
Liver function parameters in patients with external genital endometriosis and infertility
Gerasimov A.M., Malyshkina D.A., Malyshkina A.I.
Relevance: Inflammation is a key factor in the pathogenesis of endometriosis. To reduce secondary autoaggression, the body utilizes several detoxification systems, the most important of which are the urinary system, the macrophage-macrocytic system, and the liver. Liver function parameters in endometriosis have been understudied.
Objective: To assess liver function based on biochemical blood tests in patients with external genital endometriosis and infertility.
Materials and methods: The study included the patients who were admitted to hospital for therapeutic and diagnostic laparoscopy to determine the causes of infertility. Among them were women with external genital endometriosis (n=36) and the signs of chronic salpingitis (n=36). All patients underwent blood tests for creatinine, total bilirubin, urea, glucose, total protein, ALT, AST, as well as measurements of the liver frailty index (LFI) and De-Ritis ratio (DRR).
Results: Analysis of the relationship between the liver function test results and the stages of endometriosis showed a moderately negative correlation for the DRR (r=-0.49; p<0.05). The LFI values were not associated with the degrees of endometriosis (r=0.23; p>0.05).
Conclusion: Our study demonstrated changes in liver function with the development of endometriosis. Based on the obtained data it is prudent to recommend a comprehensive evaluation of hepatobiliary function in patients with external genital endometriosis, that will enable a multidisciplinary approach and subsequently, a rationale for expanding drug therapy options for these patients.
Authors' contributions: Gerasimov A.M. – the study concept and design, statistical data processing; Malyshkina D.A. – material collection and processing; Gerasimov A.M., Malyshkina D.A. – manuscript writing; Malyshkina A.I. – manuscript editing.
Conflicts of interest: The authors confirm that they have no conflicts of interest to declare.
Funding: The study was carried out without any sponsorship.
Ethical Approval: The study was approved by the Ethics Committee of Ivanovo Research Institute of Maternity and Childhood named after V.N. Gorodkov, Ministry of Health of Russia.
Patient Consent for Publication: The patients have signed informed consent for participation in the study and publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Gerasimov A.M., Malyshkina D.A., Malyshkina A.I. Liver function parameters
in patients with external genital endometriosis and infertility.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (4): 128-133 (in Russian)
https://dx.doi.org/10.18565/aig.2025.316
Keywords
external genital endometriosis
chronic salpingitis
reproductive age
liver function
hyperproliferative diseases
multidisciplinary approach
Currently, it is recognized that inflammation is a central pathophysiological mechanism of endometriosis [1]. Development of the most common endometriosis-associated symptoms, such as pelvic pain, dysuria, dyschezia and infertility can be explained by inflammation with subsequent fibrosis occurrence [2]. Inflammation is associated with local and systemic immunological and biochemical changes, thereby endometriosis is recongnized as a systemic disease [3]. Immune dysregulation occurs in endometriosis involving a cascade of inflammatory cytokines [1] and protease activity [4]. These changes affect not only peripheral blood, but also peritoneal fluid, that causes an abnormal pelvic environment [5]. In particular, these changes cause endometriosis-related infertility and pain [1]. Endometriosis is associated with systemic inflammatory response, that can explain the development of concomitant extragenital diseases – impaired lipid metabolism, central nervous system dysfunction [1], autoimmune diseases, such as systemic lupus erythematosus, multiple sclerosis, rheumatoid arthritis, Crohn's disease, scleroderma, ulcerative colitis, autoimmune thyroid diseases, Sjögren's disease, celiac disease and ankylosing spondylitis, atherosclerosis [6]. Systemic inflammatory response is characterized by activation of a cascade of cytokines and acute-phase inflammatory proteins, which have proteolytic activity, that leads to increased levels of endogenous intoxication [7, 8] and peroxidation [1] specific for endometriosis. There are several major detoxication systems in the body to reduce the level of secondary autoaggression – urinary system, mononuclear phagocyte system (MPS) and liver [8]. Over the past decades, the indicators of kidney function in endometriosis have been explored in detail. The impaired kidney function has been described as decreased glomerular filtration rate and changes in tubular reabsorption [9, 10].
