
Interdisciplinary concept of the cardio-reproductive pathway: women's health awareness as a component of cardiovascular event prevention
Salov I.A., Malinova L.I., Malenova A.Yu., Markina M.A., Tolstov S.N.
Objective: To investigate the impact of women’s awareness of their health status on cardiovascular health parameters and long-term cardiovascular outcomes.
Materials and methods: The study was conducted in two stages. The first stage was an observational, cross-sectional study analyzing baseline data from 325 women. The second stage was a prospective cohort study with a median follow-up of 13 years, designed to assess long-term cardiovascular outcomes and adherence to medical follow-up. To assess awareness levels, an original composite Awareness Index (AI) was calculated, incorporating measures of knowledge, behavior, and medical activity. The index comprised five components: (1) knowledge of cardiovascular risk factors and their contribution to cardiovascular disease; (2) implementation of healthy lifestyle practices; (3) self-assessment of quality of life; (4) awareness of reproductive risk factors and their contribution to cardiovascular pathology; and (5) awareness of personal health status and disease-related symptoms.
Results: The study cohort consisted of employed women, predominantly of older working age, with low baseline cardiovascular risk and relatively favorable cardiometabolic profiles. Exploratory factor analysis revealed a two-factor structure reflecting health awareness and cardiometabolic status, which were largely independent. Over the 13-year follow-up period, cardiovascular events were documented in 16.1% of the participants. Awareness indicators were not associated with a statistically significant reduction in cardiovascular event risk, suggesting that awareness alone has limited prognostic value without corresponding behavioral and clinical changes.
Conclusion: These findings suggest that health awareness is an independent but insufficient factor for preventing cardiovascular events among working women. This highlights the need for comprehensive interventions across all stages of the cardio-reproductive pathway that target knowledge acquisition, behavioral modification, and improved access to medical care.
Authors' contributions: Salov I.A., Malinova L.I. – conception and design of the study; Malenova A.Yu., Markina M.A. – data collection and processing; Malinova L.I. – statistical analysis; Malinova L.I., Tolstov S.N. – drafting of the manuscript.
Conflicts of interest: The authors have no conflicts of interest to declare.
Funding: There was no funding for this study.
Ethical Approval: The study was reviewed and approved by the Research Ethics Committee of the Saratov State Medical University named after V.I. Razumovsky, Ministry of Health of Russia.
Disclosure of information on the use of AI: A freely accessible AI tool was used when working with information sources and creating a list of references. All references were checked by the authors.
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Salov I.A., Malinova L.I., Malenova A.Yu., Markina M.A., Tolstov S.N. Interdisciplinary concept of the cardio-reproductive pathway: women's health awareness as a component of cardiovascular event prevention.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (3): 58-67 (in Russian)
https://dx.doi.org/10.18565/aig.2025.382
Keywords
cardio-reproductive pathway
health awareness
cardiovascular risk
prevention
Cardiovascular diseases (CVD) remain the leading cause of mortality among women, contributing substantially to disability, premature mortality, and socioeconomic losses [1]. Despite significant advances in diagnostics, treatment, and prevention, women generally experience less favorable cardiovascular outcomes than men. This disparity is partly attributable to physiological differences, variations in the impact of risk factors, and insufficient consideration of reproductive health within cardiovascular prevention strategies [2, 3]. Hormonal age-related stages, pregnancy, gestational complications, polycystic ovary syndrome, and early menopause represent additional cardiometabolic risk factors that are largely overlooked in traditional cardiovascular risk stratification models [4, 5].
In recent years, the concept of lifelong women's health monitoring has gained traction, framing women's health as a continuous biotemporal continuum in which reproductive events serve as significant predictors of cardiovascular risk [6–8]. Leading cardiology and obstetrics and gynecology scientific and professional communities emphasize the importance of an interdisciplinary approach involving coordinated care between cardiologists and gynecologists throughout a woman's life [9, 10].
A potentially modifiable factor influencing CVD risk is a woman's awareness of her own health status, encompassing knowledge of cardiovascular disease risks and symptoms, understanding the importance of regular medical examinations, making informed decisions in favor of preventive strategies, and maintaining treatment adherence [11]. While the role of awareness has been extensively studied in disease management and treatment adherence, its relationship with long-term cardiovascular outcomes in women remains underexplored, particularly in long-term follow-up studies [12].
