki-67. Paraffin sections (4 µm thick) were mounted on adhesive-coated glass slides. Following deparaffinization, antigen retrieval was performed via heat-induced epitope retrieval using citrate buffer (pH ~6.0). The sections were then incubated with a primary monoclonal antibody against the Ki-67 antigen (mouse monoclonal antibody, clone MIB-1, 1:100 dilution; Dako/Agilent, Denmark). Visualization was achieved using a polymer-based detection system with 3,3'-diaminobenzidine (DAB) chromogen. Negative controls were prepared by substituting the primary antibody with a buffer solution, while a sample of ovarian carcinoma with documented high proliferative activity served as the positive control.
Immunopositive cells were identified by the presence of brown nuclear staining, regardless of the intensity. The Ki-67 index, defined as the percentage of cells with positive nuclear staining, was determined separately for each distinct tumor tissue component. For mature cystic teratomas, two parameters were calculated: the proportion of Ki-67-positive cells in the stratified squamous epithelium (ectodermal component) and glial tissue (neuroectodermal component). For cystadenomas, the percentage of Ki-67-positive epithelial cells lining the cystic cavity was calculated. Cell counting was performed using manual image analysis. A minimum of five high-power fields (×400 magnification) were photographed for each component, and the number of immunopositive nuclei and the total number of epithelial cells in each field were counted. The Ki-67 index was expressed as a percentage (number of positive nuclei/total number of tumor cells × 100%). The mean Ki-67 index was calculated for each case based on all analyzed fields. The results were also compared with published data on Ki-67 expression in analogous tumor types.
Statistical analysis
Statistical analysis was performed using GraphPad Prism version 8.4.3 (GraphPad Software LLC, USA). Continuous variables are presented as mean and standard deviation M (SD).
Results
Histological examination of 189 resected ovarian tumors confirmed their benign nature. Morphological assessment revealed that 111/189 (58.7%) tumors were mature cystic teratomas, while 78/189 (41.3%) were cystadenomas (serous, mucinous, or mixed). A small proportion of patients (6/189 (3.2%)) exhibited synchronous occurrence of both tumor types, with a mature cystic teratoma in one ovary and a cystadenoma in the contralateral ovary.
Mature cystic teratomas exhibit characteristic morphological features. Macroscopically, they presented as thin-walled cysts containing sebaceous material, hair inclusions, and variable amounts of other tissue. These components included mesodermal derivatives such as adipose, fibrous, and smooth muscle tissue, cartilage foci, and blood vessels. Additionally, some teratomas contained islands of neuroectodermal tissue represented by mature glial tissue. In cases of monodermal teratoma (dermoid cyst), histological examination showed that the cyst wall was lined by keratinizing stratified squamous epithelium underlain by dermis containing skin appendages, including hair follicles, sebaceous glands, and sweat glands. None of the examined teratoma specimens demonstrated features of immature embryonal tissue, such as neuroectodermal rosettes characteristic of Grade 1–3 immature teratomas, nor were any foci of "cellular" glia identified. The nuclei of all teratomatous cells, including epithelial, glial, and mesenchymal elements, lacked atypia, and mitotic figures were rare. These findings confirmed the diagnosis of a mature ovarian teratoma.
Benign ovarian cystadenomas consisted of thin-walled cystic cavities lined by a single layer of columnar or cuboidal epithelium. Depending on the histological subtype, the epithelial lining was serous, mucinous, or mixed, and in some cases, papillary projections were observed on the inner cyst surface. All cystadenomas lacked evidence of invasive growth or cytological atypia; the epithelium retained an intact basal layer, and the cells were morphologically uniform without pathological mitotic figures. Even in serous papillary cystadenomas, the papillae consisted of fibrous stromal cores lined by morphologically benign epithelium. No stromal invasion or signs of malignant transformation were noted. Thus, all examined tumors fulfilled the morphological criteria for mature benign neoplasms.
