

First domestic experience of VR-intervention in endometriosis
Levakov S.A., Gromova T.A., Titova N.R., Gribkov S.V., Managadze I.J.
Endometriosis is a chronic inflammatory disease characterized by the presence of endometriosis-like tissues outside the uterus. This condition may be accompanied by psychosomatic and social discomfort, necessitating further research to understand the various factors that affect its development.
Objective: To present new data on the application of virtual reality (VR) technologies concerning the psychosomatic status of patients with endometriosis and highlight the dynamics of changes in the quality of life of women as a result of this intervention.
Materials and methods: This single-center prospective case series included four female patients diagnosed with endometriosis and/or adenomyosis. This represents the intermediate result of the 4-week VR intervention. The inclusion criteria were age between 18 and 49 years, a confirmed diagnosis of genital endometriosis of various locations through instrumental or histological diagnostic pathways, presence of chronic pelvic pain, absence of extragenital diseases, and consent to participate in the study.
Results: The reduction in anxiety and depression levels, along with decreased pain intensity, was confirmed by the changes in their condition as reported by the patients, coupled with improvements in quality of life observed in the study, indicating the potential for successful integration of virtual reality into multimodal treatment strategies for women with endometriosis.
Conclusion: This is the first domestic study to report the use of a medically supervised VR-solution designed to enhance psycho-emotional status and reduce pain in female patients with chronic pelvic pain associated with endometriosis. We hope that our experience can contribute to further research evaluating the effectiveness of VR-applications in this context and will facilitate comparisons of their effectiveness when combined with standard techniques using exclusively conservative approaches.
Authors' contributions: Levakov S.A. – conception and design of the study; Gromova T.A., Titova N.R., Gribkov S.V., Managadze I.J. – material collecting and analysis, drafting of the manuscript, statistical analysis, editing of the manuscript.
Conflicts of interest: The authors have no conflicts of interest to declare.
Funding: There was no funding for this study.
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Levakov S.A., Gromova T.A., Titova N.R., Gribkov S.V., Managadze I.J. First domestic experience of VR-intervention in endometriosis.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2025; (1): 82-87 (in Russian)
https://dx.doi.org/10.18565/aig.2024.187
Keywords
endometriosis
chronic pelvic pain
psychoemotional status
endometriosis treatment
psychological aspects of endometriosis
VR-interventions
Endometriosis is a chronic, multifactorial, dyshormonal, and inflammatory disease characterized by the proliferation of endometrial-like tissue outside the uterus [1]. It affects one in ten women, and its main clinical manifestations include dysmenorrhea, chronic pelvic pain, asthenia, and infertility. As endometriosis is a multisystemic condition, rather than solely a gynecological issue, it is crucial to investigate the psychosocial mechanisms underlying its development and to identify the role of psychoemotional status in the emergence of symptoms associated with this pathology. Future research should explore the relationship between psychoemotional factors that contribute to the development and progression of endometriosis as well as search for new therapeutic targets aimed at alleviating significant psychosomatic and social discomfort in affected women [2].
Standard drug therapies, including combined hormonal contraceptives, progestin, and gonadotropin-releasing hormone agonists, have proven effective in treating pain associated with endometriosis, but they also suppress ovulation and disrupt menstrual function [3, 4]. Despite their effectiveness, these methods do not lead to the disappearance of endometriotic lesions, particularly deep lesions, and their contraceptive effects render them unsuitable for women of reproductive age who are planning to conceive. For these women, only limited pain relief is recommended.
Surgery is typically not considered a first-line treatment and is indicated only in cases where drug treatment for pain is ineffective. However, pain relapse after surgery, especially in women who do not receive additional postoperative hormonal therapy, is common. The recurrence rate of postoperative endometriosis after 2-5 years varies based on the localization of the disease, ranging from 30% to 50% [5, 6].
The past few decades have witnessed the emergence of innovative digital therapeutic techniques (DTx) in medicine, aimed at using information technologies to broaden treatment and diagnostic methods and enhance their effectiveness. This trend has led to the development of a wide array of new therapeutic devices, including those employing immersive digital virtual reality (VR) technologies, for the treatment of acute and chronic pain [7].
