
Retrospective analysis of urgent gynecological laparoscopic surgery in patients of reproductive age
Sulima A.N., Gudz O.V.
Objective: To perform a retrospective analysis to identify relationship between various nosological forms and blood volume loss, the severity of the adhesive process, duration of surgery and postoperative rehabilitation period in emergency gynecology.
Materials and methods: The analysis of 371 cases of emergency surgery in women of reproductive age was performed. The women were divided into 4 groups. Group 1 comprised 158/371 (42.6%) women with ovarian apoplexy or ruptured ovarian cysts. Group 2 included 92/371 (24.8%) women with interrupted ectopic pregnancy. Group 3 included 65/371 (17.5%) women with various complicated forms of extragenital endometriosis. Group 4 consisted of 56/371 (15.1%) women with combination of factors.
Results: The maximum volume of blood loss was 290.0 ml in group 1 versus 132.0 ml in group 3, 100 ml in group 2 and 118.5 ml in group 4. The maximum duration of surgery was 63.0 and 64.0 minutes in group 1 and 2. The maxim length of hospital stay was 6 bed days in group 3 and the minimum length was 3.5 bed days in group 2. Minimal severity level of adhesions (stage 1) was most often in group 1 (in 87.3% of women), and maximal severity level (stage IV) was in group 3 (in 7.7% of women).
Conclusion: In the structure of urgent gynecological disorders, ovarian apoplexy or ruptured ovarian cysts were predominant. Ectopic pregnancy ranked second. Blood volume loss was higher in women with ovarian apoplexy and ruptured ovarian cysts. Duration of surgery and rehabilitation period was longer in women with extragenital endometriosis.
Author contribution. Sulima A.N. – the concept and design of the study, article editing; Gudz O.V. – data analysis,
literature review, article writing.
Conflicts of interest: The authors declare that they have no conflicts of interest.
Funding: The study was conducted without any sponsorship.
Ethical Approval: The protocol of the study was approved by the Local Ethics Committee of the Medical Institute named
after S.I. Georgievsky, V.I. Vernadsky Federal Crimean University.
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Sulima A.N., Gudz O.V. Retrospective analysis of urgent gynecological laparoscopic surgery in patients of reproductive age.
Akusherstovo i Gynecologia/Obstetrics and Gynecology. 2024; (1): 118-122 (in Russian)
https://dx.doi.org/10.18565/aig.2023.247
Keywords
ovarian apoplexy
endometriosis
ectopic pregnancy
blood loss
duration of surgery
Gynecological emergencies requiring urgent surgery, are life-threatening conditions, and the term “acute abdomen” includes several major nosological forms [1–5].
The result of urgent surgery is elimination of the etiological factor that led to surgical intervention and preservation of reproductive potential [2–5]. There are three major nosological forms in emergency gynecology, that require hospitalization: ruptured ovarian cyst, apoplexy, external genital endometriosis, ectopic pregnancy and a combination of several causes [1–7]. Some studies analyzed the structure of surgical interventions in emergency gynecology. The study by Malyshkina A.I. et al. compared the age of patients, the etiological factors, the surgical access, the volume of interventions; however, but blood loss volume, duration of surgical intervention, the severity of adhesions and the length of postoperative hospital stay were not assessed [5]. The study by Miklyaeva I.A. et al. analyzed the etiological factors, the surgical access and volume, but other data were not analyzed [6]. Analysis of the etiological factors, assessment of the proportion of each factor as the cause for surgery, the age of patients, duration of surgical interventions, blood loss volume, the prevalence of adhesions requires further exploration and comparison of various nosologies in emergency gynecology [5–10]. Attention should be paid to timely diagnosis of external genital endometriosis, which is considered to be a risk factor of surgical and postoperative complications [11]. Taking into account the era of delayed motherhood, urgent surgical interventions require research to improve surgical techniques aimed to reduce negative factors resulting from surgical intervention and improve postoperative rehabilitation techniques.
