
Surgical strategy for simultaneous deep endometriosis involving the rectum and ileocecal region
Goncharov A.L., Bekova M.A., Kalinina A.A., Kabeshov A.M., Levshin F.A., Tsechoeva Zh.R.
Intestinal endometriosis is diagnosed in 30% of patients with deep endometriosis (DE). Simultaneous involvement of both the right and left colonic segments poses a significant technical challenge, requiring surgeons to choose between staged sequential procedures and a single, simultaneous intervention.
Objective: To evaluate the feasibility, safety, and efficacy of simultaneous (single-stage) laparoscopic bowel resections in patients with DE affecting both sides of the intestinal tract.
Materials and methods: A retrospective analysis of surgical outcomes was conducted in patients who underwent simultaneous laparoscopic resection for multifocal intestinal endometriosis. A total of 110 patients with DE who required resection of one or more bowel segments were included in the study. Combined right- and left-sided intestinal involvement was identified in 35 of 110 (31.8%) patients with DE. The parameters assessed included operative duration, complication rate, and length of the recovery period.
Results: This study confirmed that simultaneous laparoscopic interventions for combined right- and left-sided intestinal involvement are technically feasible, safe, and effective. The mean operative time was 283±110 min, and the mean early recovery period was 3.45±0.95 days (range: 2–6 days). Postoperative complications were recorded in four of 35 (11.4%) patients. One case involved suppuration of the periumbilical postoperative wound, and the other involved intestinal hemorrhage from the sigmoidorectal anastomosis, requiring emergency colonoscopy and clipping. No anastomotic dehiscence of the right colonic segment was observed in any patient in the study group. In one patient, clinical signs of sigmoidorectal anastomotic dehiscence involving less than one-quarter of the circumference developed on postoperative day 5 following simultaneous resection of the rectum and ileocecal region. In one additional case, suture line failure following ureteral repair necessitated nephrostomy.
Conclusion: A comprehensive multidisciplinary approach utilizing contemporary surgical technologies enables optimal perioperative outcomes with a low risk of complications. The data obtained indicate the promise of further development and clinical implementation of simultaneous resection techniques for managing advanced forms of deep endometriosis.
Authors' contributions: Goncharov A.L., Bekova M.A., Kabeshov A.M., Levshin F.A. – conception and design of the study; Goncharov A.L., Bekova M.A., Kalinina A.A., Kabeshov A.M., Levshin F.A., Tsechoeva Zh.R. – data collection and processing; Kalinina A.A., Tsechoeva Zh.R. – statistical analysis; Goncharov A.L., Kalinina A.A., Kabeshov A.M., Tsechoeva Zh.R. – drafting of the manuscript.
Conflicts of interest: The authors have no conflicts of interest to declare.
Funding: There was no funding for this study.
Ethical Approval: The study was reviewed and approved by the Research Ethics Committee of the Central Clinical Hospital with Polyclinic of the Administrative Directorate of the President of the Russian Federation.
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Goncharov A.L., Bekova M.A., Kalinina A.A., Kabeshov A.M., Levshin F.A., Tsechoeva Zh.R.
Surgical strategy for simultaneous deep endometriosis involving the rectum and ileocecal region.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (4): 106-113 (in Russian)
https://dx.doi.org/10.18565/aig.2025.362
Keywords
intestinal endometriosis
segmental bowel resection
simultaneous resection
deep endometriosis
laparoscopic surgical strategy
Endometriosis is a prevalent chronic condition that substantially impairs the quality of life of women of reproductive age [1]. The most severe form of endometriosis is deep endometriosis (DE). Notably, a unified definition and classification of DE – particularly in domestic [Russian-language] literature – remains a subject of ongoing debate. The term is generally understood to encompass extensive retrocervical lesions involving the distal large bowel, urinary tract structures, and pelvic fatty tissue spaces [2, 3]. The current edition of the International Classification of Diseases (ICD-11) designates intestinal endometriosis as a distinct nosological entity [4]. This disease variant occurs in 3–37% of patients with endometriosis [5]. According to contemporary data, up to 30% of intestinal endometriosis cases are localized to the right-sided segments (ileocecal region, appendix, cecum, and ileum) [6], which accounts for the polymorphic clinical presentation of the disease.