Therefore, further research is needed to investigate the influence of women's awareness of their health status—including reproductive characteristics—on objective indicators of cardiometabolic health and long-term cardiovascular outcomes. This need drove the present study, which aimed to assess the impact of women's awareness of their own health status on cardiac health parameters and long-term cardiovascular outcomes.
Materials and methods
This observational analytical study comprised two interconnected phases: (1) a cross-sectional observational study to describe women's awareness of their health status and its associations with cardiometabolic and reproductive characteristics at enrollment; and (2) an observational cohort study, in which participants with a known baseline level of awareness were followed to assess the association between this parameter and the development of cardiovascular outcomes.
Sample formation. Women were enrolled from employees of two medium-sized commercial-industrial enterprises not exposed to regulated occupational hazards. The inclusion criteria were as follows: availability of data on socio-educational status and gynecological history, and consent for data processing, including participation in follow-up (for the cohort group). The exclusion criteria at study initiation were as follows: pregnancy or lactation; active oncological disease; acute infectious and autoimmune diseases in the exacerbation phase; and mental conditions that precluded adequate participation in the study. A total of 345 women were examined in the cross-sectional phase, with 325 included in the final sample.
Data were collected using direct questionnaires, analysis of medical records, and laboratory and instrumental examinations. The following parameter groups were analyzed: (1) sociodemographic characteristics (age, marital status, educational level, and type of occupation); (2) behavioral characteristics and lifestyle (physical activity level [minutes/week], sleep duration [hours/day], presence of harmful habits [smoking and alcohol consumption], dietary preferences, and frequency of medical check-ups); (3) gynecological history (age at menarche and menopause, pregnancy complications [preeclampsia, gestational diabetes, and preterm birth], presence of polycystic ovary syndrome and endometriosis, and surgical interventions); and (4) cardiometabolic parameters.
The cardiometabolic parameters included blood pressure (BP, repeated office measurements according to national guidelines and ESC/ESH 2018, 2025, using a certified automatic sphygmomanometer, accuracy class BB), serum levels of total cholesterol, triglycerides, high-density lipoprotein (HDL), low-density lipoprotein (LDL), glucose, creatinine, and uric acid. Body mass index (BMI) and waist-to-hip ratio (WHR) were calculated. Glomerular filtration rate was estimated using the modified CKD-EPI (2021) equation.
Assessment of health awareness. An author-derived composite awareness index (AI) was used, incorporating assessments of knowledge, behavior, and medical activity. The index comprised five functional domains: (1) knowledge of risk factors and their contribution to the development of cardiovascular pathology; (2) actual implementation of "healthy lifestyle" practices; (3) self-assessment of quality of life; (4) knowledge of reproductive risk factors and their contribution to the development of cardiovascular pathology; and (5) knowledge of one's own health status and presence of disease symptoms. The selection of functional domains was based on the traditional approach of analogous projects (HEALTH LITERACY EUROPE, https://www.healthliteracyeurope.net/ [accessed 20 December 2025]). Each domain was normalized to a range of 0–100 points.
For the analysis, two indices were used: composite (AIcomposite), representing the arithmetic mean across all domains, and weighted (AIweighted), calculated using the following formula:
AIweighted =(0.25×KZ)+(0.25×OZ)+(0.15×SZ)+(0.15×RZ)+(0.1×DZ),
where KZ – awareness of cardiovascular risk factors;
OZ – actual implementation of "healthy lifestyle" practices;
SZ – self-assessment of quality of life;
RZ – awareness of reproductive risks;
DZ – knowledge of one's own health status and presence of disease symptoms.
To assess individual baseline risk for the research objective, the 10-year risk of fatal cardiovascular events was calculated for all participants using a survival model based on the Weibull function, as described previously [13].
Participants for whom follow-up health information was available constituted the observational cohort group and were included in the second phase of the study. The primary endpoint was the development of a cardiovascular event, including myocardial infarction, ischemic or hemorrhagic stroke, or hospitalization for acute coronary syndrome. The secondary endpoints were as follows: frequency of visits to a cardiologist and gynecologist; hospitalizations for cardiovascular reasons; and initiation or modification of pharmacotherapy. Outcome information was collected based on medical records and questionnaire data.