Aim of the study was to perform a retrospective analysis to identify relationship between various nosological forms and blood volume loss, the severity of the adhesive process, duration of surgery and postoperative rehabilitation period in emergency gynecology.
Materials and methods
A retrospective analysis of 371 medical histories of patients of reproductive age, who were urgently hospitalized in Gynecological Emergency Department of Simferopol clinical maternity hospital No. 2 (in Simferopol) and underwent surgery in the period from 2019 to 2022, was conducted.
Surgical interventions were performed using standard videoendoscopic techniques.
Exclusion criteria were the age of patients below 19 years and over 49 years; elective surgical treatment; malignant neoplasms in female reproductive system.
To investigate and analyze the cases of surgical treatment, the women were divided into 4 groups. Group 1 comprised 158/371 (42.6%) women with records of surgical intervention due to ovarian apoplexy or ruptured ovarian cysts in medical history. Group 2 included 92/371 (24.8%) women with interrupted ectopic pregnancy. Group 3 included 65/371 (17.5%) women with various complicated forms of external genital endometriosis. Group 4 consisted of 56/371 (15.1%) women, who previously underwent surgery because of non-gynecological indications, or due to combination of factors, which potentially led to adhesions (including appendectomy, salpingo-oophoritis, pathological processes of neighboring pelvic and abdominal organs, as well as various traumas).
The following data were investigated:
1) the age of patients (years);
2) duration of surgery;
3) intraoperative blood loss (ml);
4) intraoperative determination of the severity grading of adhesions (grade 1–4);
5) the length of postoperative hospital stay (bed-days).
Assessment of the prevalence of the adhesive process was done according to the American Fertility Society classification (1988), that takes into account the prevalence, localization and nature of the adhesive process, as well as obliteration of the fallopian tubes [12].
Statistical analysis
For quantitative parameters, the Shapiro–Wilk test was used to compare how close the empirical distribution fit to the normal distribution [13].
Since at least in one sample there were statistically significant differences between the empirical and normal distribution with critical values at p<0.05 for each parameter, further statistical analysis was performed using nonparametric rank-based methods. The median (Me) and interquartile range (Q1; Q3) were calculated as the indicators of descriptive statistics of the analyzed quantitative data.
The nonparametric rank-based Kruskal–Wallis test was used to verify the hypothesis of the equality of medians in the analyzed four samples [14]. The Dunn’s post-hoc test was used for pairwise comparison for the equality of medians of parameters in the analyzed samples [15]. Holm–Bonferroni p-value adjustments were made to account for multiple pairwise comparisons [16]. For interpretation of the results of statistical analysis, the critical value of the level of statistical significance was at p<0.05.
The degree of adhesion can be expressed by ordinal or categorical scales of measurement. Consequently, the analysis of this indicator a priori cannot be performed using parametric statistical methods. In our study, based on clinical assumptions, this indicator was considered to be categorical (where the stages of the adhesive process from 1 to 4 were denoted as categories). Therefore, the absolute and relative frequency was used in descriptive statistics, and the chi-square goodness-of-fit test was used to compare distribution in four analyzed groups [17].
Statistical data processing was performed using software program PAST, version 4.03, that was used for free for scientific purposes conditional upon reference for the first publication of the authors’ program [18].
Results and discussion
Table 1 presents descriptive statistics and the results of comparison of quantitative parameters with indication of precise values of the statistical significance level p according to the Kruskal–Wallis test.
The results of pairwise comparisons of quantitative parameters that were obtained using the Dunn’s post-hoc test and Holm–Bonferroni correction are shown in Table 2.