Particular attention should be paid to the new digital therapeutic approach known as Endocare, which encompasses a variety of therapeutic procedures based on several modalities within a virtual reality environment, each designed to reduce pain. The Endocare therapeutic complex includes auditory components (e.g., alpha/theta binaural beats and nature sounds) and visual components (e.g., bilateral alternating stimulation) associated with a 3D VR environment. This multimodal strategy significantly reduces the intensity of pain in patients diagnosed with chronic pelvic pain associated with endometriosis [8].
Therefore, it is essential to broaden the range of therapeutic methods aimed at treating endometriosis and alleviating chronic pelvic pain. This expansion should ensure a comprehensive, patient-oriented therapeutic approach that includes both pharmacological interventions and psychosocial support, ultimately contributing to improved psychoemotional status, reduced pain intensity, and enhanced quality of life in women with endometriosis.
This study aimed to present new data on the application of VR technologies concerning the psychosomatic status of patients with endometriosis and highlight the changes in the quality of life of women resulting from this intervention.
Materials and methods
Four patients were selected for the study at the Center for Endometriosis and Pelvic Pain at Clinical Hospital No. 85 of FMBA of Russia. Inclusion criteria included women of reproductive age, between 18 and 49 years; an established diagnosis of genital endometriosis at various locations, confirmed by instrumental or histological diagnostic methods; the presence of chronic pelvic pain; the absence of extragenital diseases; and informed consent to participate in the study. The exclusion criteria included age inconsistent with the declared range, severe forms of endometriosis involving adjacent organs and structures, previous participation in endometriosis treatment using VR methods, and refusal to participate in the study. The patients were observed under the interdisciplinary supervision of obstetrician-gynecologists and psychologists at the center. At the time of the study, patients continued to receive their primary endometriosis therapy according to clinical guidelines (hormonal therapy).
The VR intervention was conducted using the Oculus Quest VR system during a 4-week follow-up. Every week, patients were invited to virtual reality sessions at the Center for Endometriosis and Pelvic Pain at Clinical Hospital No. 85 of the FMBA of Russia, which were conducted under the interdisciplinary supervision of gynecologists and psychologists. Each session involved a 20-minute immersion in virtual reality using VR goggles, featuring a stereoscopic image of real places and landscapes that simulated sensations of novelty and open spaces. The selection of the environment was based on patient preferences and wishes.
To assess psychoemotional status, intensity of chronic pelvic pain, and dynamics of these indicators, the following psychometric scales were used:
- Hospital Anxiety and Depression Scale (HADS). This scale is designed to diagnose clinically significant anxiety and depression and to differentiate between these affective disorders. The patients answered 14 questions, 7 for each subscale. Each question had four response options, with scores ranging from 0 to 3 points. The maximum score for each disorder is 21. A normal level of anxiety and depression corresponds to a score of 0 to 7 points, a subclinical level ranges from 8 to 10, and a score above 11 indicates a clinical level of anxiety or depression.
- The short form of the Endometriosis Health Profile (EHP-5) is a reliable and effective tool to assess the quality of life of patients with endometriosis. The psychometric scale contains five items that evaluate different aspects of life for women with endometriosis: pain, control, emotional components, social support, and self-esteem. Each question offered four response options rated from 0 (never) to 3 (always). The quality of life of women with endometriosis was assessed by summing the scores of all five questions, ranging from best possible health (0 points) to worst possible health (15 points), which is inversely proportional to the patient's quality of life.
- Visual analog pain scale (VAS). Patients rated the intensity of their pain using marks on a horizontal line from 0 to 10, where 0 represented no pain, 5 represented moderate pain, and 10 represented the worst pain imaginable.
- Pain relief assessment. Pain relief was rated after each session on a 5-point categorical scale (0 = no relief, 1 = slight relief, 2 = moderate relief, 3 = marked relief, and 4 = complete relief).
In this study, the assessment of anxiety and depression levels on the HADS scale and the quality of life of women with endometriosis on the EHP-5 scale was conducted before the first and after the last session. Pain intensity on the VAS scale and the degree of pain reduction were assessed before and after each session.
Results
The following are the data on the dynamics of the changes in the psychosomatic status of each patient.