These changes can be explained by the increased load on the excretory function of the kidneys due to excessive accumulation of medium weight molecules. [7, 9]. Also, it has been stated that immune surveillance is involved in almost all stages of the pathogenesis of endometriosis, including formation of systemic inflammatory response [1, 2]. At the same time, the indicators of liver function are understudied, since it has been reported only about the presence of certain alterations in the indicators characterizing the state of this detoxification organ. However, their involvement in the pathogenesis of external endometriosis has not been explained [3]. At the same time, there is convincing evidence on the effectiveness of the interdisciplinary approach the treatment of external genital endometriosis taking into account comorbid conditions [11].
The objective of the study was to assess liver function based on biochemical blood tests in patients with external genital endometriosis and infertility.
Materials and methods
The study included the patients who were admitted to the Department of Endoscopic Surgery, Ivanovo Research Institute of Maternity and Childhood named after V.N. Gorodkov, Ministry of Health of Russia, and underwent therapeutic and diagnostic laparoscopy to determine the causes of infertility. Depending on the results of interventional endoscopy, the patients were divided into 2 groups. Group 1 included the patients (n=36) with external genital endometriosis stages I–IV. Group 2 included the patients (n=36) with the signs of chronic salpingitis. Inclusion criteria were patients with infertility associated with chronic salpingitis, and patients with infertility in combination with external genital endometriosis. Exclusion criteria were both current and previous acute and chronic hepatobiliary pathology, endocrine infertility, and a history of oncological diseases.
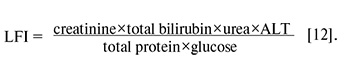
All patients underwent preoperative biochemistry testing to determine the blood levels of creatinine, total bilirubin, urea, glucose, total protein, alanine aminotransferase (ALT), and aspartate aminotransferase (AST) using standard laboratory methods. Based on the obtained parameters, the indices characterizing liver function were calculated. The liver frailty index (LFI) was calculated by the formula:
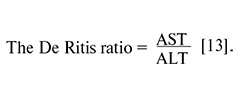
The De Ritis ratio was calculated by the formula:
Statistical analysis
Statistical data processing was performed using Statistica software. Description of quantitative values with non-normal distribution is represented as median (Me) and interquartile range (25%; 75%). The qualitative and categorical data are described using the absolute numbers (n) and relative frequencies (%).
The nonparametric Mann–Whitney U-test was used to assess statistical significance of differences in quantitative parameters between two independent groups: group I – the patients with endometriosis, group II – the patients with pelvic inflammatory disease (PID). Comparisons of categorical variables were performed using chi-squared (χ2) test with Yates' correction or Fisher's exact test for small samples.
The Spearman rank correlation coefficient (r) was calculated to analyze the relationship between the two quantitative traits. In all types of analysis, the differences were considered statistically significant at p<0.05.
Results
The median age of patient in the groups was comparable: 33 (23; 38) years in group I and 32 (26; 39) years in group II.
Evaluation of menstrual function found earlier onset of menarche in women with endometriosis – 12 (11; 13) years compared with women with PID – 13 (11; 14) years, р=0.00. In vast majority of cases, timely onset of menarche was observed in 23/36 (92%) patients in group I and in 24/36 (96%) in group II. Late menarche was in 1/36 (4%) woman with endometriosis. Early menarche was in 1/36 (4%) woman with endometriosis and in 1/36 (4%) woman with PID. Heavy menstrual bleeding was observed more often in women in group I – 22/36 (88%) compared with 1/36 (4%) in the group with PID (р=0.00). Painful periods were also in women with endometriosis – 24/36 (96%) versus 17/36 (68%) in the group with PID (р=0.01). The length of the menstrual cycle was longer in women with PID – 28 days (26; 30) compared with patients with endometriosis – 28 days (24; 30) (р=0.02). Duration of menstruation was similar in both groups – 5 days (4; 7) in women with endometriosis and 5 days (4; 7) in women with PID.
Concomitant gynecological and extragenital pathologies and the frequency of occurrence did not differ between the groups.