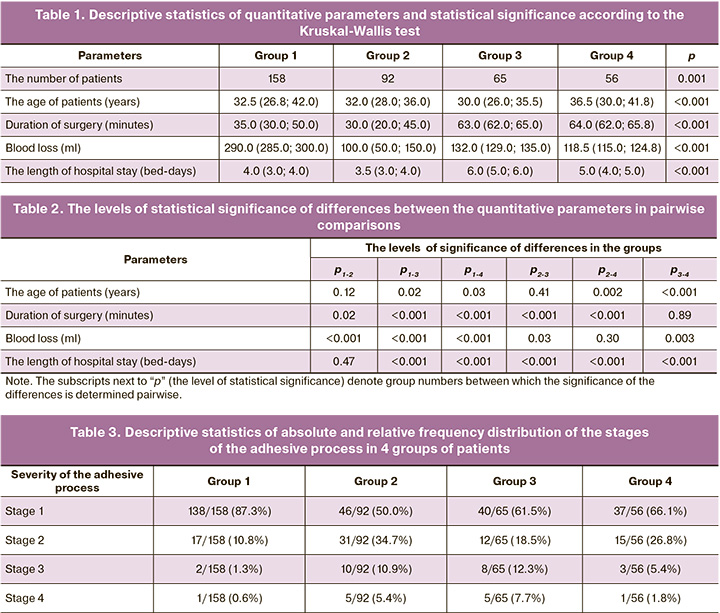
In addition, the initial numerical values of the parameters are shown in Table 1.
Table 3 shows the descriptive statistics for the stage of adhesion in absolute and relative frequency (in percentage).
Chi-square test showed that there are differences between frequency distribution of the stages of the adhesive process in 4 groups at the level of significance p<0.001 (χ2=51.8, the number of the degrees of freedom k=9).
The analysis demonstrated that ruptured ovarian cyst or ovarian apoplexy is a nosological form that most often was the reason for urgent hospitalization (158 patients in group 1; 92 patients in group 2; 65 patients in group 3, and 56 patients in group 4) and was accompanied by higher blood loss – 290.0 (285.0;300.0) ml in group 1 versus minimal blood loss – 100.00 (50.0;150.0) ml in group 2. The obtained results differ from the results of retrospective analysis done by other authors. According to analysis of urgent interventions performed by Malyshkina et a. in 2018–202 in V.N. Gorodkov Research Institute of Maternity and Childhood, the Ministry of Health of Russia, the most common reason for hospitalization was ectopic pregnancy –in 67.4% of cases, while ovarian apoplexy – only in 25.2% of cases [5]. However, Miklyaeva I.A. et al., who did the analysis of urgent care in V.N. Gorodkov Research Institute of Maternity and Childhood, the Ministry of Health of Russia, reported that the most common reason for hospitalization was ectopic pregnancy – in 44% of cases, and ovarian apoplexy ranked second – in 42% of cases, that was only 2% less [6].
Given the data in Table 1, maximum time of surgery duration was in group 3 and 4, where the results were almost identical: 64.0 (62.0; 65.8) minutes in group 4 and 63.0 (62.0; 65.0) minutes in group 3 versus 35.0 (30.0; 50.0) minutes in group 1, 30.0 (20.0;45.0) minutes in group 2. Longer lasting surgery in group 3 and 4 was due to external genital endometriosis, and combination of various etiological factors that led to surgical intervention in women in group 4. The maximum length of postoperative rehabilitation period was 6.0 (5.0; 6.0) and 5.0 (4.0; 5.0) bed-days in group 3 and 4, respectively. Therefore, the diagnosis of external genital endometriosis or the presence of combination of factors that led to urgent intervention, even at the stage of hospitalization suggested necessity to get ready for a longer surgical intervention and a longer postoperative rehabilitation period.
The analysis of the severity grade of the adhesive process in 4 groups showed, that grade 4 was most often in group 3 that included the patients with external genital endometriosis – in 5/65 (7.7%) women. Minimal prevalence of the adhesive process was most often in group 1 – in 138/158 (87.3%) women.
Conclusion
- In the structure of urgent gynecological pathology, ovarian apoplexy or ruptured ovarian cysts were predominant – 158/371 (42.6%) cases. The second most common nosological form was ectopic pregnancy – 92/371 (24,8%) cases.
- With ruptured ovarian cysts and ovarian apoplexy, clinical and statistical blood volume loos was significantly higher.
- With anamnestic and clinical diagnosis of external genital endometriosis, postoperative rehabilitation period is longer.
