
Expression of epithelial–mesenchymal transition markers in different forms of ectopic pregnancy
Danilov A.A., Kozachenko A.V., Badlaeva A.S., Asaturova A.V.
Objective: To investigate the role of epithelial-mesenchymal transition (EMT) in different forms of ectopic pregnancy by analyzing the expression of EMT markers.
Materials and methods: Forty-nine patients who underwent surgical treatment for ectopic pregnancies in various locations were included in the study: cervical/cervico-isthmic (n=20), tubal (n=12), and cesarean scar (n=17). Immunohistochemistry was used to assess EMT marker expression in the intermediate trophoblast, syncytiotrophoblast, and cytotrophoblast of the removed gestational sac, as well as in endometrial/endocervical curettage specimens. Uterine cavity curettage specimens from ten women with normal early pregnancies were used as controls. Statistical analysis was performed using GraphPad Prism 9.3.1 (Dotmatics, USA). The Shapiro–Wilk and Kruskal–Wallis tests were used, with statistical significance set at p<0.05.
Results: Compared with patients with tubal pregnancies, those with rare forms of ectopic pregnancy had a higher number of previous pregnancies, deliveries (including operative deliveries), and abortions. Pre- and post-surgical β-hCG levels were also significantly higher in the rare ectopic pregnancy group. The EMT marker E-cadherin showed comparable expression in the intermediate trophoblast of cervical and normal pregnancies (p>0.5), but higher expression in the cytotrophoblast of patients with cervical pregnancies (p<0.04). The lowest E-cadherin expression was detected in the cytotrophoblasts of tubal pregnancies. In ectopic pregnancies, β-catenin expression predominated in the intermediate trophoblast (p<0.0001), whereas in intrauterine pregnancies, it predominated in the cytotrophoblast.
Conclusion: EMT is involved in the development of ectopic pregnancy, with a specific pattern of EMT marker expression varying depending on the location of the gestational sac.
Authors' contributions: Kozachenko A.V. – final editing of the manuscript; Danilov A.A. – design of the study, material collection, statistical analysis, drafting of the manuscript; Asaturova A.V., Badlaeva A.S. – immunohistochemical study, analysis of the results.
Conflicts of interest: The authors have no conflicts of interest to declare.
Funding: There was no funding for this study.
Ethical Approval: The study was reviewed and approved by the Research Ethics Committee of the V.I. Kulakov NMRC for OG&P, Ministry of Health of Russia.
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Danilov A.A., Kozachenko A.V., Badlaeva A.S., Asaturova A.V. Expression of
epithelial-mesenchymal transition markers in different forms of ectopic pregnancy.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (4): 87-95 (in Russian)
https://dx.doi.org/10.18565/aig.2026.377
Keywords
ectopic pregnancy
cervical pregnancy
cervico-isthmic pregnancy
cesarean scar pregnancy
E-cadherin
β-catenin
Epithelial tissue is characterized by a close association between cells and the basement membrane, which establishes cellular polarity. Epithelial–mesenchymal transition (EMT) is a process in which epithelial cells lose epithelial characteristics, such as apical-basal polarity and expression of cell adhesion markers, and acquire mesenchymal characteristics, including the capacity for migration, invasion, increased resistance to apoptosis, and synthesis of enzymes that degrade the extracellular matrix [1, 2].
Intercellular junctions, particularly transmembrane proteins called cadherins, mediate specific calcium-dependent cell adhesion and facilitate close interactions between epithelial cells. Cadherins are integral components of intercellular junctions and play important roles in the morphogenesis of many tissues and organs. E-cadherin, which is found in epithelial cells, suppresses cellular invasiveness. β-catenins maintain the association of E-cadherin with the cytoskeleton and the integrity of cell layers during embryogenesis, morphogenesis, and tissue homeostasis [1]. At the molecular level, EMT can be mediated by various signaling cascades, with the Wnt pathway being of particular interest.
The current understanding recognizes several types of EMT, which are classified based on their biological context. Type I EMT is crucial for embryonic development and organ morphogenesis. The role of EMT has been confirmed during trophoblast invasion into the decidua in normally progressing pregnancy [3]. As trophoblast invasion occurs, an extravillous zone forms at the apical end of the chorionic villi, specifically in the cytotrophoblast. During EMT, the distal portion of the cytotrophoblast acquires the ability to migrate and invade [4].