All patients in the examined groups complained of infertility. Primary infertility was most often in women with PID – 9/36 (36%) versus 3/36 (12%) patients with endometriosis (р=0.04). At the same time, the average pregnancy rate was 2 (0; 3) per 1 woman with endometriosis, and 1 (0; 3) per 1 woman with PID. Analysis of pregnancy outcomes showed that in 23 patients in group I (1.0; 2) and in 10 women in group II (1.0; 1) (р=0.00) pregnancy ended with childbirth. Abortion rate was significantly higher in the group with endometriosis – 41.6%, whereas in group with PID – 8.3% (р=0.00). Spontaneous miscarriages were in 8.3% of women with endometriosis and in 16.67% of women with PID. In group I, 2.78% of women had one ectopic (tubal) pregnancy, in group II – 8.3%. Stillbirths were in 5.56% of women with endometriosis, and in 16.67% of women with PID. Also, anembryonic pregnancy happened once in 2.78 % of women in the group with PID.
Analysis showed that in most cases blood biochemical parameters in the studied groups were within normal ranges. The results of biochemical tests are represented in the Table.
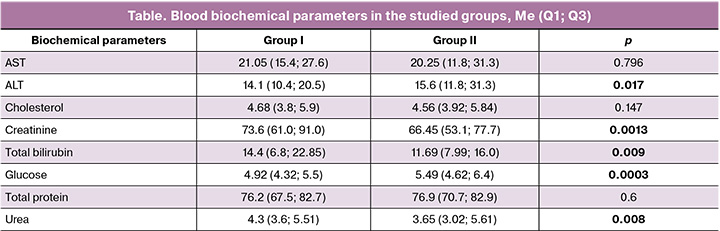
As is shown in the Table, the median values of some parameters differed significantly. In group I, the average levels of ALT and glucose were lower than those in group II (Table). ALT levels ranged from 8.9–25.0 U/L (Group I) to 9.8–32.3 U/L (Group II). Glucose levels ranged 4.2–5.8 mmol/L in group I, while in group II glucose levels ranged 4.5–6.73 mmol/L and exceeded the normal range in 19.4% of cases.
The levels of creatinine, total bilirubin, and urea in women with endometriosis were, on average, higher than those in women with PID (Table). Creatinine levels ranged 51.9–94.0 μmol/L in group I and 42.4–82.0 μmol/L in group II. The levels of total bilirubin ranged 5.7–33.0 μmol/L and 6.56–18.64 μmol/L, respectively. At the same time, in group 1 the levels of total bilirubin were slightly above normal in 13.89% of cases. Urea levels ranged 27.6–8.4 mmol/L and 2.35–8.98 mmol/L, respectively.
Comparison of the indices characterizing liver function also showed the differences between the groups.
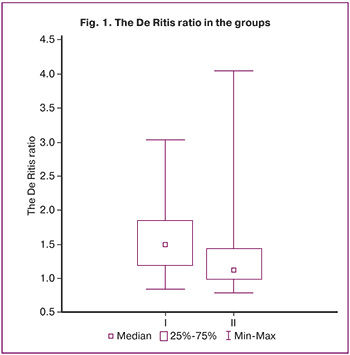
The De Ritis ratio (median 25%; 75%) in group I was 1.49 (1.18; 1.84), whereas in group II it was 1.12 (0.99; 143) and was significantly lower (p=0,0012). The De Ritis ratio ranged 0.84–3.03 in group I, and 0.78 – in group II (Fig. 1). In 52.7% of cases, the values of the De Ritis ratio exceeded Q2 in group II.
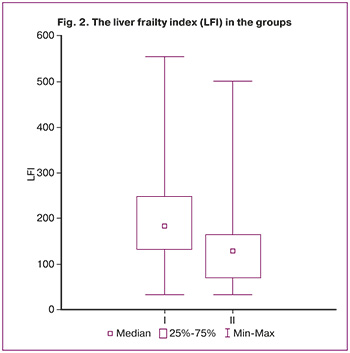
Also, LFI scores significantly differed between the groups. The median (25%; 75%) LFI score in group I was 184.1 (165.3; 239.4), and 128.9 (107.1; 171.5) in group II, that was significantly lower (p=0.0019), just as the De Ritis ratio. LFI scores ranged 32.82–554.17 in group I and 34.42–501.22 in group II (Fig. 2). LFI scores in the group with endometriosis exceeded Q3 in group II in 59.4% of cases.