Patient No. 1
Before the intervention, the first patient had the worst quality of life (15/15 points on the EHP-5 scale), clinical anxiety level (10/14 points on the HADS scale), and depression level at the upper limit of the norm (6/14 points on the HADS scale). At the end of the observation period, the quality of life increased by 33% (10/15 points on the EHP-5 scale), anxiety level decreased to the upper limit of the normal range (7/14 points on the HADS scale), and depression level also decreased to 4 points on the HADS scale. It should be noted that during the first three sessions, the level of chronic pelvic pain intensity, according to the VAS, remained unchanged at 2 points. Pain relief after the first session was absent (0 points on the Likert scale). After the second and third sessions, the difference was not statistically significant (one point). However, after the fourth session, the pain level became minimal, registering 1 point, while the degree of pain relief was moderate and noticeable (2 points out of 4 possible).
Patient No. 2
The second patient before the intervention had a satisfactory level of quality of life (4/15 points on the EHP-5 scale) and levels of anxiety and depression within the normal range (5 and 4 points on the HADS scale, respectively). By the end of the observation period, the quality of life had increased by 13.3% (2/15 points on the EHP-5 scale), the anxiety level had decreased by one unit to four points on the HADS scale, and the depression level remained unchanged. Although the intensity of chronic pelvic pain, as measured by the VAS, remained unchanged at 1 point during the intervention, pain relief after the first two sessions was insignificant (1 point on the Likert scale). However, after the third session, the patient reported complete relief (4 points of 4 possible).
Patient No. 3
Before the intervention, the third patient had an unsatisfactory quality of life (12/15 points on the EHP-5 scale), highest clinical level of anxiety (14/14 points on the HADS scale), and subclinical level of depression (9/14 points on the HADS scale). At the end of the observation period, quality of life improved by approximately 27% (8/15 points on the EHP-5 scale), while both anxiety and depression levels decreased, reaching the upper limit of the normal range (6/14 points on the HADS scale for both indicators). Notably, this patient exhibited a clear reduction in pain intensity. In the first session, the level of chronic pelvic pain, according to the VAS, was 4 points, with no relief after the first session (0 points on the Likert scale). After the second session, the pain intensity decreased to 3 points on the VAS, and the degree of pain relief became noticeable, albeit minor (1 point). Following the third session, pain intensity decreased by one unit to 2 points on the VAS, while the degree of pain relief was moderate and significant (2 points out of 4 possible).
Patient No. 4
Before the intervention, the fourth patient reported low quality of life (11/15 points on the EHP-5 scale) and subclinical levels of anxiety and depression (8/14 points on the HADS scale for both indicators). By the end of the observation period, the quality of life had improved to satisfactory levels, increasing by 47% (4/15 points on the EHP-5 scale). The anxiety level decreased to within the normal range (4/14 points on the HADS scale), while the depression level remained unchanged. Notably, during the first two sessions, the level of chronic pelvic pain intensity according to the VAS remained constant at 2 points, with minimal pain relief (1 point on the Likert scale). After the third session, the patient experienced moderate relief (2 out of 4 possible points), and pain intensity significantly decreased to 1 point on the VAS.
The study also predicted the dynamics of the changes in the assessed indicators and determined the optimal number of sessions needed to achieve the best psychosomatic status for each patient (Fig. 1–4).