In the pathogenesis of tubal ectopic pregnancy, an abnormal microenvironment at the site of trophoblast implantation plays a leading role. Implantation and embryogenesis are closely linked to EMT. This relationship is supported by similarities in protein expression, including β-integrins, the Wnt signaling pathway, mucin-1 (MUC-1), E-cadherin, signal transducer and activator of transcription 3 (STAT3), and matrix metalloproteinases (MMPs) [5].
Given the similarity of the main risk factors for cervical and cesarean scar pregnancies, namely, intrauterine and intracervical surgical manipulations, similar pathogenetic mechanisms may underlie these conditions. Researchers have suggested that EMT-related processes may be a mechanism underlying ectopic pregnancy.
This study aimed to analyze the features of EMT marker expression to clarify its role in the different forms of ectopic pregnancy.
Materials and methods
To investigate the potential role of EMT in ectopic pregnancy progression, 57 pregnant patients with this diagnosis underwent surgical treatment. The diagnosis of ectopic pregnancy was established by pelvic ultrasound examination performed in the Department of Functional Diagnostics of the V.I. Kulakov National Medical Research Centre for Obstetrics, Gynecology, and Perinatology of the Ministry of Health of the Russian Federation using a Voluson S10 ultrasound system. Based on the implantation site of the gestational sac, patients were allocated to three groups: 20 patients with cervical or cervico-isthmic pregnancy, 20 patients with tubal pregnancy, and 17 patients with ectopic pregnancy implanted within a uterine scar following a prior caesarean section.
All patients underwent serial measurement of serum beta-human chorionic gonadotropin (β-hCG) concentrations using electrochemiluminescence immunoassay performed on a Cobas e411 automated immunochemical analyzer (Roche Diagnostics GmbH, Germany) using the manufacturer's proprietary commercial reagent kits. Venous blood samples were collected from the antecubital vein using closed-system S-Monovette collection tubes with a clot activator (Sarstedt, Germany). Serum was obtained by centrifugation at 3,000 rpm for a minimum of 10 minutes using an Eppendorf 5804 centrifuge (Germany).
Surgical treatment was performed in the Gynecology Department of the V.I. Kulakov NMRC for OG&P of the Ministry of Health of the Russian Federation. Intraoperatively, tissue specimens comprising excised gestational sac and endometrial/endocervical curettage material were collected for subsequent immunohistochemical analysis. As a reference control, curettage specimens from the uterine cavity were obtained from ten women with normally progressing early pregnancies.
Tissue samples were fixed in buffered 10% formalin and subsequently processed according to a standard histological protocol comprising graded alcohol dehydration and xylene clearing, followed by paraffin embedding. Four-micrometer sections were cut from the paraffin blocks, mounted on glass slides, and stained with hematoxylin and eosin. For immunohistochemical analysis, positively charged slides were dried in a thermostatic oven for 24 h at 48°C.
At the initial stage of the study, the antibody titers were optimized (Table 1).

Immunohistochemical staining was performed on a BenchMark XT automated stainer (Ventana, Roche, Switzerland) using standard protocols (incubation temperature 37°C, incubation time 16–24 min), the DAB Universal ultraView detection kit (Ventana, Roche, Switzerland), and manual counterstaining, followed by dehydration through a graded alcohol and xylene series and coverslipping. This protocol was uniformly applied to each of the aforementioned antibodies.
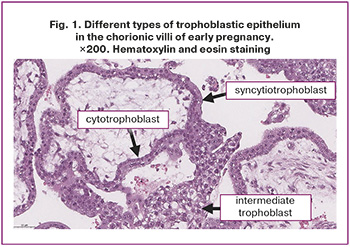
Digital whole-slide images in the SVS format were acquired for each immunohistochemically stained section using an Aperio AT2 scanning microscope (Leica Biosystems, Germany). Morphometric analysis was conducted within a fixed area of 2 mm² in chorionic villi, with quantification of staining intensity for tissue markers in the intermediate trophoblast, syncytiotrophoblast, and cytotrophoblast, and calculation of mean values (Fig. 1). Staining intensity was expressed in arbitrary units on a green-channel grayscale using QuPath software.