Analysis of the relationship between the indices characterizing liver function and the degree of invasion of endometriosis showed moderate negative relationship for the de Ritis index: r=-0.49; p<0.05. LFI scores were not associated with the degree of invasion of endometriosis: r=0.23; p>0.05.
Discussion
Currently, the impact of endometriosis on the development of dysfunction of extragenital organs and systems is not in doubt. Almost all authors exploring the problem of endometriosis point to the relationship between endometriosis and systemic somatic diseases [1, 6]. Association between endometriosis and the development of systemic connective tissue disorders, autoimmune processes, kidney diseases, and specific features of neuropsychiatric status has been described [1, 6–8, 14]. These changes in organ systems are explained by the development of systemic inflammatory response, increased endogenous intoxication, specific hormonal imbalance, and microRNA-mediated changes in metabolism, which occur in patients with external endometriosis [1, 7, 15]. The hepatobiliary system, one of the body's primary detoxification systems, is exposed to aggressive effects of autoimmunity developing in endometriosis. This leads to changes in liver function parameters. However, this issue has been insufficiently addressed in medical research literature. Our study analyzed the main biochemical parameters and indices characterizing liver function. The study demonstrated the role of liver function in the development of endometriosis, despite the fact that some biochemical parameters were within the normal range in most cases. It should be noted that LFI scores were significantly higher in the group of patients with endometriosis compared with the group with chronic salpingitis. Given that at the time of patient examination all women in the study groups had neither acute nor previous hepatobiliary pathology, increased LFI scores can be attributed to activated and stress-induced liver function, which is the primary detoxification organ. This is also proved by the increased values of the de Ritis index, characterizing the changes in metabolism of transaminases. Negative correlation between the de Ritis index and the degree of invasion of endometriosis can indirectly indicate a higher cytolytic activity of small lesions of endometrioid heterotopias. The cytolytic activity declines over time, and with high degrees of invasion of endometriosis, perifocal fibrosis occurs, which restricts the invasive capacity of endometriosis [16].
Conclusion
Our study showed the changes in liver function associated with invasion of endometriosis. The obtained data indicate the necessity of a comprehensive examination of the hepatobiliary system in patients with external genital endometriosis, that will enable a multidisciplinary approach, and subsequently justify extended medical therapy for these patients, in particular, reduce possible negative effects of gestagens on liver function, taking into account its involvement in the pathogenesis of external endometriosis.
References
- Park W., Lim W., Kim M., Jang H., Park S.J., Song G., Park S. Female reproductive disease, endometriosis: from inflammation to infertility. Mol. Cells. 2025; 48(1): 100164. https://dx.doi.org/10.1016/j.mocell.2024.100164
- Wang Y., Nicholes K., Shih I.M. The origin and pathogenesis of endometriosis. Annu. Rev. Pathol. 2020; 15: 71-95. https://dx.doi.org/10.1146/annurev-pathmechdis-012419-032654
- Taylor H.S., Kotlyar A.M., Flores V.A. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021; 397(10276): 839-52. https://dx.doi.org/10.1016/S0140-6736(21)00389-5
- Герасимов A.M. Особенности протеазной и антипротеазной активности крови у женщин с наружным эндометриозом. Клиническая лабораторная диагностика. 2005; 3: 14-16. [Gerasimov A.M. Features of protease and antiprotease activity of blood in women with external endometriosis. Clinical Laboratory Diagnostics. 2005; 3: 14-16 (in Russian)].