The pathogenesis involves proliferation and transmural infiltration of the bowel wall by endometriotic implants, triggering a fibrotic response [7]. Under the influence of recurrent cyclic hormonal stimulation, this process ultimately results in the formation of strictures and dense adhesions. This mechanism explains the broad symptomatic spectrum, ranging from complete absence of symptoms and chronic abdominal or pelvic pain, nausea, vomiting, diarrhea, and rectal bleeding, to the presentation of acute surgical pathology (bowel obstruction, intussusception, or intestinal perforation) that may be precipitated by stenosing involvement of the ileocecal region. A critical diagnostic hallmark is the clear association between symptomatology and the menstrual cycle.
Topographic diagnosis of intestinal endometriosis is challenging, resulting in delayed diagnosis and untimely initiation of treatment. Diagnostic laparoscopy, previously regarded as the diagnostic "gold standard" for endometriosis, has now largely ceded this role to non-invasive imaging modalities – expert-level ultrasound and magnetic resonance imaging (MRI) – and its application is currently confined to definitive diagnostic verification and surgical treatment [8]. These characteristics necessitate extending diagnostic attention to the entire abdominal cavity at the time of diagnosis to exclude multifocal intestinal involvement, in full accordance with the current IDEA consensus recommendations [9].
Currently, the extent of bowel surgery for endometriotic involvement varies with respect to the radicality of the intestinal wall. The choice of technique depends on the linear dimensions of the endometriotic infiltrate and the depth of its invasion into the bowel wall, as determined preoperatively. Shaving refers to the excision of endometriotic infiltrates within healthy tissue margins without entering the bowel lumen. Its indication is involvement with a contact area ("footprint") of up to 1 cm and an invasion depth of no more than 5 mm [10]. Disc resection, applied for a solitary endometriotic nodule ≤ 3 cm in size and involvement of less than one-third of the bowel circumference, entails full-thickness excision of the infiltrate as a "disc" of the bowel wall, with reconstruction of the defect using a stapling device or a sealing double-layer suture. Segmental resection with anastomosis formation remains the method of choice for transmural endometriotic bowel involvement by nodules ≥ 3 cm extending to more than one-third of the circumference, for multiple lesions, and for stenosing processes, providing maximum surgical radicality [11].
Recurrence rates and complication risks associated with varying extents of surgery for the most typical patterns of rectosigmoid involvement have been well characterized [12–15]. Advances in diagnostic methods and surgical techniques have made simultaneous (single-stage) procedures feasible, enabling the correction of combined lesions across multiple bowel segments. Accordingly, the technical aspects, efficacy, safety, and long-term outcomes of this surgical approach for advanced forms of DE merit thorough investigation.
This study aimed to evaluate the feasibility, safety, and efficacy of simultaneous (single-stage) laparoscopic bowel resections for the treatment of patients with DE affecting both sides of the intestinal tract.
Materials and methods
Between 2018 and 2025, 110 patients underwent surgical treatment for DE involving resection of one or more bowel segments at the Central Clinical Hospital with a Polyclinic of the Administrative Directorate of the President of the Russian Federation and the Hospital of Fomin Michurinsky Clinic, LLC. Preoperatively, all patients underwent a comprehensive evaluation, including clinical and laboratory investigations, pelvic and abdominal ultrasonography, pelvic magnetic resonance imaging, and consultations with a gynecologist, colorectal surgeon, and, when indicated, a urologist and reproductive medicine specialist. A multidisciplinary team determined the surgical strategy based on the clinical presentation, extent of disease, and patient's reproductive intentions. All procedures were performed by a multidisciplinary surgical team comprising gynecologists, colorectal surgeons, and urologists, when required.