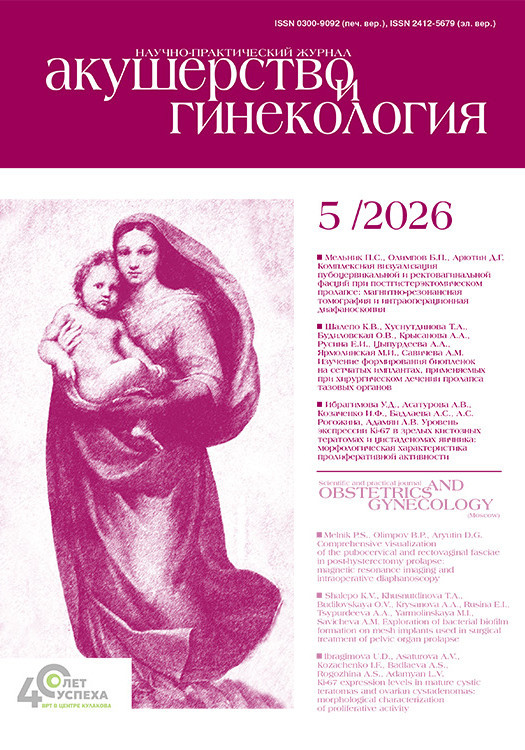
Immunohistochemical staining revealed varying levels of proliferative activity in the tumor tissues. In all cases, Ki-67 expression was focal, with a low number of positively stained nuclei. Nevertheless, the Ki-67 index varied substantially among the different tumor components. In mature teratomas, the highest proliferative activity is observed in the epithelial component of the dermoid cyst. The stratified squamous epithelium lining the cystic cavity contained a moderate number of Ki-67-positive nuclei, predominantly in the basal and parabasal epidermal layers. The mean Ki-67 index in the stratified squamous epithelium of teratomas was 8.9 (3.6)% (Fig. 1). Ki-67 expression in mature cystic teratomas reflects the moderate proliferative activity of the squamous epithelium, consistent with physiological epithelial renewal.
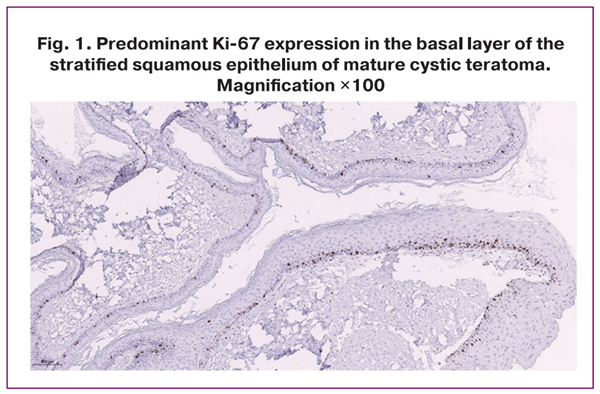
In contrast, Ki-67 expression in the neuroectodermal glial tissue within the teratomas was minimal. Only isolated cells with positive nuclear staining were identified in the fields containing mature neuroglial tissue. The mean Ki-67 index in the glial component was only 0.4 (0.1) % (Fig. 2), indicating an almost complete absence of proliferative activity.
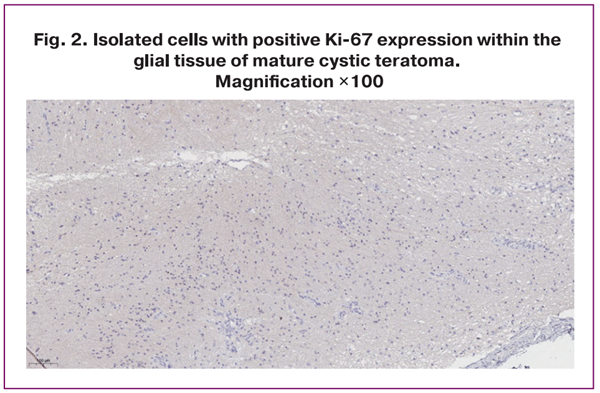
Benign ovarian cystadenomas, both serous and mucinous, also demonstrate very low proliferative activity. Immunohistochemical staining for Ki-67 revealed only a few positive nuclei within the single-layered epithelial lining of the cysts. In many microscopic fields, no stained cells were identified, whereas isolated Ki-67-positive nuclei were occasionally observed among hundreds of negative cells. The mean Ki-67 index in the epithelial lining of cystadenomas ranged from 1% to 2%; in our series, it was 1.1 (0.24)% (Fig. 3). Even in specimens with papillary intracystic projections, the proportion of proliferating cells remained low and did not differ substantially from that in smooth-walled cystadenomas.