The study was conducted in accordance with the principles of evidence-based medicine and complied with all the requirements of the Declaration of Helsinki and the National Standard of the Russian Federation, "Good Clinical Practice (GCP)" (GOST R52379-2005). The study protocol was approved by the local ethics committee, and all participants provided informed voluntary consent to participate. The personal data were de-identified.
Statistical analysis
Individual participant data were recorded according to the study protocol and analyzed anonymously. Statistical analysis was performed using JASP software (version 0.95.4). Missing data were tolerated up to 5%. Quantitative variables are described using the median and interquartile range (IQR). Categorical variables are presented as n/N (%), where N is the number of observations with available data for the corresponding variable. Missing values were not included in the percentage calculations. The normality of the distribution of quantitative variables was assessed using the Shapiro–Wilk test. Non-parametric methods were used to test statistical hypotheses because of deviations from a normal distribution and/or the ordinal nature of the data analyzed.
Comparisons between two independent groups were performed using the Mann–Whitney U test. For comparisons involving more than two groups, the Kruskal–Wallis one-way analysis of variance was used, followed by pairwise comparisons if an overall significance was found; the Holm correction was applied for multiple comparisons. The level of statistical significance was set at p<0.05.
If the amount of missing data exceeded 5%, an analysis was performed using Little's test. If the hypothesis that data were Missing at Random (MAR) could not be rejected, multiple imputation was used to handle missing values. Twenty imputations were performed, followed by pooling of estimates. A generalized linear model with a binomial distribution and a logit link function was used to assess the association between participants' awareness and the development of cardiovascular events. Model comparison was performed using the likelihood ratio test. Differences were considered statistically significant at p<0.05. Exploratory factor analysis was conducted using the principal axis method with oblique rotation, allowing for factor correlation.
Results
Characteristics of the study population
Overall, the assembled sample of employed women was relatively "aged," with a median age of 50 years (IQR, 16). Of the participants, 178/324 (54.9%) were married (including cohabiting partnerships), whereas 63/324 (19.4%) had never been married or in a long-term relationship. The vast majority held higher education (138/324; 42.6%) or vocational/complete secondary specialized education (127/324; 39.2%). At the time of study enrollment, 174/321 (54.2%) participants were postmenopausal. In 74.6% of cases (138/185), menopause resulted from age-related involution; in 16.7% of participants (31/185), it was induced menopause with preserved ovaries. The overwhelming majority (299/317; 94.3%) of women were not receiving hormone replacement therapy.
Notably, the frequency of gynecological consultations was low: 111/311 (35.8%) women had not seen a gynecologist for more than one year, and 55/311 (17.7%) had not done so within the preceding five years, despite a verified gynecological diagnosis in 180/311 (57.9%) participants. The most prevalent diagnoses in the sample were uterine leiomyoma/fibromyoma (ICD-10 codes D25.0–D25.9), observed in 66/311 (21.2%) cases, postmenopausal atrophic vaginitis (N95.2), 33/311 (10.6%), and endometriosis (N80.0–N80.9), 38/311 (12.2%).
As shown in Table 1, the participants exhibited low overall cardiovascular risk and a moderate level of health awareness. As anticipated, arterial hypertension was the most frequent form of cardiovascular pathology: combined systolic-diastolic hypertension was present in 6/325 (19.4%) participants, and isolated systolic or diastolic hypertension was present in 46/325 (14.2%). Additionally, gestational hypertension was identified in 53/282 (18.8%) participants.