Statistical analysis
All study data were subjected to statistical analysis using parametric and non-parametric methods. For categorical clinical variables (presenting complaints, reproductive history, and treatment modalities), frequencies and proportions (expressed as percentages) were calculated. Between-group comparisons of categorical variables were performed using the chi-square and Fisher’s exact tests. Given the small sample sizes in each group, continuous variables are reported as median with interquartile range [presented in tables as Me (Q25%; Q75%)]; non-parametric tests were applied for between-group comparisons, specifically the Kruskal–Wallis test for multi-group comparisons and the Mann–Whitney U test for pairwise comparisons. A significance level of p=0.05 was adopted for all inferential analyses. The Bonferroni correction was applied for multiple pairwise comparisons (p=0.017 for three-group comparisons; p=0.008 for four-group comparisons). The computation of clinical parameters, data collation, verification, organization, and visualization of immunohistochemical results were performed using Microsoft Excel 2019 and IBM SPSS Statistics, version 26.
Results
A comparative analysis of clinical complaints and characteristics was conducted across the different ectopic pregnancy groups.
As shown in Table 2, the median age of patients with rare-site ectopic pregnancy did not differ significantly between the groups.
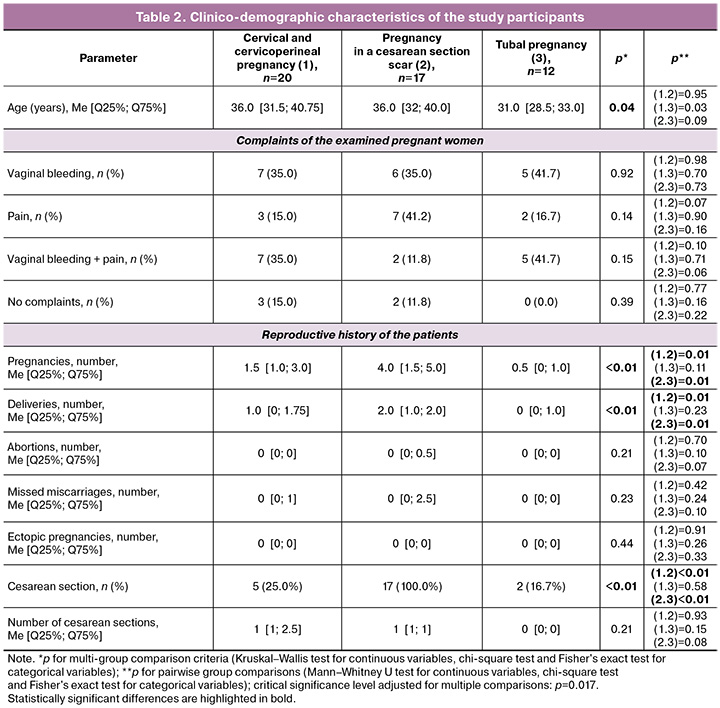
The predominant presenting complaints among patients with ectopic pregnancy were vaginal bleeding and pain. Vaginal bleeding was reported more frequently in patients with tubal pregnancy – 5/12 (41.7%), whereas lower abdominal pain was the predominant complaint in the cesarean scar pregnancy group – 7/17 (41.2%). Combined pain and vaginal bleeding were reported most frequently in tubal pregnancy – 5/12 (41.7%) and cervico-isthmic pregnancy – 7/20 (35.0%). No statistically significant differences in the frequency of these complaints were observed between the groups (p>0.07).
The profiles of concomitant gynecological pathologies did not differ significantly between the groups. However, the rates of assisted reproductive technology (ART) procedures and hysteroscopy were significantly higher in the cervical/cervico-isthmic pregnancy group than in the cesarean scar pregnancy group (p=0.02). No significant differences in the frequency of ART procedures or hysteroscopy were identified when comparing the cervical/cervico-isthmic and tubal pregnancy groups (p=0.19 and p=0.72, respectively).