The Ki-67 index in the stratified squamous epithelium of mature cystic teratomas was higher than that in the glial component of teratomas and the epithelium of cystadenomas. In contrast, no differences in Ki-67 expression were identified between serous and mucinous cystadenomas, both of which demonstrated comparably low proliferative activities.
Overall, all examined samples of mature cystic teratomas and cystadenomas exhibited low tumor cell proliferative potential. The overwhelming majority of cells (>90–99%) were outside of the cell cycle. These findings support the morphological conclusion that these tumors are benign and slow growing.
Discussion
The results of the immunohistochemical assessment of Ki-67 in BOTs indicate the extremely low proliferative activity of their cellular components. All examined mature cystic teratomas and cystadenomas demonstrated very-low Ki-67 indices. These findings complement the morphological characterization of BOTs and confirm their low-proliferative potential.
Mature teratomas exhibit heterogeneity in proliferative activity among different tissue components, reflecting their embryological origins. Specifically, approximately 8–9% of cells in the epidermal component of mature cystic teratomas were Ki-67-positive, predominantly localized within the basal layer. Our findings confirm that the squamous epithelium of mature cystic teratomas retains normal differentiation and proliferative activity comparable to that of the normal skin epithelium [5].
In contrast, the neuroglial tissue within mature teratomas exhibited virtually no proliferative activity. The Ki-67 index of 0.4% observed in our study indicates the absence of a substantial population of dividing glial cells. Under physiological conditions, mature glial tissue demonstrates minimal proliferative activity, except for a limited number of progenitor cells. Our findings are consistent with this concept, as the glial component of the teratomas exhibited features of functionally mature tissue. Importantly, the absence of proliferative activity within the glial areas indirectly suggests the absence of immature neuroectodermal foci. Even a small focus of immature neural tissue within a teratoma is expected to demonstrate increased cellularity, mitotic activity, and elevated Ki-67 expression [18]. For example, Hongo-Kohama M. et al. (2017) demonstrated that an increase in the histological grade of immature teratomas is associated with a marked increase in Ki-67 expression [19]. In highly malignant (Grade 3) ovarian teratomas, the proportion of Ki-67-positive cells within the neuroectodermal components may reach several tens of percent, whereas in mature (Grade 0) teratomas, it remains minimal [19]. Another study reported that "cellular neuroglia," which some authors consider a potential diagnostic feature of immature teratomas, is characterized by poorly defined borders, increased mitotic activity, necrotic foci, and high Ki-67 expression, whereas neuroglial tissue in mature teratomas is hypocellular, mitotically inactive, and demonstrates minimal Ki-67 staining [18,20]. Our observations are fully consistent with these published findings; glial foci in the examined teratomas met the criteria for mature tissue, including well-defined borders, absence of atypia and necrosis, and rare mitotic figures. Thus, a low Ki-67 index may serve as an additional morphological marker for the differential diagnosis of immature teratomas.
The findings for benign cystadenomas were also consistent with established patterns. We found that the epithelial lining of serous and mucinous cystadenomas had a Ki-67 index of approximately 1%, indicating an extremely small proportion of proliferating cells. Histologically, the epithelium of cystadenomas was characterized by small, uniform nuclei within a single-layer cuboidal or columnar epithelium, whereas mitotic figures were exceedingly rare. The absence of Ki-67 expression in most microscopic fields confirms that the cell cycle is minimally activated in these tumors. Similar findings have been reported in the literature; in typical benign serous and mucinous ovarian cystadenomas, only a small percentage of cells undergo mitosis [21]. For example, Singh N. and Kamath S.M. (2022) reported a mean Ki-67 index of approximately 0.99% in benign ovarian tumors compared with 64.5% in malignant tumors [5]. The authors emphasized that benign tumors exhibit minimal Ki-67 expression, close to background levels comparable to normal tissues, in sharp contrast to the markedly elevated indices observed in carcinomas [5].