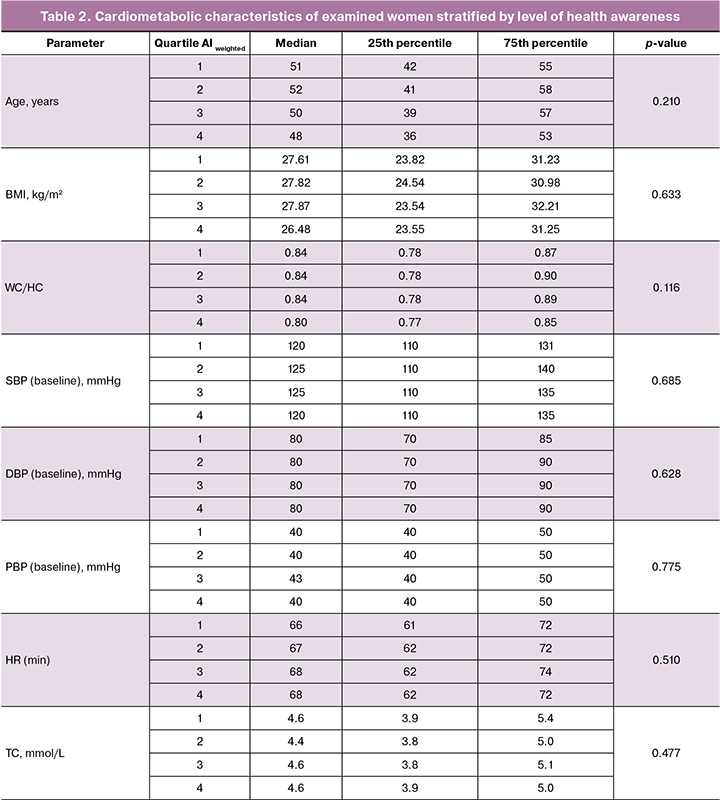
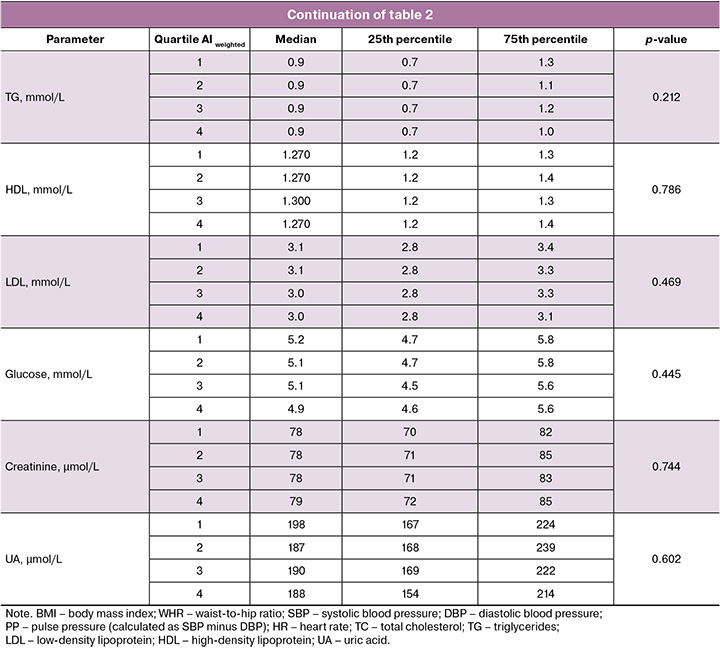
Health awareness and cardiometabolic parameters
The study sample demonstrated relative cardiometabolic well-being (Table 2). Trends toward increasing creatinine levels, decreasing age, and waist-to-hip ratio with higher awareness levels were neither clinically nor statistically significant.
Cardiovascular outcomes
During the follow-up period (median: 13 years), a substantial loss to follow-up occurred; the response rate was 19.1% (62/325). Although this rate is comparatively low for observational studies, it reflects the considerable challenge in maintaining participant contact over such an extended interval. Nevertheless, analyses of missing data patterns and the application of statistical methods for bias correction support the validity of using these results to evaluate associations between awareness parameters and cardiovascular outcomes within the observed cohort.
During follow-up, most respondents (31/29 (52.5%)) reported a reduction in daily walking duration. Normotension persisted in 46.7% of cases (29/62). Among participants receiving antihypertensive therapy, target blood pressure levels were achieved in 27.4% (17/62), while "new-onset" arterial hypertension developed in 4/62 participants (6.5%).
A cardiovascular event (stroke, transient ischemic attack, or acute coronary syndrome) occurred in 10/62 (16.1%) participants during follow-up. According to a generalized linear model with binomial distribution and logit link function, the inclusion of awareness measures (both composite and weighted awareness index) did not yield a statistically significant improvement in predicting cardiovascular event occurrence over the 13-year observation period (χ²=2.55; p=0.11 and χ²=3.06; p=0.08, respectively). Given the continuous nature of exposure, the low event count, and the absence of a biologically justified awareness threshold, calculation of relative risk lacked independent interpretive value and was therefore not performed.