The number of prior pregnancies, deliveries, and cesarean sections was significantly greater in the cesarean scar pregnancy group than in the cervical/cervico-isthmic and tubal pregnancy groups. The rates of induced abortions, missed miscarriages, and prior ectopic pregnancies did not differ significantly among the groups.
Comparative analysis of serum β-human chorionic gonadotropin (β-hCG) levels (Table 3) demonstrated significantly higher values in the rare-site ectopic pregnancy groups than in the tubal pregnancy group, both before and after surgical treatment. The highest β-hCG levels were recorded in the cesarean scar pregnancy group.
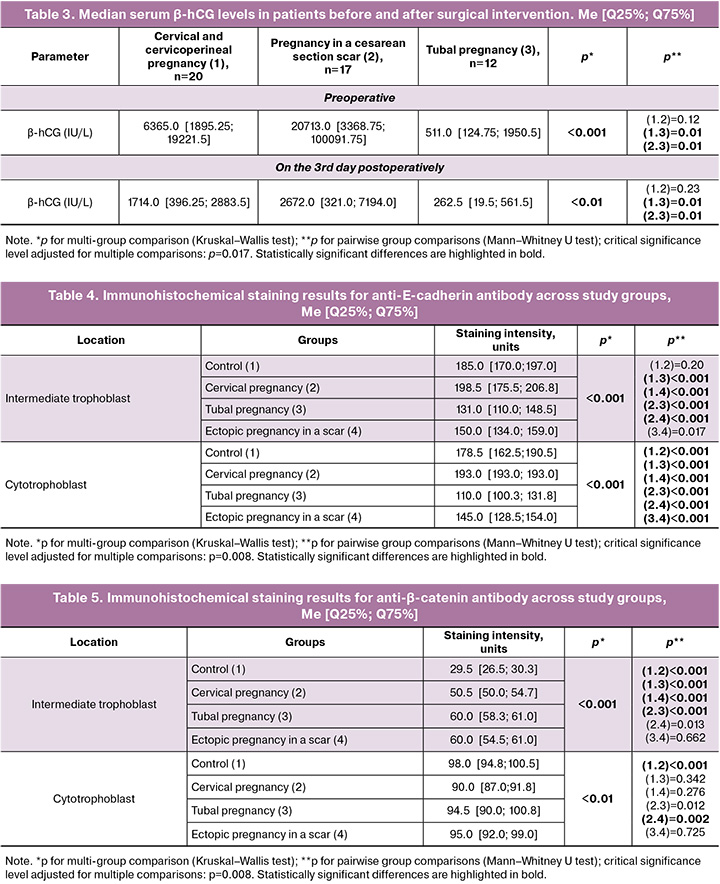
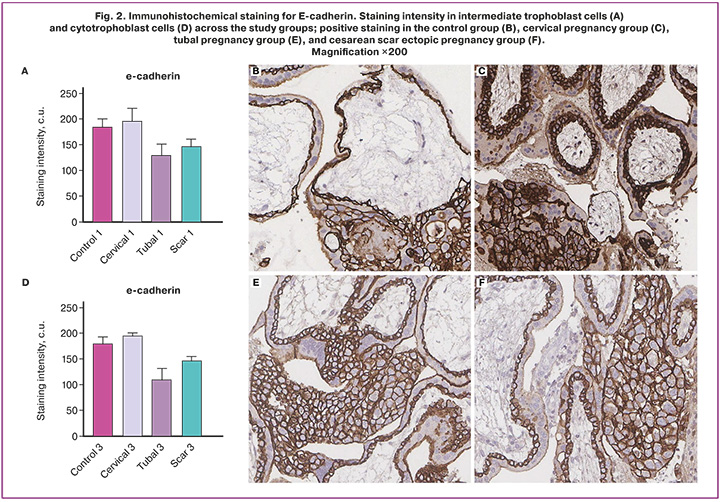
Assessment of E-cadherin expression (Fig. 2) revealed maximal staining intensity in the intermediate trophoblast (Fig. 2A), and cytotrophoblasts (Fig. 2D) specimens from patients with cervical pregnancies. E-cadherin expression in the intermediate trophoblast did not differ substantially between cervical and normal pregnancies; the median values were 198.5 and 185 conventional units (c.u.), respectively (p=0.20). However, assessment of E-cadherin staining intensity in the cytotrophoblast revealed a significant difference between cervical and normal pregnancy; the median values were 193 and 178.5 c.u., respectively (p<0.001). E-cadherin expression in both tubal and cesarean scar ectopic pregnancy was significantly lower in both intermediate trophoblasts and cytotrophoblasts compared to the control group (p<0.001). The lowest E-cadherin values were observed in the cytotrophoblasts in tubal pregnancy. No E-cadherin expression was detected in the syncytiotrophoblasts in any of the examined specimens.