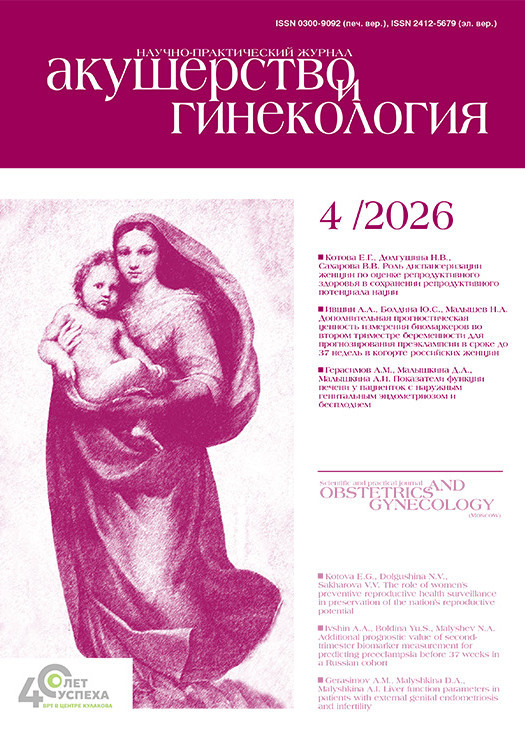
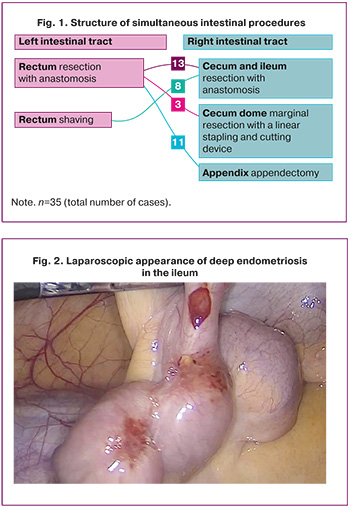
The patients’ ages ranged from 29 to 51 years (mean age, 34.82±4.71 years). The body mass index ranged from 17.16 to 31.30 kg/m² (mean, 21.20±3.03 kg/m²). Combined involvement of both the right and left colonic segments was identified in 35 of 110 patients (31.8%) with DE. In 13 of these 35 cases (37.14%), deep endometrial infiltration involved the ileocecal region and rectum, necessitating simultaneous resection of the cecum and ileum, segmental rectosigmoid resection, and construction of two intestinal anastomoses (Fig. 1). In 8 of the 35 cases (22.85%), the predominant endometriotic involvement was localized to the right colonic segments, specifically the cecum and ileum (Figure 2), while lesions of the pelvic peritoneum and rectum were adequately managed by shaving and excision. Deep involvement of the rectum and appendix was identified in 11 of the 35 patients (31.43%) who underwent rectal resection with anastomosis combined with appendectomy. In three of the 35 cases (8.57%), endometriotic disease extended beyond the rectum to involve the vermiform appendix, base of the appendix, and dome of the cecum. A history of one to five prior surgeries for endometriosis was documented in 22 of the 35 patients (62.8%).
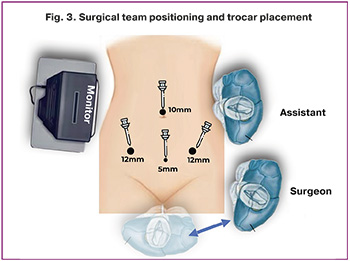
All patients underwent laparoscopic intervention using three-dimensional visualization, a harmonic scalpel, a bipolar vessel-sealing device, and linear and circular stapling instruments. The positioning of the surgical team and trocar placement are shown in Figure 3.
The operative sequence for simultaneous segmental rectosigmoid resection and ileocecal resection with the construction of two anastomoses was as follows:
- Pelvic dissection was performed by the gynecological surgical team.
- Mobilization and resection of the right colonic segments (ileocecal region) were performed by the colorectal surgical team.
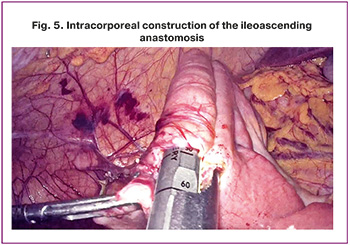
- Intracorporeal construction of the ileocolic [ileoascending] anastomosis.
- Segmental resection of the rectum and/or sigmoid colon was performed.
- Specimen extraction via minilaparotomy or natural orifice specimen extraction (NOSE).
- Intracorporeal construction of sigmoidorectal anastomosis.