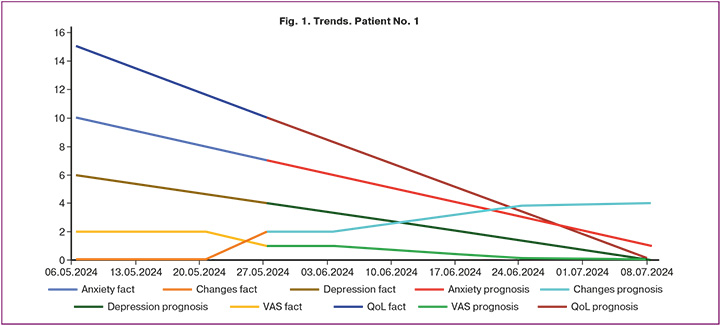
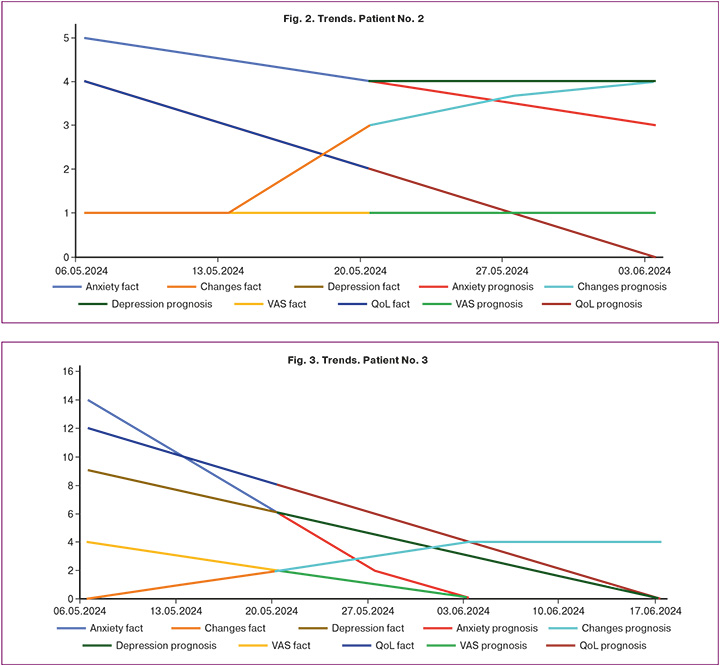
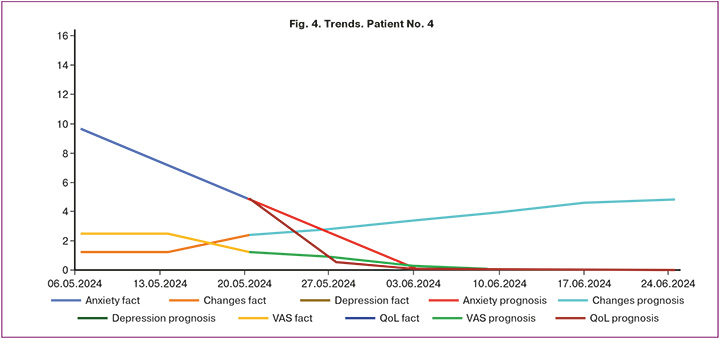
Thus, patient No. 1 requires 10 sessions to achieve optimal psychosomatic status, patient No. 2 needs 5 sessions, patient No. 3 requires 7 sessions, and patient No. 4 needs 8 sessions. This indicates that the approach to managing women in this population group should be personalized and patient oriented, taking into account their initial psychoemotional and somatic status.
Conclusion
This is the first domestic study to describe the use of VR methods under medical supervision, aimed at improving psychoemotional status and reducing pain intensity in patients with chronic pelvic pain associated with endometriosis. Although this study has limitations due to the small sample size, it was conducted under controlled conditions. The results demonstrated the potential effectiveness of VR solutions in enhancing the quality of life of patients with endometriosis as well as positive trends regarding the future use of this technique. A decrease in anxiety and depression, along with reduced pain intensity, as evident from the improvements reported by patients, indicates the potential for successful integration of virtual reality into multimodal treatment strategies for women with endometriosis. Long-term analysis and an expanded sample size would provide more insights into the impact of VR on the effectiveness of treatment of this condition. Therefore, further studies are needed to evaluate VR's effectiveness of VR and compare it with standard treatment methods, which will help determine the need to incorporate this strategy into a comprehensive approach for treating this patient population. We hope that our experience will contribute to the development of new approaches to patient-centered therapy for endometriosis, a psychosomatic, socially significant disease.
References
- Johnson N.P., Hummelshoj L., Adamson G.D., Keckstein J., Taylor H.S., Abrao M.S. et al.; World Endometriosis Society Sao Paulo Consortium. World Endometriosis Society consensus on the classification of endometriosis. Hum. Reprod. 2017; 32(2): 315-24. https://dx.doi.org/10.1093/humrep/dew293.
- Ferreira A.L.L., Bessa M.M.M., Drezett J., de Abreu L.C. Quality of life of the woman carrier of endometriosis: systematized review. Reprodução Clim. 2016; 31: 48-54. https://dx.doi.org/10.1016/j.recli.2015.12.002.