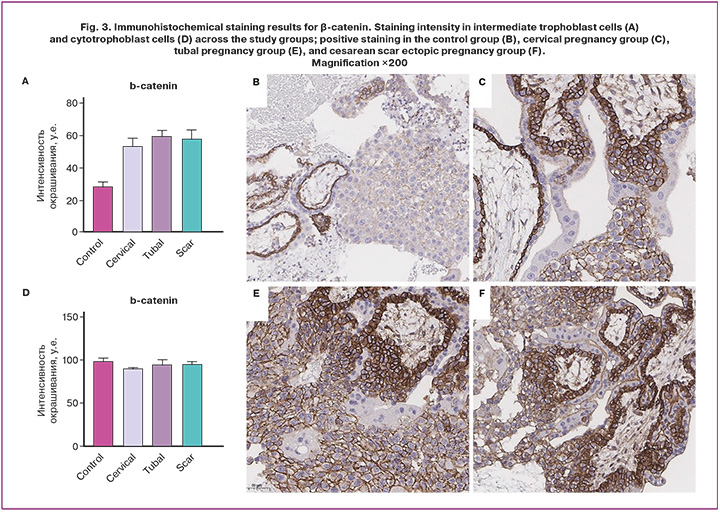
Assessment of β-catenin expression revealed its significant predominance in the intermediate trophoblast (Fig. 3A) across all forms of ectopic pregnancy compared with normal pregnancy (p<0.001). Conversely, β-catenin expression in cytotrophoblasts (Fig. 3D) was higher in patients with normal pregnancies than in those with ectopic pregnancies. A significant difference in β-catenin staining intensity was observed between normal and cervical pregnancies (p≤0.001). The differences in β-catenin expression between tubal and cesarean scar ectopic pregnancies relative to the control group were not statistically significant (p≥0.05).
Taken together, EMT marker expression was detected in both intermediate trophoblasts and cytotrophoblasts across all study groups. No expression of these markers was identified in the syncytiotrophoblasts in any of the examined specimens.
Discussion
The dynamic balance between cellular adhesion and migration is essential for the successful progression of pregnancy. Cadherin-catenin complexes, which participate in intercellular junctions and regulate signaling pathways that control cell division and differentiation, play an important role in these processes.
In our study, immunohistochemical analysis of E-cadherin revealed the highest staining intensity in intermediate trophoblast and cytotrophoblast samples from patients with cervical pregnancy. E-cadherin expression in cervical pregnancy was higher in both intermediate trophoblasts and cytotrophoblasts than in normal pregnancy. In contrast, tubal and cesarean scar ectopic pregnancies were characterized by markedly lower E-cadherin expression, with the lowest levels identified in the cytotrophoblasts in tubal pregnancies.
E-cadherin, also known as epithelial cadherin (cadherin-1 (type 1; CD324)), is a membrane glycoprotein belonging to the family of calcium-dependent proteins involved in cell adhesion, motility, and proliferation of epithelial cells, and it potentially suppresses cellular invasiveness. The increased E-cadherin level in cervical pregnancy may be related to the unique characteristics of the chorionic invasion site. The cervix is inherently unsuitable for normal implantation and placentation due to weak decidualization, a limited amount of muscle tissue, and moderate capacity for blood supply. In cervical pregnancy, invasion occurs more deeply than in normal pregnancy, with chorionic villi penetrating deeply between the fibromuscular elements of the cervix. Furthermore, in the present study, patients with cervical/cervico-isthmic pregnancies more often had a history of ART procedures and hysteroscopies, which are likely risk factors for impaired decidualization, scarring, and alterations in muscular architecture [6]. Therefore, the elevated E-cadherin level in cervical pregnancy may be due to the degradation of a substantial area of dense intercellular junctions within the connective tissue.