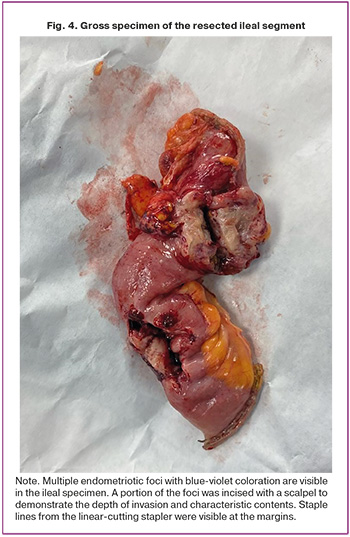
Mobilization of the right colon was performed along the Toldt fascia with division of adhesions at the root of the small-bowel mesentery. The mesentery of the colon and ileum was dissected and divided using the LigaSure bipolar vessel-sealing device close to the bowel wall, preserving the main trunk of the ileocolic and right colic arteries. The resection margin was planned to be 1 cm from the infiltrative boundary, ensuring R0 resection. The ileum and cecum/ascending colon were divided using endoscopic linear cutting staplers (Fig. 4). Following isoperistaltic alignment of the bowel ends, colotomy and enterotomy apertures were created, the jaws of a linear stapler were introduced into the bowel lumen, and anastomosis was performed. The resulting enterotomy was closed with a double-layer suture using V-Loc suture material, with additional reinforcement of the distal angle using interrupted Vicryl 3-0 sutures. In cases of isolated ileal involvement without extension to the cecum or ascending colon, parietal mobilization of the ileal mesentery was performed. The bowel was divided proximally at the margin of the infiltrate and distally at the cecal border, avoiding the creation of a terminal ileal stump. An appendectomy was subsequently performed. An intracorporeal isoperistaltic ileoascending anastomosis was constructed as described above (Figure 5). Ileocecal resection with ileoascending anastomosis was performed in 21 of the 35 patients (60%). In two of the 35 cases (5.7%), intermittent bowel obstruction was identified preoperatively and confirmed intraoperatively by dilatation of the afferent ileal loop to 5–7 cm. In these cases, the mobilized right colonic segment was exteriorized through a periumbilical incision, the bowel was decompressed, and a manual two-layer isoperistaltic ileoascending anastomosis was constructed extracorporeally.
In cases of appendiceal endometriosis extending to the dome of the cecum, marginal resection of the cecal dome was performed to prevent recurrence. Following mobilization of the cecum and delineation of the resection margins within the mesocolon, a linear cutting stapler was applied to the cecal wall. The cecal dome was stapled and excised, and the patency of the ileocecal junction was confirmed intraoperatively.
Resection of rectal endometriotic infiltrates was performed using an embryo-oriented, nerve-sparing technique for segmental rectal resection, as described previously [16]. The configuration of the sigmoidorectal anastomosis varied: end-to-end anastomosis was performed in 23 of 35 patients (65.7%), side-to-side anastomosis in 8 of 35 (22.9%), and end-to-side anastomosis in 2 of 35 (5.7%).
Rectal shaving simultaneous with resection of the right colonic segments was performed in eight of the 35 cases (22.85%). Concomitant urological procedures were performed in two of the 35 patients (5.71%). A prophylactic stoma was fashioned in one of the 35 cases (2.8%) in the setting of combined rectal resection, ileocecal resection, and ureteral resection with reimplantation; stoma closure was performed five weeks postoperatively.
Specimen extraction was accomplished via Pfannenstiel minilaparotomy in 17 of the 35 cases (48.5%), through a periumbilical incision in 11 of the 35 cases (31.4%), through an extended 12 mm trocar site in 4 of the 35 patients (11.4%), and by NOSE transvaginally or transrectally in 3 of the 35 patients (8.5%).
Results
The mean operative time was 283±110 min (range: 150–570 min). The mean intraoperative blood loss was 137.9±118.6 mL (range, 0–400 mL). Return of intestinal peristalsis occurred at a mean of 3.45±0.95 days (range, 2–6 days). Abdominal drainage was employed in 8/35 (22.8%) patients. The mean duration of hospitalization was 6.7±3.6 days (range, 2–17 days).
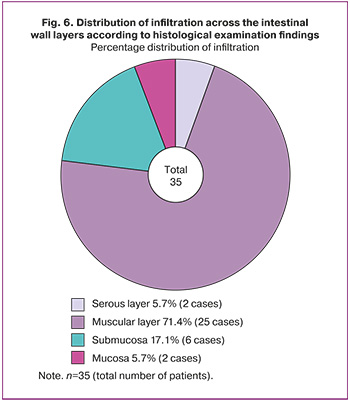
Histological examination confirmed intestinal wall involvement in the form of infiltration of the following layers: serosa in 2/35 (5.7%) patients, muscularis propria in 25/35 (71.4%), submucosa in 6/35 (17.1%), and mucosa in 2/35 (5.7%) (Fig. 6).