- Geoffron S., Cohen J., Sauvan M., Legendre G., Wattier J.M., Daraï E. et al. Traitement médical de l’endométriose: prise en charge de la douleur et de l’évolution des lésions par traitement hormonal. RPC Endométriose CNGOF-HAS [Endometriosis medical treatment: Hormonal treatment for the management of pain and endometriotic lesions recurrence. CNGOF-HAS Endometriosis Guidelines]. Gynecol. Obstet. Fertil. Senol. 2018; 46(3): 231-47. (in French). https://dx.doi.org/10.1016/j.gofs.2018.02.011.
- Legendre G., Delbos L., Hudon E., Chabbert-Buffet N., Geoffron S., Sauvan M. et al. Place des nouveaux traitements médicaux dans l’endométriose douloureuse, RPC Endométriose CNGOF-HAS [New medical treatments for painful endometriosis: CNGOF-HAS Endometriosis Guidelines]. Gynecol. Obstet. Fertil. Senol. 2018; 46(3): 256-63. (in French). https://dx.doi.org/10.1016/j.gofs.2018.02.009.
- Vercellini P., Frattaruolo M.P., Rosati R., Dridi D., Roberto A., Mosconi P. et al. Medical treatment or surgery for colorectal endometriosis? Results of a shared decision-making approach. Hum. Reprod. 2018; 33(2): 202-11. https://dx.doi.org/10.1093/humrep/dex364.
- Vercellini P., Buggio L., Frattaruolo M.P., Borghi A., Dridi D., Somigliana E. Medical treatment of endometriosis-related pain. Best Pract. Res. Clin. Obstet. Gynaecol. 2018; 51: 68-91. https://dx.doi.org/10.1016/j.bpobgyn.2018.01.015.
- Merlot B., Dispersyn G., Husson Z., Chanavaz-Lacheray I., Dennis T., Greco-Vuilloud J. et al. Pain reduction with an immersive digital therapeutic tool in women living with endometriosis-related pelvic pain: randomized controlled trial. J. Med. Internet. Res. 2022; 24(9): e39531. https://dx.doi.org/10.2196/39531.
- Merlot B., Elie V., Périgord A., Husson Z., Jubert A., Chanavaz-Lacheray I. et al. Pain reduction with an immersive digital therapeutic in women living with endometriosis-related pelvic pain: at-home self-administered randomized controlled trial. J. Med. Internet. Res. 2023; 25: e47869. https://dx.doi.org/10.2196/47869.
Received 01.08.2024
Accepted 25.12.2024
About the Authors
Sergey A. Levakov, Dr. Med. Sci., Professor, Head of the Department of Obstetrics and Gynecology, N.V. Sklifosovsky ICM, I.M. Sechenov First MSMU, Ministry of Health of Russia (Sechenov University), 119991, Russia, Moscow, Trubetskaya str., 8, bld. 2, +7(495)609-14-00, levakoff@yandex.ru, https://orcid.org/0000-0002-4591-838XTatyana A. Gromova, PhD, Teaching Assistant at the Department of Obstetrics and Gynecology of the Faculty of Medicine, I.M. Sechenov First MSMU, Ministry of Health of Russia (Sechenov University), 119991, Russia, Moscow, Trubetskaya str. 8, bld. 2, +7(495)609-14-00, tgromova928@yandex.ru, https://orcid.org/0000-0001-6104-9842
Nana R. Titova, Deputy Head of the Center for Endometriosis and Pelvic Pain, Head of the Consultative and Diagnostic Department, Clinical Hospital No. 85 of the FMBA of Russia, 115409, Russia, Moscow, Moskvorech'e str., 16, +7(499)782-85-85, titova_nana@mail.ru
Stanislav V. Gribkov, Head of the Department of Virtual and Augmented Reality, I.M. Sechenov First MSMU, Ministry of Health of Russia (Sechenov University), 119991, Russia, Moscow, Trubetskaya str., 8, bld. 2, +7(495)609-14-00.
Ioanna J. Managadze, Student at the N.V. Sklifosovsky ICM, I.M. Sechenov First MSMU, Ministry of Health of Russia (Sechenov University), 119991, Russia, Moscow, Trubetskaya str., 8, bld. 2, +7(495)609-14-00, ktb1966@mail.ru, https://orcid.org/0000-0001-8745-9372
Corresponding author: Sergey A. Levakov, levakoff@yandex.ru
Similar Articles