Importantly, the presence of papillary structures in some cystadenomas was not associated with increased proliferation. Although papillary projections may be linked to enhanced epithelial proliferation, this phenomenon has not been observed in benign serous papillary cystadenomas. In our series, these cystadenomas demonstrated Ki-67 indices comparable to those of the smooth-walled cysts. Similar observations have been described previously: borderline serous tumors exhibit higher Ki-67 expression than benign tumors; however, the mere presence of papillary inclusions without atypia is not necessarily associated with increased Ki-67 expression [22]. These findings confirm that papillary cystadenomas without atypia remain morphologically benign and demonstrate minimal epithelial proliferation. None of the tumors in our study demonstrated elevated Ki-67 expression, a characteristic of borderline or malignant lesions. This is consistent with their benign growth patterns and extremely low proliferative potential.
From a practical perspective, Ki-67 assessment may serve as an additional morphological tool for the comprehensive evaluation of tumor tissue. Our findings suggest that when morphological assessment raises diagnostic uncertainty, immunohistochemical evaluation of Ki-67 expression may help determine the true biological activity of the tumor; a low Ki-67 index would support the morphological features of a benign lesion. Conversely, the identification of areas with substantially increased Ki-67 expression may indicate the presence of a borderline or malignant component, requiring more detailed examination. Rare cases of malignant transformation arising in mature cystic teratomas have been described in the literature; in such lesions, Ki-67 expression increases sharply to 30–40%, whereas the remaining cyst components retain low proliferative activity [23]. Therefore, focal increases in Ki-67 expression within an otherwise benign tumor should alert the pathologist and prompt a more careful evaluation.
The low proliferative activity observed in all examined samples reflects the morphological maturity and biological stability of the tumors. Previous studies have shown that low Ki-67 expression in BOTs is associated with favorable clinical outcomes and rare recurrence [5, 24]. Our findings are consistent with this observation.
Conclusion
Thus, the Ki-67 index may be used as an additional morphological marker of proliferative activity in tumor tissue and may complement standard histological examination in assessing the biological characteristics of benign ovarian neoplasms.
References
- Samaddar J.B., Barua M., Dutta Pal R., Mandal S., Samaddar D., Goswami B.K. Clinicopathological spectrum of ovarian neoplasms with a special emphasis on risk of malignancy index – a single institutional study. Asian J. Med. Sci. 2025; 16(9): 122-9. https://dx.doi.org/10.71152/ajms.v16i9.4713
- Mustafin C., Vesnin S., Turnbull A., Dixon M., Goltsov A., Goryanin I. Diagnostics of ovarian tumors in postmenopausal patients. Diagnostics (Basel). 2022; 12(11): 2619. https://dx.doi.org/10.3390/diagnostics12112619
- Aher K.D., Gadhire M., Bhosle A., Agarwal N. Giant mature cystic teratoma of the ovary mimicking a 36-week pregnancy in a 14-year-old female. Int. J. Res. Med. Sci. 2025; 13(12): 5539-42. https://dx.doi.org/10.18203/2320-6012.ijrms20253993
- Mordecai O.G., Oboma Y.I., Teme R. Immunocytochemistry profiling of ovarian cysts: a review of its clinical utility, future direction, and challenges. Tumor Discovery. 2025; 4(1): 14-26. https://dx.doi.org/10.36922/td.5369
- Singh N., Kamath S.M. Ki-67 immunostaining in epithelial ovarian tumors with clinicopathological correlation. Int. J. Med. Res. Health Sci. 2022; 11(5): 19-26.