Postoperative complications were recorded in 4/35 (11.4%) patients. One case involved suppuration of a periumbilical postoperative wound (2.8%), and another involved intestinal hemorrhage from the sigmoidorectal anastomosis (2.8%), necessitating an emergency colonoscopy with hemostatic clipping. No anastomotic leakage was identified in the right colon in any case in the study group. In one patient who underwent simultaneous resection of the rectum and ileocecal region, clinical signs of sigmoidorectal anastomotic dehiscence involving less than one-quarter of the circumference developed on postoperative day 5. Emergency laparoscopy was performed, comprising suture repair of the anastomotic defect, pelvic drainage, and formation of a diverting transversostomy, which was closed 2.5 months later. In one case, following ureteroplasty, a suture line failure was identified, requiring nephrostomy.
Discussion
Multifocal deep intestinal endometriosis poses a clinically significant challenge. A retrospective analysis by Malzoni M. (2025) demonstrated that, among 426 surgical procedures for excision of endometriotic lesions, intestinal involvement was confirmed in 298 (70%) patients, with lesions localized in two or more intestinal segments in 34% of cases [17]. These findings are consistent with the frequency of right- and left-sided intestinal involvement observed in the present study (31.8%). Segmental resection may be required in more than one-third of cases with transmural intestinal infiltration. Among 670 operated patients, intestinal infiltrate shaving was performed in 422/670 (62.9%) and segmental resection in 248/670 (37%) [12]. In our study, we focused on the outcomes of segmental resections, although shaving was also employed simultaneously in a subset of cases. Assessment of three-year long-term outcomes demonstrated a statistically significant reduction in pain intensity of more than 80% on the visual analogue scale. Quality of life improved in 96% of the operated patients [12]. The disease recurrence rate requiring any form of medical intervention was 4.5%, with no cases necessitating repeated intestinal resection. The overall complication rate, including anastomotic leakage, was 8.06%, consistent with the complication rate observed in our study (11.4%). In a randomized clinical trial by Roman H. et al. (2019), the rate of defunctioning stoma formation in patients undergoing rectal resection for deep endometriosis (DE) was 13% (9/69) [13]. In our study, this figure was lower: stoma formation was required in only 1/35 (2.8%) patients who underwent surgery for multifocal intestinal endometriosis. In the overall segmental resection cohort (n=110), a defunctioning stoma was required in two patients (1.8%), and two cases of sigmoidorectal anastomotic leakage requiring diverting stoma formation were recorded (1.8%). Thus, the overall stoma formation rate was 4/110 (3.6%). Stoma reversal was performed in all patients within 1–3 months after the initial surgery.
In study by Popov A.A. et al. (2024), 104 cases of deep ileocecal endometriosis diagnosed between 2013 and 2023 were included. A total of 73 patients underwent surgery, with combined interventions involving the right and left intestinal segments accounting for 26% (n=27) [18]. This figure is comparable to the rate of simultaneous interventions reported in our study (31.8%). Furthermore, in a prospective study conducted at the Moscow Regional Research Institute of Obstetrics and Gynecology (MONIIAG), the high diagnostic efficacy of targeted transabdominal ultrasound scanning of the right iliac fossa using a linear transducer was demonstrated, enabling preoperative verification of ileocecal endometriosis in 68% of cases (25/37 patients examined). These findings, in the context of the high prevalence of combined ileocaecal and colorectal involvement (65.4%, n=68), substantiate the inclusion of targeted ultrasound assessment of the right iliac fossa in the preoperative evaluation algorithm for patients with endometriosis [18]. Proficiency in nerve-sparing surgical techniques enables minimization of postoperative functional disturbances associated with transection of the hypogastric nerves (nn. hypogastrici), as demonstrated in a comparative study conducted in 2019 that included 118 patients. The nerve-sparing approach was associated with a statistically significant reduction in the incidence of urinary dysfunction in the early postoperative period (11.3% versus 29.8% with the conventional technique) and persistent defecatory disturbances at 6 months postoperatively (4.2% versus 17.0%) [19]. These data confirm that the deliberate identification and preservation of the branches of the inferior hypogastric plexus yields superior functional outcomes in combined intestinal interventions.