- Boucher A., Brichant G., Gridelet V., Nisolle M., Ravet S., Timmermans M. et al. Implantation failure in endometriosis patients: etiopathogenesis. J. Clin. Med. 2022; 11(18): 5366. https://dx.doi.org/10.3390/jcm11185366
- Тимофеева Ю.С., Маринкин И.О., Кулешов В.М., Айдагулова С.В. Патогенез боли при эндометриозе. Акушерство и гинекология. 2022; 9: 12-8. [Timofeeva Yu.S., Marinkin I.О., Кuleshov V.M., Aidagulovа S.V. Pathogenesis of pain in endometriosis. Obstetrics and Gynecology. 2022; (9): 12-8 (in Russian)]. https://dx.doi.org/10.18565/aig.2022.9.12-18
- Vazgiourakis V.M., Zervou M.I., Papageorgiou L., Chaniotis D., Spandidos D.A., Vlachakis D., Eliopoulos E., Goulielmos G.N. Association of endometriosis with cardiovascular disease: genetic aspects (review). Int. J. Mol. Med. 2023; 51(3): 29. https://dx.doi.org/10.3892/ijmm.2023.5232
- Герасимов A.M., Посисеева Л.В., Гришанкова М.А. Молекулы средней массы у больных наружным генитальным эндометриозом. Клиническая лабораторная диагностика. 2003; 12: 16. [Gerasimov A.M., Posiseeva L.V., Grishankova M.A. Mean-weight molecules in patients with external genital endometriosis. Clinical Laboratory Diagnostics. 2003; 12: 16 (in Russian)].
- Дубовая А.В. Экзогенная и эндогенная интоксикация. Функциональная система детоксикации. Методы активной детоксикации. Здоровье ребенка. 2011; 5(32): 93-6. [Dubova G.V. Exogenous and endogenous intoxication. Functional detoxication system. Methods of active detoxication. Child's Health. 2011; 5(32): 93-6 (in Russian)].
- Герасимов А.М., Штрыголь С.Ю. Показатели водно-солевого обмена и выделительной функции почек у женщин с бесплодием различной этиологии. Нефрология. 2001; 5(3): 125. [Gerasimov A.M., Shtrygol S.Yu. The parameters of water-salt metabolism and excretory function of the kidneys in women with infertility of different etiology. Nefrologiya. 2001; 5(3): 125 (in Russian)].
- Иваненкова А.М., Добрынина М.Л. Эндометриоз - заболевание гинекологическое или всего организма? Молодежь, наука, медицина. Материалы 65-й Всероссийской межвузовской студенческой научной конференции с международным участием, Тверь, 17-18 апреля 2019 г. 2019: 407-9. [Ivanenkova A.M., Dobrynina M.L. Endometriosis: a gynecological or systemic disease? Youth, science, medicine. Materials of the 65th All-Russian intercollegiate student scientific conference with international participation, Tver, April 17-18, 2019. 2019: 407-9 (in Russian)].
- Шаров М.Н., Чернецова А.С., Адамян Л.В., Мурватов К.Д., Киселёв С.И., Прокофьева Ю.С., Гончаров И.Н. Нейропатическая боль у пациенток с эндометриозом – диагностика и лечение: сравнительное проспективное исследование. Коморбидная неврология. 2024; 1(2): 5-14. [Sharov M.N., Chernetsova A.S., Adamyan L.V., Murvatov K.D., Kiselev S.I., Prokofieva Yu.S., Goncharov I.N. Neuropathic pain in patients with endometriosis – diagnosis and treatment: comparative prospective study. Comorbidity Neurology. 2024; 1(2): 5-14 (in Russian)]. https://dx.doi.org/10.62505/3034-185x-2024-1-2-5-14
- Ярмолинская М.И., Русина Е.И., Семенова В.О., Беганова А.К. Экстрагенитальный эндометриоз: сложности диагностики, современная тактика лечения. Акушерство и гинекология. 2022; 8: 154-62. [Yarmolinskaya M.I., Rusina E.I., Semenova V.O., Beganova A.K. Extragenital endometriosis: diagnostic difficulties, modern treatment policy. Obstetrics and Gynecology. 2022; (8): 154-62 (in Russian)]. https://dx.doi.org/10.18565/aig.2022.8.154-162.