In pregnancies developing within a cesarean scar, implantation of the gestational sac occurs in the area of the scar tissue defect due to insufficient decidualization, possibly resulting from the high rate of cesarean delivery among patients in the study. A study by Gao L. et al. (2022), using immunohistochemical evaluation of samples obtained during laparoscopic excision of cesarean scar pregnancy at 6–11 weeks of gestation, demonstrated significantly reduced E-cadherin expression in the scarred myometrium in response to trophoblast invasion [7]. However, outside the implantation zone, E-cadherin expression in the scar tissue was significantly higher. Consistent with this, our study also observed lower E-cadherin expression in scar pregnancy than in intrauterine pregnancy. In addition, patients in this group demonstrated significantly higher β-hCG levels. The literature suggests that elevated β-hCG levels are associated with cellular invasiveness and the expression of EMT markers in several cancers, particularly ovarian cancer [8, 9]. Researchers have proposed that the stimulatory effect of β-hCG on EMT is related to its structural similarity to transforming growth factor-β (TGF-β), a well-known promoter of EMT [10–12]. Based on this, it is reasonable to assume that trophoblast invasion into the area of a uterine scar defect is greatly facilitated by the absence of decidualization in the defect area, as well as by fibrosis and scattered myometrial fibers. Our data also support the theory that uterine scar pregnancy occurs only in the presence of an actual scar defect.
The pattern of trophoblast invasion during the development and progression of tubal ectopic pregnancy may also be explained from the perspective of the EMT. Several authors have reported that the implantation site of the gestational sac in the fallopian tube is characterized by the lowest E-cadherin level [13, 14]. In our study, tubal pregnancy exhibited the minimal degree of E-cadherin expression compared with the control group and other types of ectopic pregnancies. Researchers have reported significantly reduced E-cadherin expression in chronic inflammatory disease of the fallopian tubes and an altered ratio of ciliated to secretory epithelium, which they attribute to increased activity of the Wnt signaling pathway [13, 14]. Areas with disrupted EMT processes in the fallopian tube become sites of pathological implantation.
According to the immunohistochemical assessment of β-catenin expression, intrauterine pregnancy was characterized by a relatively low level in intermediate trophoblast cells and a fairly high level in the cytotrophoblast. In ectopic pregnancy, the β-catenin level in intermediate trophoblasts was twofold higher than that observed in intrauterine pregnancy. However, the pattern of β-catenin changes in intermediate trophoblasts did not differ substantially among the various forms of ectopic pregnancy. The degree of β-catenin expression in cytotrophoblasts in all forms of ectopic pregnancy was somewhat lower than that in intrauterine pregnancy.
We believe that the increased β-catenin expression in intermediate trophoblasts in ectopic pregnancy reflects the limited invasive potential associated with pathological implantation.
β-Catenin is a protein and a marker of the epithelial phenotype that participates in cell adhesion together with E-cadherin; it also acts as the principal effector of the Wnt signaling pathway, which plays an important role in embryonic development and tissue homeostasis [11, 15]. Free β-catenin in the cytosol is rapidly degraded unless the Wnt signaling pathway is activated. In recent years, it has been established that E-cadherin and its associated catenins, especially β-catenin, are not merely static components of adhesive junctions but also contribute to the maintenance of cellular differentiation in two ways: by establishing cell-cell adhesive interactions and basolateral polarity and by acting as a negative regulator of the Wnt signaling pathway. Thus, β-catenin degradation is required to enable Wnt signaling, which initiates the complex morphogenetic process of EMT. As previously shown, the transformation of cytotrophoblasts into extravillous trophoblasts is mediated by EMT [16]. Previous studies have demonstrated reversible changes in adhesion molecules. During the transformation of epithelial cells into mesenchymal cells, β-catenin expression decreases significantly, cell-cell contacts are weakened, and the capacity for migration and invasion increases [17]. Experimental studies have shown that β-catenin overexpression leads to reduced decidualization and impaired implantation [18]. Therefore, the pattern of β-catenin expression may reflect the altered EMT mechanisms underlying pathological implantation in ectopic pregnancy.