Despite the growing interest in this field, the comparative efficacy and safety of surgery for combined right- and left-sided intestinal involvement, which requires different operative approaches and anastomotic techniques, remain insufficiently investigated. A systematic review of the current literature confirms the paucity of evidence regarding the surgical management of simultaneous multi-segment intestinal resection in the context of DE. The data obtained in our study concerning the technical aspects and postoperative outcomes of such procedures are consistent with the limited number of publications addressing this issue. Of particular interest in this context are cases of isolated intestinal endometriosis not associated with pelvic pathology, as they clearly illustrate the diagnostic complexity and the necessity for a thorough intraoperative revision. A pertinent illustration is provided by a case report described in the literature, in which a 35-year-old patient presenting with intestinal obstruction and a mass in the ileocecal region underwent laparoscopic resection of the terminal ileum with anastomosis formation, with histological examination confirming invasive endometriosis with stricture in the setting of intact pelvic organs [20]. Our study included two cases of small bowel obstruction attributable to DE. This case, together with our results, demonstrates that the prevalence of multifocal and atypical forms of intestinal endometriosis may be underestimated: right-sided intestinal involvement in various manifestations and combinations was identified in 35/110 (31.8%) patients in our study. This finding underscores the importance of adequate preoperative diagnostics for operative planning, the necessity of developing standardized diagnostic protocols incorporating advanced imaging and a multidisciplinary approach, and the imperative for a thorough intraoperative inspection of the entire abdominal cavity to identify concomitant lesions. The experience with simultaneous resections using minimally invasive techniques presented in our study represents a logical response to this clinical challenge and contributes to the optimization of surgical care for this patient group. A key consideration is standardizing the approach. When multiple affected zones are identified, double resection can be performed with virtually no modification of the standard trocar placement, thereby minimizing the abdominal wall trauma. The present study aimed to analyze our institutional experience with technically demanding simultaneous operations for combined intestinal endometriosis using contemporary laparoscopic and extraction techniques, which is of considerable relevance to abdominal surgeons and gynecologists and may contribute to the refinement of surgical strategies for this condition.
Conclusion
Laparoscopic resection of the affected intestinal segments in DE is a safe and effective treatment modality, providing a low postoperative complication rate and functional restoration of intestinal patency. These findings support the feasibility of intracorporeal anastomosis formation and minimally invasive techniques within a multidisciplinary framework, particularly in patients with combined involvement of multiple intestinal segments.
References
- Giudice L.C., Kao L.C. Endometriosis. Lancet. 2004; 364(9447): 1789-99. https://dx.doi.org/10.1016/S0140-6736(04)17403-5
- Адамян Л.В., Андреева Е.Н. Эндометриоз и его глобальное влияние на организм женщины. Проблемы репродукции. 2022; 28(1): 54‑64. [Adamyan L.V., Andreeva E.N. Endometriosis and its global impact on a woman’s body. Russian Journal of Human Reproduction. 2022; 28(1): 54‑64 (in Russian)]. https://dx.doi.org/10.17116/repro20222801154