Among women who experienced cardiovascular events during follow-up, there was a higher prevalence of self-reported complicated pregnancy histories, including gestational hypertension and preeclampsia, as well as earlier menopause onset. Owing to the limited number of events, these differences did not reach statistical significance; however, the observed trends align with the contemporary understanding of reproductive factors as early markers of elevated cardiovascular risk in women.
To assess potential selection bias, a comparative analysis of baseline characteristics was conducted between participants retained in the cohort follow-up phase and those for whom long-term outcome data were unavailable. The groups did not differ significantly regarding median age, educational attainment, baseline overall cardiovascular risk, or values of the composite and weighted Awareness Index (p>0.05 for all comparisons). However, participants who remained in contact throughout the follow-up period exhibited a tendency toward more regular outpatient medical supervision and higher healthcare engagement, suggesting a modest selection bias toward more compliant respondents.
Additional (exploratory) analysis
Exploratory factor analysis confirmed sampling adequacy based on the Kaiser–Meyer–Olkin coefficient (KMO=0.64) and a significant result from Bartlett's test of sphericity (p<0.001). The number of factors was determined using parallel analysis. A two-factor structure was retained in the final model, accounting for approximately 81% of the total variance among variables. Factor loadings ≥ 0.40 were considered interpretable (Table 3).
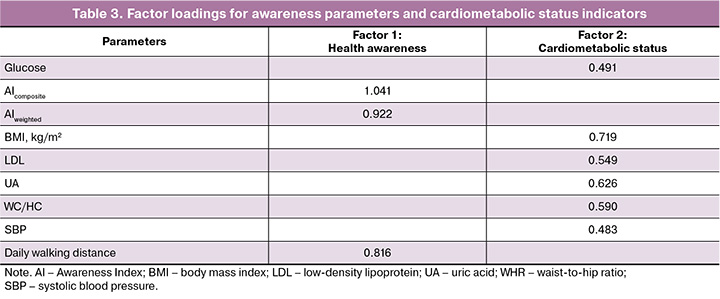
The first factor exhibited high loadings for variables reflecting health awareness (AIweighted, AIcomposite, and daily walking duration) and explained 29% of the total variance. The second factor comprised variables associated with cardiometabolic health (BMI; LDL; UA; WHR; SBP) and accounted for 52% of the variance (Table 3). Collectively, the two-factor structure explained approximately 81% of the total variance among the included variables. Communalities for most variables exceeded 0.30, indicating a satisfactory explanatory contribution of the extracted factors to the variance of baseline measurements. Oblique rotation revealed a weak negative correlation between factors (r=-0.07), supporting their practical independence and the absence of a shared latent factor.
Discussion
The present study enabled the evaluation of sociodemographic, reproductive, behavioral, and cardiometabolic factors in women within the context of the cardio-reproductive pathway. Another strength was the objective assessment of women's awareness of their own health status through calculated awareness indices (AI).
However, the analysis did not reveal a statistically significant association between the level of awareness, cardiometabolic parameters, and incidence of cardiovascular events in the studied cohort of working-age women. This somewhat unexpected result warrants careful consideration.
First, knowledge of one's health status does not always translate into proactive steps toward improvement, and changes in behavior do not guarantee complete cardiovascular well-being. It is possible that the AI used does not capture aspects of "health literacy" that lead to sustained lifestyle modifications or treatment adherence (i.e., functional health literacy, self-management, and decision-making skills). This aligns with the findings from studies on health literacy in cardiovascular diseases. A systematic review and meta-analysis showed that low health literacy is associated with increased mortality, more frequent hospitalizations, and poorer quality of life. However, evidence regarding population-level prevention and outcomes in healthy or relatively healthy groups remains limited and inconsistent [14].
Second, the pathway from awareness to final outcomes is complex, involving multiple intermediate stages: knowledge → motivation → behavior → modification of cardiovascular continuum components (blood pressure, lipid profile, body weight, etc.) → vascular remodeling, inflammation, atherogenesis, and thrombosis → clinical cardiovascular events. If the behavioral change link is weak (e.g., due to socioeconomic factors, limited access to healthy nutrition, lack of time for routine health examinations, or low motivation), the effect on clinical outcomes may be attenuated. In a homogeneous population with relatively favorable socioeconomic status and initially low overall cardiovascular risk, as in our study, the variability in AI – and therefore in functional health literacy – was likely too small to detect an effect on outcomes, even over a prolonged follow-up period.