- Масютин В.А., Широков Д.М., Пивоварова Л.П., Нохрин С.П. Оценка лабораторных данных в критических состояниях (трактовка, прогнозирование, медикаментозная коррекция). Пособие для врачей. С.-Пб.; 1999. 79 с. [Masyutin V.A., Shirokov D.M., Pivovarova L.P., Nokhrin S.P. Evaluation of laboratory data in critical conditions (interpretation, forecasting, and drug correction). A guide for physicians. St. Petersburg; 1999. 79 p. (in Russian)].
- Хаджибаев А.М., Туляганов Д.Б., Стопницкий А.А. Ранние предикторы развития острой печеночной недостаточности при острых отравлениях и эндотоксикозах. Вестник экстренной медицины. 2025; 18(2): 35-42. [Khadjibaev A.M., Tulyaganov D.B., Stopnitskiy A.A. Early predictors of acute liver failure in acute poisoning and endotoxemia. Bulletin of Emergency Medicine. 2025; 18(2): 35-42 (in Russian)]. https://dx.doi.org/10.54185/TBEM/vol18_iss2/a4
- Чернецова А.С., Адамян Л.В., Мурватов К.Д., Степанян А.А. Патогенетические аспекты хронической тазовой боли при эндометриозе: перспективы диагностики (обзор литературы). Проблемы репродукции. 2023; 30(4): 112-20. [Chernetsova A.S., Adamyan L.V., Murvatov K.D., Stepanian A.A. Pathogenetic aspects of chronic pelvic pain in endometriosis: diagnostic prospects (literature review). Russian Journal of Human Reproduction. 2024; 30(4): 112-20 (in Russian)]. https://dx.doi.org/10.17116/repro202430041112
- Mamillapalli R., Slutzky R., Mangla A., Gawde N., Taylor H.S. Effect of endometriosis-linked microRNAs on hepatic gene expression. F S Sci. 2025; 6(2): 221-31. https://dx.doi.org/10.1016/j.xfss.2025.02.001
- Vissers G., Giacomozzi M., Verdurmen W., Peek R., Nap A. The role of fibrosis in endometriosis: a systematic review. Hum. Reprod. Update. 2024; 30(6): 706-50. https://dx.doi.org/10.1093/humupd/dmae023
Received 30.10.2025
Accepted 09.04.2026
About the Authors
Aleksey M. Gerasimov, Dr. Med. Sci., Professor, Department of Obstetrics, Gynecology and Medical Genetics, Ivanovo State Medical University, Ministry of Health of Russia, 153012, Russia, Ivanovo region, Ivanovo, Sheremetevsky Ave., 8, +7(903)879-33-50, quake98@mail.ru, eLibrary SPIN: 5656-6210, https://orcid.org/0000-0002-6254-1385Darya A. Malyshkina, PhD, Associate Professor at the Department of Obstetrics, Gynecology and Medical Genetics, Academic Director of the Scientific Society of Students and Young Scientists, Ivanovo State Medical University, Ministry of Health of Russia, 153012, Russia, Ivanovo Region, Ivanovo, Sheremetevsky Ave., 8; Оbstetrician-Gynecologist, Ivanovo Research Institute of Maternity and Childhood named after V.N. Gorodkov, Ministry of Health of Russia, 153045, Russia, Ivanovo region, Ivanovo, Pobedy str., 20, +7(920)377-96-99, nidsumi@mail.ru, eLibrary SPIN: 3738-4508, https://orcid.org/0000-0002-1200-3570
Anna I. Malyshkina, Dr. Med. Sci., Professor, Director, Ivanovo Research Institute of Maternity and Childhood named after V.N. Gorodkov, Ministry of Health of Russia, 153045, Russia, Ivanovo region, Ivanovo, Pobedy str., 20; Head of the Department of Obstetrics, Gynecology and Medical Genetics, Ivanovo State Medical University,
Ministry of Health of Russia, 153012, Russia, Ivanovo Region, Ivanovo, Sheremetevsky Ave., 8, +7(910)982-24-19, anna_im@mail.ru, https://orcid.org/0000-0002-1145-0563
Corresponding author: Aleksey M. Gerasimov, quake98@mail.ru
Similar Articles