- Common forms of external genital endometriosis lead to severe grade of adhesion – stage 4 according to the American Fertility Society classification (1988).
- Duration of surgical intervention was longer in the group of patients with external genital endometriosis and combination of several etiological factors.
References
- Самарцев В.А., Гаврилов В.А., Пушкарев Б.С., Паршаков А.А., Кузнецова М.П., Кузнецова М.В. Спаечная болезнь брюшной полости: состояние проблемы и современные методы профилактики. Пермский медицинский журнал. 2019;36(3):72-90. [Samartsev V.A., Gavrilov V.A., Pushkarev B.S., Parshakov A.A., Kuznetsova M.P., Kuznetsova M.V. Adhesive disease of the abdominal cavity: the state of the problem and modern methods of prevention. Perm Medical Journal. 2019;36(3):72-90. (in Russian)]. https://dx.doi.org/10.17816/pmj36372-90.
- Пучкина Г.А., Сулима А.Н. Современные аспекты патогенеза и профилактики спаечного малого таза. Акушерство, гинекология и репродукция. 2020;14(4):523-33. [Puchkina G.A., Sulima A.N. Current aspects of pathogenesis and prophylaxis of pelvic adhesions. Obstetrics, Gynecology and Reproduction. 2020;14(4):523-33. (in Russian)].https://dx.doi.org/10.17749/2313-7347/ob.gyn.rep.2020.107.
- Moris D., Chakedis J., Rahnemai-Azar A.A., Wilson A., Hennessy M.M., Athanasiou A. et al. Postoperative abdominal adhesions: clinical significance and advances in prevention and management. J. Gastrointest. Surg. 2017;21(10):1713-22. https://dx.doi.org/10.1007/s11605-017-3488-9.
- Ghobrial S., Ott J., Parry J.P. An overview of postoperative intraabdominal adhesions and their role on female infertility: a narrative review. J. Clin. Med. 2023;12(6):2263. https://dx.doi.org/10.3390/jcm12062263.
- Малышкина А.И., Батрак Н.В. Острый живот в гинекологии: анализ структуры оперативных вмешательств при различных ургентных состояниях. Вестник Ивановской медицинской академии. 2021;26(3):44-7. [Malyshkina A.I., Batrak N.V. Acute abdomen in gynecology: analysis of operative interventions in different urgent states. Bulletin of the Ivanovo Medical Academy. 2021;26(3):44-7. (in Russian)]. https://dx.doi.org/10.52246/1606-8157_2021_26_3_44.
- Микляева И.А., Османов Э.М., Данилова И.К. Структура ургентной патологии и анализ оперативной активности гинекологического отделения. Вестник Ивановской медицинской академии. 2020;25(2):64-6. [Miklyaeva I.A., Osmanov E.M., Danilova I.K. The structure of urgent pathology and analysis of the operational activity of the gynecological department. Bulletin of the Ivanovo Medical Academy. 2020;25(2):64-6. (in Russian)].
- Есин Р.Г., Федоренко А.И., Горобец Е.А. Хроническая неспецифическая тазовая боль у женщин: мультидисциплинарная проблема (обзор). Медицинский альманах. 2017;5(50):97-101. [Esin R.G., Fedorenko A.I., Gorobets E.A. Chronic nonspecific pelvic pain in women: a multidisciplinary problem (review). Medical almanac. 2017;5(50):97-101. (in Russian)].
- Аюшинова Н.И., Шурыгина И.А., Григорьев Е.Г. Шкала оценки выраженности спаечного процесса брюшной полости. Acta Biomedica Scientifica. 2017;2(6):96-9. [Ayushinova N.I., Shurygina I.A., Grigoriev E.G. The rating scale for the severity of abdominal adhesions. Acta Biomedica Scientifica. 2017;2(6):96-9. (in Russian)]. https://dx.doi.org/10.12737/article_5a0a891f132b26.07816727.