Third, the observational design and limited statistical power (due to the rarity of events) may have been insufficient to detect weak but clinically meaningful associations. Identifying such relationships may require a larger cohort or a stratified approach (e.g., identifying subgroups with a high reproductive burden, unfavorable metabolic profiles, and low adherence).
Nevertheless, the undeniable importance of key determinants of cardiovascular risk directs us to the concept of the cardio-reproductive pathway. Our study included a detailed collection of gynecological and reproductive history, including information on menarche and menopause, pregnancy complications (preeclampsia, gestational diabetes, and preterm birth), as well as endocrine-gynecological and surgical conditions. Such factors are increasingly recognized as early indicators of future cardiovascular risk – the so-called female-specific risk trajectory.
It should be emphasized that despite the limitations of the cohort study, the cross-sectional component conducted in a sample of 325 women demonstrated high methodological reliability. The identified independence between awareness and cardiometabolic status is of independent scientific interest and confirms the need to distinguish between health knowledge and objective biological risk when developing preventive strategies.
Numerous large cohort studies and meta-analyses have shown that pregnancy complications, particularly gestational diabetes mellitus and hypertensive disorders of pregnancy (gestational hypertension and preeclampsia), are associated with a significantly increased long-term risk of CVD [15–17].
In a large national retrospective cohort study, hypertensive disorders of pregnancy were associated with an increased risk of arterial hypertension and CVD: women with one episode of preeclampsia had a hazard ratio (HR) of 1.29 for CVD after childbirth, and with recurrent episodes up to an HR of 1.53; the risk of arterial hypertension was particularly high (HR≈4–6) [18]. Moreover, a genetic epidemiological analysis demonstrated that a genetic predisposition to hypertensive disorders of pregnancy is associated with an increased risk of coronary heart disease, stroke, heart failure, and atrial fibrillation [19]. This strengthens the rationale for considering pregnancy complications not merely as markers but potentially as part of the causal pathway leading to CVD.
Thus, a cardio-reproductive pathway emerges through which long-term cardiovascular risk is established in young and middle-aged women. These data underscore the need to recognize pregnancy and its outcomes as "stress tests" of the female cardiovascular system; incorporate reproductive factors into the assessment of long-term cardiovascular risk; develop recommendations for screening and long-term monitoring of women with adverse reproductive histories; and implement early preventive interventions and targeted programs aimed at controlling metabolic and vascular risk factors. In this context, the design of our study – with careful collection of reproductive history and prolonged follow-up – was particularly justified. Even if awareness index (AI) was not identified as a predictor, reproductive and biological factors may act as key determinants of risk, as supported by the growing body of evidence.
An important practical implication is that prevention programs for women should combine education with practical support, such as strengthening motivation, ensuring access to healthy lifestyle options, providing regular monitoring, and implementing structured multimodal pregnancy care.
Study limitations
A major limitation of the present study was the substantial loss to follow-up during the cohort stage. Despite analyzing the missing data and applying bias-correction methods, the influence of this factor on the assessment of associations between awareness and cardiovascular outcomes cannot be completely excluded. The small absolute number of cardiovascular events (n=10) limited the statistical power of the analysis. Under these conditions, the absence of statistically significant associations cannot be interpreted as evidence of true absence. An additional limitation is the use of an author-developed composite AI that did not undergo external validation in independent samples.
The obtained results were interpreted considering the study limitations, including the observational design, limited cohort size, low event rate, and use of the author-developed AI. Therefore, the conclusions should be considered hypothesis-generating and define directions for future research. Promising areas include the development and validation of tools for assessing functional health literacy and the study of complex interventions combining educational, behavioral, and clinical components of CVD prevention in women within the context of the cardio-reproductive pathway.
Conclusion
The results suggest that women's awareness of their own health status is a potentially important, yet seemingly insufficient when considered alone, component of CVD prevention among working-age women. Within the framework of the present study, no convincing evidence was found of its independent association with long-term cardiovascular outcomes; however, this does not exclude the possibility of an indirect influence of awareness through behavioral and clinical mechanisms.
Overall, the findings support the feasibility of comprehensive preventive strategies within the cardio-reproductive pathway that combine educational, behavioral, and medical interventions at different stages of a woman's life. Such strategies should aim not only to increase knowledge but also to promote sustainable lifestyle changes and ensure regular medical follow-up.