Conclusion
In summary, this study demonstrated that the development of ectopic pregnancy is associated with the expression of various EMT markers, the pattern of which depends on the type of ectopic pregnancy. From the perspective of EMT involvement, several pathophysiological processes arising in ectopic pregnancy may be explained, particularly the formation of a pool of highly invasive cells. Thus, based on the study findings, it may be assumed that EMT may play a role as one of the factors influencing the onset and development of ectopic pregnancy.
References
- Гапонова А.В., Родин С., Мазина А.А., Волчков П.Ю. Эпителиально-мезенхимальный переход: злокачественная прогрессия и перспективы противоопухолевой терапии. Acta Naturae. 2020; 12(3): 4-23. [Gaponova A.V., Rodin S., Mazina A.A., Volchkov P.Yu. Epithelial-mesenchymal transition: malignant progression and prospects of anticancer therapy. Acta Naturae. 2020; 12(3): 4-23 (in Russian)].
- Шварев Е.Г., Зоева А.Р., Зайцев И.В. Эпителиально-мезенхимальный переход как важный этап формирования патологических пролиферативных заболеваний матки. Российский вестник акушера-гинеколога. 2025; 25(4): 37 43. [Shvarev E.G., Zoeva A.R., Zaitsev I.V. Epithelial-mesenchymal transition as an important stage in the formation of pathological proliferative diseases of the uterus. Russian Bulletin of Obstetrician-Gynecologist. 2025; 25(4): 37 43 (in Russian)]. https://dx.doi.org/10.17116/rosakush20252504137
- Akhurst R.J. From shape-shifting embryonic cells to oncology: The fascinating history of epithelial mesenchymal transition. Semin. Cancer Biol. 2023; 96: 100-14. https://dx.doi.org/10.1016/j.semcancer.2023.10.003
- Вишнякова П.А., Тарасова Н.В., Володина М.А., Марей М.В., Ходжаева З.С., Кан Н.Е., Высоких М.Ю. Эпителиально-мезенхимальный переход в плаценте при преэклампсии. Акушерство и гинекология. 2016; 12: 53-7. [Vishnyakova P.A., Tarasova N.V., Volodina M.A., Marei M.V., Khodzhaeva Z.S., Kan N.E., Vysokikh M.Yu. Placental epithelial-mesenchymal transition in preeclampsia. Obstetrics and Gynecology. 2016; (12): 53-7 (in Russian)]. https://dx.doi.org/10.18565/aig.2016.12.53-7
- Bilyk O., Coatham M., Jewer M., Postovit L.M. Epithelial-to-mesenchymal transition in the female reproductive tract: from normal functioning to disease pathology. Front. Oncol. 2017; 7: 145. https://dx.doi.org/10.3389/fonc.2017.00145
- Panelli D.M., Phillips Flanagan C.H., Brady P.C. Incidence, diagnosis and management of tubal and nontubal ectopic pregnancies. Fertil. Res. Pract. 2015; 1: 15. http://dx.doi.org/10.1186/s40738-015-0008-z
- Gao L., Chen H., Liu J., Wang M., Lin F., Yang G. et al. Extravillous trophoblast invasion and decidualization in cesarean scar pregnancies. Acta Obstet. Gynecol. Scand. 2022; 101(10): 1120-8. https://dx.doi.org/10.1111/aogs.14435
- Liu N., Peng S.M., Zhan G.X., Yu J., Wu W.M., Gao H. et al. Human chorionic gonadotropin β regulates epithelial-mesenchymal transition and metastasis in human ovarian cancer. Oncol. Rep. 2017; 38(3): 1464-72. https://dx.doi.org/10.3892/or.2017.5818
- Kawamata F., Nishihara H., Homma S., Kato Y., Tsuda M., Konishi Y. et al. Chorionic gonadotropin β modulates epithelial-mesenchymal transition in colorectal carcinoma metastasis. Am. J. Pathol. 2018; 118(1): 204-15. https://dx.doi.org/10.1016/j.ajpath.2017.08.034