- Адамян Л.В., Арсланян К.Н., Сонова М.М., Харченко Э.И., Логинова О.Н., Ласкевич А.В., Гапарова А.А. Современные тенденции в хирургическом лечении инфильтративных форм эндометриоза. Проблемы репродукции. 2019; 25(5): 36‑41. [Adamyan L.V., Arslanyan K.N., Sonova M.M., Kharchenko E.I., Loginova O.N., Laskevich A.V., Gaparova A.A. Current trends in the surgical treatment of infiltrative forms of endometriosis. Russian Journal of Human Reproduction. 2019; 25(5): 36‑41 (in Russian)]. https://dx.doi.org/10.17116/repro20192505136
- Tomassetti C., Johnson N.P., Petrozza J., Abrao M.S., Einarsson J.I., Horne A.W. et al. An international terminology for endometriosis, 2021. Facts Views Vis. Obgyn. 2021; 13(4): 295-304. https://dx.doi.org/10.52054/fvvo.13.4.036
- Zondervan K.T., Becker C.M., Koga K., Missmer S.A., Taylor R.N., Viganò P. Endometriosis. Nat. Rev. Dis. Primers. 2018; 4(1): 9. https://dx.doi.org/10.1038/s41572-018-0008-5
- Bazot M., Kermarrec E., Bendifallah S., Daraï E. MRI of intestinal endometriosis. Best Pract. Res. Clin. Obstet. Gynaecol. 2021; 71: 51-63. https://dx.doi.org/10.1016/j.bpobgyn.2020.05.013
- Chapron C., Chopin N., Borghese B., Foulot H., Dousset B., Cécile Vacher-Lavenu M. et al. Deeply infiltrating endometriosis: pathogenetic implications of the anatomical distribution. Hum. Reprod. 2006; 21(7): 1839-45. https://dx.doi.org/10.1093/humrep/del079
- Horne A.W., Missmer S.A. Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022; 379: e070750. https://dx.doi.org/10.1136/bmj-2022-070750
- Guerriero S., Condous G., Rolla M., Pedrassani M., Leonardi M., Hudelist G. et al. Addendum to consensus opinion from the International Deep Endometriosis Analysis (IDEA) group: sonographic evaluation of superficial endometriosis. Ultrasound Obstet. Gynecol. 2025; 66(4): 541-7. https://dx.doi.org/10.1002/uog.29288
- Donnez O., Donnez J. Deep endometriosis: the place of laparoscopic shaving. Best Pract. Res. Clin. Obstet. Gynaecol. 2021; 71: 100-13. https://dx.doi.org/10.1016/j.bpobgyn.2020.05.006
- De Cicco C., Corona R., Schonman R., Mailova K., Ussia A., Koninckx P. Bowel resection for deep endometriosis: a systematic review. BJOG. 2011; 118(3): 285-91. https://dx.doi.org/10.1111/j.1471-0528.2010.02744.x
- Malzoni M., Di Giovanni A., Exacoustos C., Lannino G., Capece R., Perone C. et al. Feasibility and safety of laparoscopic-assisted bowel segmental resection for deep infiltrating endometriosis: a retrospective cohort study with description of technique. J. Minim. Invasive Gynecol. 2016; 23(4): 512-25. https://dx.doi.org/10.1016/j.jmig.2015.09.024
- Roman H., Tuech J.J., Huet E., Bridoux V., Khalil H., Hennetier C. et al. Excision versus colorectal resection in deep endometriosis infiltrating the rectum: 5-year follow-up of patients enrolled in a randomized controlled trial. Hum. Reprod. 2019; 34(12): 2362-71. https://dx.doi.org/10.1093/humrep/dez217
- Roman H., Tuech J.J., Huet E., Bridoux V., Khalil H., Hennetier C. et al. Corrigendum. Excision versus colorectal resection in deep endometriosis infiltrating the rectum: 5-year follow-up of patients enrolled in a randomized controlled trial. Hum. Reprod. 2020; 35(3): 736. https://dx.doi.org/10.1093/humrep/deaa019
- Bendifallah S., Puchar A., Vesale E., Moawad G., Daraï E., Roman H. Surgical outcomes after colorectal surgery for endometriosis: a systematic review and meta-analysis. J. Minim. Invasive Gynecol. 2021; 28(3): 453-66. https://dx.doi.org/10.1016/j.jmig.2020.08.015