References
- Mehta L.S., Velarde G.P., Lewey J., Sharma G., Bond R.M., Navas-Acien A. et al. Cardiovascular disease risk factors in women: the impact of race and ethnicity: a scientific statement from the American heart association. Circulation. 2023; 147(19): 1471-87. https://dx.doi.org/10.1161/CIR.0000000000001139
- Gauci S., Cartledge S., Redfern J., Gallagher R., Huxley R., Lee C.M.Y. et al. Biology, bias, or both? The contribution of sex and gender to the disparity in cardiovascular outcomes between women and men. Curr. Atheroscler. Rep. 2022; 24(9): 701-8. https://dx.doi.org/10.1007/s11883-022-01046-2
- Mahowald M.K., Esmail K., Ezzeddine F.M., Choi C., Mieszczanska H., Velarde G. Sex disparities in cardiovascular disease. Methodist Debakey Cardiovasc. J. 2024; 20(2): 107-19. https://dx.doi.org/10.14797/mdcvj.1328
- O'Kelly A.C., Michos E.D., Shufelt C.L., Vermunt J.V., Minissian M.B., Quesada O. et al. Pregnancy and reproductive risk factors for cardiovascular disease in women. Circ. Res. 2022; 130(4): 652-72. https://dx.doi.org/10.1161/CIRCRESAHA.121.319895
- Kim C., Catov J., Schreiner P.J., Appiah D., Wellons M.F., Siscovick D. et al. Women's reproductive milestones and cardiovascular disease risk: a review of reports and opportunities from the CARDIA study. J. Am. Heart Assoc. 2023; 12(5): e028132. https://dx.doi.org/10.1161/JAHA.122.028132
- Lindley K.J. Introduction to the compendium on lifelong care in women: applying a sex- and gender-lens to practice. Circ. Res. 2025; 136(6): 551-2. https://dx.doi.org/10.1161/CIRCRESAHA.125.326335
- Ivey S.L., Hanley H.R., Taylor C., Stock E., Vora N., Woo J. et al. Early identification and treatment of women's cardiovascular risk factors prevents cardiovascular disease, saves lives, and protects future generations: policy recommendations and take action plan utilizing policy levers. Clin. Cardiol. 2022; 45(11): 1100-6. https://dx.doi.org/10.1002/clc.23921
- Lassi Z.S., Wade J.M., Ameyaw E.K. Stages and future of women's health: a call for a life-course approach. Womens Health (Lond). 2025; 21: 17455057251331721. https://dx.doi.org/10.1177/17455057251331721
- De Backer J., Haugaa K.H., Hasselberg N.E., de Hosson M., Brida M., Castelletti S. et al. 2025 ESC Guidelines for the management of cardiovascular disease and pregnancy. Eur. Heart J. 2025; 46(43): 4462-568. https://dx.doi.org/10.1093/eurheartj/ehaf193
- Mehta L.S., Warnes C.A., Bradley E., Burton T., Economy K., Mehran R. et al. Cardiovascular considerations in caring for pregnant patients: a scientific statement from the american heart association. Circulation. 2020; 141(23): e884-e903. https://dx.doi.org/10.1161/CIR.0000000000000772
- Bairey Merz C.N., Andersen H., Sprague E., Burns A., Keida M., Walsh M.N. et al. Knowledge, attitudes, and beliefs regarding cardiovascular disease in women: the women's heart alliance. J. Am. Coll. Cardiol. 2017; 70(2): 123-32. https://dx.doi.org/10.1016/j.jacc.2017.05.024
- Beussink-Nelson L., Baldridge A.S., Hibler E., Bello N.A., Epps K., Cameron K.A. et al. Knowledge and perception of cardiovascular disease risk in women of reproductive age. Am. J. Prev. Cardiol. 2022; 11: 100364. https://dx.doi.org/10.1016/j.ajpc.2022.100364
- Малинова Л.И., Долотовская П.В., Фурман Н.В., Толстов С.Н., Клочков В.А., Денисова Т.П. Оценка метаболического бремени в свете концепции сосудистого старения при артериальной гипертензии (исследование трудоспособного населения крупного промышленного центра). Артериальная гипертензия. 2023; 29(1): 24-37. [Malinova L.I., Dolotovskaya P.V., Furman N.V., Tolstov S.N., Klochkov V.A., Denisova T.P. Assessment of metabolic burden in the light of the concept of vascular aging in arterial hypertension (study of the working-age population of a large industrial center). Arterial Hypertension. 2023; 29(1): 24-37 (in Russian)]. https://dx.doi.org/10.18705/1607-419X2023-29-1-24-37