- Ishida M., Takebayashi A., Kimura F., Nakamura A., Kitazawa J., Morimune A. et al. Induction of the epithelial-mesenchymal transition in the endometrium by chronic endometritis in infertile patients. PLoS One. 2021; 16(4): e0249775. https://dx.doi.org/10.1371/journal.pone.0249775
- Kahata K., Dabras M.S., Moustakas A. TGF-beta family signaling in epithelial differentiation and epithelial-mesenchymal transition. Cold Spring Harb. Perspect. Biol. 2018; 10(1): a022194. https://dx.doi.org/10.1101/cshperspect.a022194
- Song P., Gao Z., Bao Y., Chen L., Hang Y., Liu Y. et al. Wnt/beta-catenin signaling pathway in cancerogenesis and cancer therapy. J. Hematol. Oncol. 2024; 17(1): 46. https://dx.doi.org/10.1186/s13045-024-01563-4
- Jiang H., Yang X.Y., Zhu W.J. Network of E-cadherin, β1 integrin, and local adhesion kinase in the pathogenesis of tubal pregnancy. Gynecol. Endocrinol. 2019; 35(4): 346-50. https://dx.doi.org/10.1080/09513590.2018.1528578
- Flanagan H., Lin C.J., Campbell L.L., Horner P., Horne A.W., Spears N. Ectopic pregnancy and epithelial to mesenchymal transition: is there a link? Reproduction. 2020; 161(3): V11-4. https://dx.doi.org/10.1530/REP-20-0542
- Han Q., Zheng L., Liu Z., Luo J., Chen J., Yan J. Expression of β-catenin in human trophoblast and its role in placenta accreta and placenta previa. J. Int. Med. Res. 2016; 47(1): 206-14. https://dx.doi.org/10.1177/0300060518799265
- Liu Y., Li P., Liao J., Rao M., Peng L., Gan H. et al. Decreased RSPO3 and beta-catenin in preeclampsia: correlation with blood pressure and pregnancy outcomes. Med. Sci. Monit. 2024; 30: e945848. https://dx.doi.org/10.12659/MSM.945848
- DaSilva-Arnold S., James J.L., Al-Khan A., Zamudio S., Illsley N.P. Differentiation of first-trimester cytotrophoblast to extravillous trophoblast involves epithelial-mesenchymal transition. Placenta. 2015; 36(12): 1412-8. https://dx.doi.org/10.1016/j.placenta.2015.10.013
- Chronopoulou E., Koika V., Tsiveriotis K., Stefanidis K., Kalogeropoulos S., Georgopoulos N. et al. Wnt4, Wnt6 and beta-catenin expression in human placental tissue – is there a link with first trimester miscarriage? Results from a pilot study. Reprod. Biol. Endocrinol. 2022; 20(1): 51. https://dx.doi.org/10.1186/s12958-022-00923-4
Received 16.12.2025
Accepted 19.03.2026
About the Authors
Andrey A. Danilov, PhD student at the Gynecological Department, V.I. Kulakov NMRC for OG&P, Ministry of Health of Russia, 117997, Russia, Moscow, Ac. Oparin str., 4,andreydanilov2018@gmail.com, https://orcid.org/0009-0009-1959-2548
Andrey V. Kozachenko, Dr. Med. Sci., Senior Researcher at the Gynecological Department, V.I. Kulakov NMRC for OG&P, Ministry of Health of Russia, 117997, Russia, Moscow, Ac. Oparin str., 4, a_kozachenko@oparina4.ru, https://orcid.org/0000-0002-5573-6694
Alina S. Badlaeva, PhD, Senior Researcher at the 1st Pathoanatomical Department, V.I. Kulakov NMRC for OG&P, Ministry of Health of Russia, 117997, Russia, Moscow,
Ac. Oparin str., 4, a_badlaeva@oparina4.ru, https://orcid.org/0000-0001-5223-9767
Alexandra V. Asaturova, Dr. Med. Sci., Head of the 1st Department of Anatomical Pathology, V.I. Kulakov NMRC for OG&P, Ministry of Health of Russia, 117997, Russia, Moscow, Ac. Oparin str., 4, a_asaturova@oparina4.ru, https://orcid.org/0000-0001-8739-5209
Similar Articles