- Гончаров А.Л., Чичерина М.А., Чернышенко Т.А., Левшин Ф.А., Ненахов Ф.В., Кабешов А.М., Жакиев Н.С., Галлямов Э.А. Особенности колоректальных резекций при глубоком инфильтративном эндометриозе. Хирургия. Журнал им. Н.И. Пирогова. 2022; (12‑2): 54‑8. [Goncharov A.L., Chicherina M.A., Chernyshenko T.A., Levshin F.A., Nenakhov F.V., Kabeshov A.M., Zhakiyev N.S., Gallyamov E.A. The results of colorectal resection for bowel deep infiltrating endometriosis. Pirogov Russian Journal of Surgery. 2022; (12‑2): 54‑8 (in Russian)]. https://dx.doi.org/10.17116/hirurgia202212254
- Malzoni M. Tailoring surgical strategy of bowel endometriosis. Endometriosis Foundation of America (EndoFound). 2025. Available at: https://www.endofound.org/tailoring-surgical-strategy-of-bowel-endometriosis-mario-malzoni-md
- Попов А.А., Пучков К.В., Трошина В.В., Сопова Ю.И., Федоров А.А., Тюрина С.С., Овсянникова М.Р., Ершова И.Ю., Глебов Т.А., Мамедова С.Г. Илеоцекальный эндометриоз: диагностика и лечение. Российский вестник акушера-гинеколога. 2024; 24(4): 77‑82. [Popov A.A., Puchkov K.V., Troshina V.V., Sopova Yu.I., Fedorov A.A., Tyurina S.S., Ovsyannikova M.R., Ershova I.Yu., Glebov T.A., Mamedova S.G. Ileocecal endometriosis: diagnosis and treatment. Russian Bulletin of Obstetrician-Gynecologist. 2024; 24(4): 77‑82 (in Russian)]. https://dx.doi.org/10.17116/rosakush20242404177
- Беженарь В.Ф., Круглов С.Ю., Аракелян Б.В., Кузьмина Н.С., Паластин П.М., Крылова Ю.С. Нерв-сберегающие операции при глубоком инфильтративном эндометриозе. Доктор.Ру. 2019; 7(162): 40-5. [Bezhenar V.F., Kruglov S.Yu., Arakelyan B.V., Kuzmina N.S., Palastin P.M., Krylova Yu.S. Nerve-sparing surgery for deep infiltrating endometriosis. Doctor.Ru. 2019; 7(162): 40-5 (in Russian)] https://dx.doi.org/10.31550/1727-2378-2019-162-7-40-45
- Thirumurthy S.K., Mohammed M. A rare case of invasive endometriosis causing intestinal obstruction. J. Surg. Case Rep. 2024; 2024(2): rjae082. https://dx.doi.org/10.1093/jscr/rjae082
Received 09.12.2025
Accepted 09.04.2026
About the Authors
Artem L. Goncharov, PhD, Colorectal Surgeon, Head of the Coloproctology Department, Central Clinical Hospital with Polyclinic of the Administrative Directorate of the President of the Russian Federation, 15 Marshala Timoshenko str., Moscow, 121359, Russia; Staff member, Endometriosis Surgery Center, Hospital of Fomin Michurinsky Clinic LLC, 15A Michurinsky Ave., Floor 2, Office 5, Moscow, 119192, Russia, goncharovartemleo@gmail.com, https://orcid.org/0000-0002-1326-7893Madina A. Bekova, PhD, Gynecologist, Medical Holding «SM-Clinic», 8-1, Ak. Anokhina str., Moscow, 119602, Russia, bekova.madina@yandex.ru,
https://orcid.org/0000-0002-2362-433X
Filipp A. Levshin, Gynecologist, Head of the Department of Operative Gynecology, Hospital of Fomin Michurinsky Clinic LLC, 15A Michurinsky Ave., Floor 2, Office 5, Moscow, 119192, Russia, fillalex1@yandex.ru, https://orcid.org/0000-0002-1702-0847X
Alexander M. Kabeshov, Obstetrician-Gynecologist, Specialist in Operative Laparoscopy in Gynecology, Hospital of Fomin Michurinsky Clinic, LLC, 15A Michurinsky Ave.,
Floor 2, Office 5, Moscow, 119192, Russia, kabeshovalexander@gmail.com, https://orcid.org/0000-0001-8928-3454
Alexandra A. Kalinina, 5th Year Student, Institute of Clinical Medicine, Pirogov Russian National Research Medical University, Ministry of Health of Russia (Pirogov University), 1-6 Ostrovityanov str., Moscow, 117513, Russia, +7(909)975-25-25, sasha.k.msk@gmail.com, https://orcid.org/0009-0006-0304-051X
Zhannati-Ferdovs R. Tsechoeva, 5th Year Student, Institute of Medicine, Ingush State University, 7 Idrisa Zyazikova Ave., Magas, Republic of Ingushetia, 386001, Russia, jannetta301@mail.ru, https://orcid.org/0009-0008-5388-677X
Corresponding author: Alexandra A. Kalinina, sasha.k.msk@gmail.com
Similar Articles