- Kanejima Y., Shimogai T., Kitamura M., Ishihara K., Izawa K.P. Impact of health literacy in patients with cardiovascular diseases: a systematic review and meta-analysis. Patient Educ. Couns. 2022; 105(7): 1793-800. https://dx.doi.org/10.1016/j.pec.2021.11.021
- Kramer C.K., Campbell S., Retnakaran R. Gestational diabetes and the risk of cardiovascular disease in women: a systematic review and meta-analysis. Diabetologia. 2019; 62(6): 905-14. https://dx.doi.org/10.1007/s00125-019-4840-2
- Crump C., Sundquist J., Sundquist K. Adverse pregnancy outcomes and long-term risk of heart failure in women: national cohort and co-sibling study. JACC Heart Fail. 2025; 13(4): 589-98. https://dx.doi.org/10.1016/j.jchf.2024.11.004
- Oliver-Williams C., Stevens D., Payne R.A., Wilkinson I.B., Smith G.C.S., Wood A. Association between hypertensive disorders of pregnancy and later risk of cardiovascular outcomes. BMC Med. 2022; 20(1): 19. https://dx.doi.org/10.1186/s12916-021-02218-8
- Hassdenteufel K., Muller M., Gutsfeld R., Goetz M., Bauer A., Wallwiener M. et al. Long-term effects of preeclampsia on maternal cardiovascular health and postpartum utilization of primary care: an observational claims data study. Arch. Gynecol. Obstet. 2023; 307(1): 275-84. https://dx.doi.org/10.1007/s00404-022-06561-w
- Taageby Nielsen S., Luo J., Tybjaerg-Hansen A., Iversen K., Bundgaard H., Qvist Thomassen J. et al. Preeclampsia, gestational hypertension, and cardiovascular disease risk: a genetic epidemiological study. Eur. Heart J. 2025; 46(41): 4316-25. https://dx.doi.org/10.1093/eurheartj/ehaf565
Received 23.12.2025
Accepted 12.02.2026
About the Authors
Igor A. Salov, Dr. Med. Sci., Professor, Honored Doctor of the Russian Federation, Professor at the Department of Obstetrics and Gynecology, Faculty of Medicine,Saratov State Medical University named after V.I. Razumovsky, Ministry of Health of the Russian Federation, 410012, Russia, Saratov, B. Kazachya str., 112, salov.i.a@mail.ru,
https://orcid.org/0000-0002-1926-5418
Lidia I. Malinova, Dr. Med. Sci., Associate Professor at the Department of Therapy with courses of cardiology, functional diagnostics and geriatrics, Saratov State Medical University named after V.I. Razumovsky, Ministry of Health of the Russian Federation, 410012, Russia, Saratov, B. Kazachya, 112, lidia.malinova@yandex.ru,
https://orcid.org/0000-0002-0951-9314
Anastasia Yu. Malenova, Resident at the Department of Therapy with courses of cardiology, functional diagnostics and geriatrics, Saratov State Medical University named
after V.I. Razumovsky, Ministry of Health of the Russian Federation, 410012, Russia, Saratov, B. Kazachya str., 112, anastysa2000@yandex.ru,
https://orcid.org/0009-0006-2891-8501
Maria A. Markina, Resident at the Department of Therapy with courses in cardiology, functional diagnostics and geriatrics, Saratov State Medical University
named after V.I. Razumovsky, Ministry of Health of the Russian Federation, 410012, Russia, Saratov, B. Kazachya str., 112, markina2626@gmail.com
Sergey N. Tolstov, Dr. Med. Sci., Associate Professor at the Department of Therapy with courses of cardiology, functional diagnostics and geriatrics, Saratov State Medical University named after V.I. Razumovsky, Ministry of Health of the Russian Federation, 410012, Russia, Saratov, B. Kazachya str., 112, tolstovsn@mail.ru,
https://orcid.org/0000-0002-4546-9449
Corresponding author: Sergey N. Tolstov, tolstovsn@mail.ru
Similar Articles