- Dewi I.G.A.S.M., Susraini A.A.A.N., Ekawati N.P. HER2/neu and Ki-67 as prognostic factors in serous type ovarian carcinoma. Bali Med. J. 2020; 9(2): 567-71. https://doi.org/10.15562/bmj.v9i2.1926
- Basak B., Mondal S.K., Debnath S. WT1, Bcl-2, Ki-67 and Her2/Neu as diagnostic and prognostic immunomarkers in ovarian serous and endometrioid carcinoma. Int. J. Clin. Diagn. Pathol. 2020; 3(3): 153-7. https://dx.doi.org/10.33545/pathol.2020.v3.i3c.273
- ALgarsh H., Abusaida H., Torjman F. The correlate between argyrophilic nucleolar organizer region stain and Ki-67 immunohistochemistry in diagnostic breast cancer. Iberoam J. Med. 2020; 2(4): 285-92. https://dx.doi.org/10.5281/ZENODO.4043776
- Qasim Y.A., Saeed S.Z., Rashid I.M. Immunohistochemical study of P53 and Ki 67 expression in surface epithelial tumor of the ovary. Saudi J. Pathol. Microbiol. 2017; 2(3): 52-9. https://dx.doi.org/10.21276/sjpm.2017.2.3.3
- Zayyan M.S. Risk factors for ovarian cancer. In: Lasfar A., Cohen-Solal K., eds. Tumor progression and metastasis. 2020: 75-102.
- Zhang S., Zhang Y., Zhang X., Yang X., Liu L., Liu J. et al. Diagnostic extended usefulness of RMI: comparison of four risk of malignancy index in preoperative differentiation of borderline ovarian tumors and benign ovarian tumors. J. Ovarian Res. 2019; 12(1): 87. https://dx.doi.org/10.1186/s13048-019-0568-3
- Remnant L., Kochanova N.Y., Reid C., Cisneros-Soberanis F., Earnshaw W.C. The intrinsically disorderly story of Ki-67. Open Biol. 2021; 11(8): 210120. https://dx.doi.org/10.1098/rsob.210120
- Cong L., Wang S., Yeung S.Y., Lee J.H.S., Chung J.P.W., Chan D.Y.L. Mature cystic teratoma: an integrated review. Int. J. Mol. Sci. 2023; 24(7): 6141. https://dx.doi.org/10.3390/ijms24076141
- Cao Y., Wang B., Jia A.R., Li X., Yang L., Jia Z. Mature cystic teratoma of the ovary with a grossly visible, completely developed intestinal loop: a case report and review of the literature. Medicine (Baltimore). 2023; 102(26): e34081. https://dx.doi.org/10.1097/MD.0000000000034081
- Zhang J., He L., Yang L., Wang J., Wei L., Ma X., Jiang L. Ovarian collision tumor consisting of sclerosing stromal tumor and mature cystic teratoma complicated with Meigs syndrome: a case report. Oncol. Lett. 2022; 24(6): 443. https://dx.doi.org/10.3892/ol.2022.13563
- Elansary M.F.A.A., Alkafaji H.A., Al-Hilli N.M. Diagnostic evaluation of immunohistochemical expression of p16 and Ki67 in ovarian serous neoplasms. Iraqi Postgrad. Med. J. 2023; 22(2): 183-91. https://dx.doi.org/10.52573/IPMJ.2023.180588
- Li X., Tang X., Zhuo W. Malignant transformation of ovarian teratoma responded well to immunotherapy after failed chemotherapy: A case report. Ann. Palliat. Med. 2021; 10(7): 8499-505. https://dx.doi.org/10.21037/apm-20-2429
- Chai Y., Woo C.G., Kim J.Y., Kim C.J., Khang S.K., Kim J. et al. Diagnostic significance of cellular neuroglial tissue in ovarian immature teratoma. J. Pathol. Transl. Med. 2017; 51(1): 49-55. https://dx.doi.org/10.4132/jptm.2016.09.19
- Hongo-Kohama M., Kurata A., Hashimoto H., Fujita K., Horiuchi H., Nagao T., Kuroda M. Vascular smooth muscle cell maturation stage and Ki-67 index are diagnostic biomarkers for pathologic grade of ovarian teratoma. Int. J. Gynecol. Pathol. 2017; 36(6): 582-92. https://dx.doi.org/10.1097/PGP.0000000000000373
- Iemura Y., Yamada Y., Hirata M., Kataoka T.R., Minamiguchi S., Haga H. Histopathological characterization of the neuroglial tissue in ovarian teratoma associated with anti-N-methyl-D-aspartate (NMDA) receptor encephalitis. Pathol. Int. 2018; 68(12): 677-84. https://dx.doi.org/10.1111/pin.12732
- Sardar K., Singh J., Tirkey S. Ki67 immunoexpression in ovarian tumours. IOSR J. Dent. Med. Sci. 2018; 17(2): 34-7. https://dx.doi.org/10.9790/0853-1702163437
- Yu N., Wang N., Liu Y.F., Li Y.Y., Zhang T.G. Expression and clinical significance of Ki-67, E-cadherin, and mesothelin in serous borderline ovarian tumors. Eur. J. Gynaecol. Oncol. 2017; 38(1): 85-90.