- Магомедов М.М., Иманалиев М.Р., Магомедов М.А. Роль лапароскопических операций в формировании спаечного процесса в брюшной полости. Современная наука: актуальные проблемы теории и практики. Серия: Естественные и технические науки. 2021;8:180-7. [Magomedov M.M., Imanaliev M.R., Magomedov M.A. The role of laparoscopic surgery in the formation of the adhesion process in the abdominal cavity. Modern science: actual problems of theory and practice. Series: Natural and Technical Sciences. 2021;8:180-7. (in Russian)].
- Сулима А.Н., Пучкина Г.А. Оценка эффективности комплексного подхода к профилактике послеоперационного спаечного процесса. Российский медицинский журнал. Мать и дитя. 2021; 4(2):130-6. [Sulima A.N., Puchkina G.A. Evaluation of the effectiveness of an integrated approach to the prevention of postoperative adhesions. Russian Medical Journal. Mother and child. 2021; 4(2):130-6. (in Russian)]. https://dx.doi.org/10.32364/2618-8430-2021-4-2-130-136.
- Хамошина М.Б., Абитова М.З., Оразов М.Р., Оразмурадов А.А., Демина О.А., Исмаилзаде С.Я., Бабаева Э.И. Хирургическое лечение наружного гениального эндометриоза, как фактора риска снижения репродуктивного потенциала молодых женщин (по материалам гинекологического стационара). Акушерство и гинекология: новости, мнения, обучение. 2020;8(3) Приложение:55-60. [Khamoshina M.B., Abitova M.Z., Orazov M.R., Orazmuradov A.A., Demina O.A., Ismailzade S.Ya., Babaeva E.I. Surgical treatment of the external genital endometriosis as a risk factor for reducing young womens reproductive potential (based on the materials of the gynecological hospital). Obstetrics and Gynecology: News, Opinions, Training. 2020;8(3) Supplement:55-60. (in Russian)]. https://dx.doi.org/10.24411/2303-9698-2020-13909.
- The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil. Steril. 1988;49(6):944-55. https://dx.doi.org/10.1016/s0015-0282(16)59942-7.
- Shapiro S.S., Wilk M.B. An analysis of variance test for normality (complete samples). Biometrika. 1965;52(3-4):591-611. https://dx.doi.org/10.1093/biomet/52.3-4.591.
- Kruskal W.H., Wallis W.A. Use of ranks in one-criterion variance analysis. J. Am. Statistical Association. 1952; 47(260): 583-621.
- Dunn O.J. Multiple comparisons using rank sums. Technometrics. 1964;6(3):241-52. https://dx.doi.org/10.1080/00401706.1964.10490181.
- Holm S. A simple sequentially rejective multiple test procedure. Scan. J. Statis. 1979;6(2):65-70.
- Greenwood P.E., Nikulin M.S. A guide to chi-squared testing. NY: Wiley; 1996.
- Hammer Ø., Harper D.A., Ryan P.D. PAST: paleontological statistics software package for education and data analysis. Palaeontologia Electronica. 2001;4(1):9.
Received 26.10.2023
Accepted 27.12.2023
About the Authors
Anna N. Sulima, Dr. Med. Sci., Professor at the Department of Obstetrics, Gynecology and Perinatology No. 1, Order of Labor Red Banner Medical Institute named afterS.I. Georgievsky, V.I. Vernadsky Crimean Federal University, +7(978)764-82-00, gsulima@yandex.ru, Boulevard Lenina 5/7, 295051, Simferopol, Russia,
https://orcid.org/0000-0002-2671-6985
Oksana V. Gudz, Assistant at the Department of Obstetrics, Gynecology and Perinatology No. 1, Order of Labor Red Banner Medical Institute named after S.I. Georgievsky, V.I. Vernadsky Crimean Federal University, +7(978)772-02-92, pugovlaoks@mail.ru, Boulevard Lenina 5/7, 295051, Simferopol, Russia, https://orcid.org/0000-0002-48881-6792
Corresponding author: Anna N. Sulima, gsulima@yandex.ru
Similar Articles