- Shiravani Z., Najib F.S., Momtahan M., Robati M., Hajisafari Tafti M., Namazi N. Are ovarian dermoid cysts should be always considered benign? A case series study of different malignant transformation. Indian J. Surg. Oncol. 2020; 11(Suppl 2): 156-8. https://dx.doi.org/10.1007/s13193-020-01159-7
- Öcal İ., Demir S. Prognostic value of Ki67 in borderline mucinous ovarian tumors. Med. J. SDU. 2023; 30(1): 123-9. https://dx.doi.org/10.17343/sdutfd.1187197
Received 17.02.2026
Accepted 20.03.2026
About the Authors
Ummusalimat D. Ibragimova, PhD student, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of Russia, 117997, Russia, Moscow, Ac. Oparin str., 4, amintaeva_umm@mail.ru, https://orcid.org/0009-0008-6984-7193Alexandra V. Asaturova, Dr. Med. Sci., Head of the 1st Pathological Anatomical Department, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of Russia, 117997, Russia, Moscow, Ac. Oparin str., 4, Associate Professor, Department of Pathological Anatomy and
Clinical Pathological Anatomy, Institute of Biology and Pathobiology (IBPCh), Pirogov Russian National Research Medical University, Ministry of Health of Russia,
a.asaturova@gmail.com, https://orcid.org/0000-0001-8739-5209
Irena F. Kozachenko, Dr. Med. Sci., Leading Researcher, Obstetrician-Gynecologist, Gynecological Department, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of the Russia, 117997, Russia, Moscow, Ac. Oparin str., 4, irenakozachenko@rambler.ru,
https://orcid.org/0000-0003-1822-9164
Alina S. Вadlaeva, Senior Researcher, Pathologist, 1st Department of Pathology, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of Russia, 117997, Russia, Moscow, Ac. Oparin str., 4; Associate Professor, Department of Pathological Anatomy and Clinical Pathological Anatomy, Institute of Biology and Pathobiology (IBPCh), Pirogov Russian National Research Medical University, Ministry of Health of Russia,
https://orcid.org/0000-0001-5223-9767
Aleksandra S. Rogozhina, Junior Researcher, Pathologist, 1st Department of Pathology, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of Russia, 117997, Russia, Moscow, Ac. Oparin str., 4, https://orcid.org/0009-0009-6244-1219
Leila V. Adamyan, Academician of the Russian Academy of Sciences, Dr. Med. Sci., Professor, Deputy Director for Research, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of Russia, 117997, Russia, Moscow, Ac. Oparin str., 4; Chief Specialist in Gynecology of the Ministry of Health of Russia; Head of the Department of Reproductive Medicine and Surgery of the Faculty of Postgraduate Education, Russian University of Medicine, Ministry of Health of Russia, adamyanleila@gmail.com, https://orcid.org/0000-0002-3253-4512
Corresponding author: Ummusalimat D. Ibragimova, amintaeva_umm@mail.ru
Similar Articles

