
Fertility preservation in women with placenta accrete spectrum undergoing organ-sparing surgery
Relevance: Placenta accreta spectrum is a life-threatening pregnancy complication, significantly increasing maternal morbidity and mortality. Over the past decades, advances in organ-sparing surgical techniques for placenta accreta spectrum helped avoid hysterectomy in many women. However, the feasibility of preserving fertility in this group of patients has not been studied.Mikheeva A.A., Shmakov R.G., Rogachevskiy O.V., Yarygina T.A., Nizyaeva N. V., Amiraslanov E. Yu.
Results: This study analyzed the course and outcome of pregnancy in patients after organ-sparing surgery for morphologically confirmed placenta accreta spectrum. During 2014—2021, 10 pregnancies were observed in 9 patients who underwent organ-sparing operations for abnormal placental implantation. Only one patient was diagnosed with pregnancy in a scar and underwent surgical pregnancy termination at nine weeks gestation. One patient had two early pregnancy spontaneous miscarriages. The patients had a complicated obstetric and gynecologic history and a high rate of complications, including two cases of spontaneous miscarriage, preeclampsia, and fetal growth restriction. However, six pregnancies resulted in a live birth, including 5 cases of planned operative delivery at the V.I. Kulakov NMRC for OG&P of Ministry of Health of Russia and one case of emergency operative delivery at 33 weeks at the patient's residence for bleeding and suspected uterine scar dehiscence. One patient had ongoing uncomplicated pregnancy at the time of the study publication.
Conclusion: This pilot study analyzed the course of 10 pregnancies after placenta accreta spectrum metroplasty. Only one patient had a recurrent chorionic invasion into the uterine scar. Six patients gave live birth. Further research is needed to identify the risk factors for complications, develop predictive algorithms and methods to improve pregnancy outcomes in patients after metroplasty.
Keywords
pregnancy
placenta accreta spectrum
metroplasty
organ-preserving surgery
The realization of the female's reproductive potential is a natural human need. Radical organ-removing surgery is a direct barrier to reproduction and is a serious medical, social and demographic problem [1]. The placenta accreta spectrum is one of the leading causes of hysterectomies in women of reproductive age worldwide, with a current incidence rate of about 0.17% (1:588). It is steadily increasing [2, 3] due to the significant increase in the number of caesarian deliveries, which is a major risk factor for abnormal placental implantation and invasion into the uterine scar [4, 5]. More than half of operations for placenta accreta spectrum worldwide end in hysterectomy resulting in the loss of reproductive function [6, 7]. Uterine transplantation has recently emerged [8, 9] is still not a routine operation and remains an experimental treatment [10].
Innovative organ-sparing surgical techniques such as fundal transverse cesarean section with metroplasty and excision of the area of abnormal placental invasion [11, 12], which has been performed at the V.I. Kulakov NMRC for OG&P since 2014, offer significantly better chances of maintaining normal menstrual and reproductive function in patients with placenta accreta spectrum. Such surgical modalities have been developed due to modern proprietary techniques of surgical hemostasis, such as bilateral ligation of the internal iliac arteries, temporary occlusion of the common iliac arteries, and complex compression hemostasis [13, 14].
To date, 393 organ-sparing operations for the placenta accreta spectrum have been performed at the National Centre in pregnant women from different regions of Russia. Despite the expansive geography of the patients, the staff of the Centre continues monitoring their health not only in the early but also in the distant postoperative period, including monitoring the course and delivery of subsequent pregnancies. The latter is highly challenging due to the lack of accumulated international experience in managing and delivering women with a history of placenta accreta spectrum and organ-sparing surgery [15–17].
Results
Due to the remoteness of the regions, determining the actual number of pregnancies after organ-preserving treatment and metroplasty for the placenta accreta spectrum can be challenging. We analyzed the course and outcome of pregnancies in patients after organ-sparing surgery for morphologically confirmed placenta accreta spectrum, conducted at the V.I. Kulakov NMRC for OG&P. The study was approved by the Ethical Committee of the Centre.
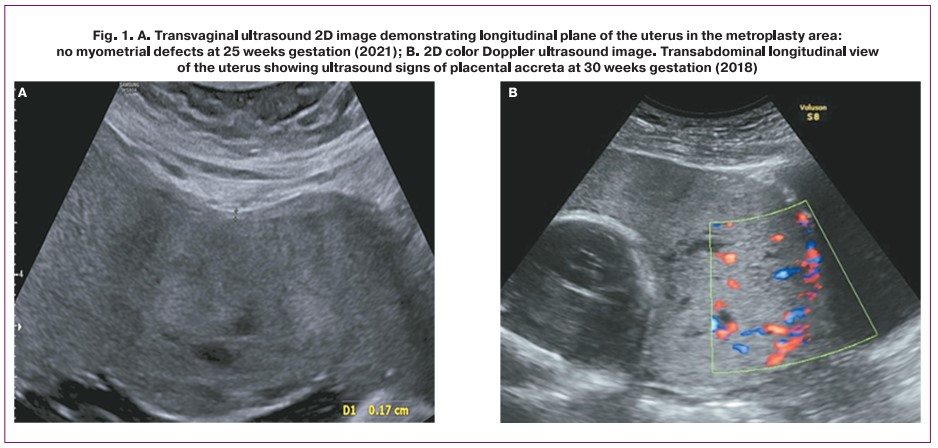
We analyzed medical history, clinical characteristics, and results of laboratory and diagnostic investigations of 9 patients who had pregnancies after metroplasty morphologically confirmed placenta accreta spectrum and medical records of 6 newborns. Ultrasound examination was performed on Voluson S6 Expert (GE Healthcare, Austria) and SAMSUNG MEDISON WS80A (Samsung Medison, South Korea) expert class systems using 3D\4D transabdominal convex multi-frequency (2–8 MHz) and 3D\4D intracavitary multi-frequency (5–13 MHz) probes (Fig. 1). Placental and myometrial tissue fragments were fixed for 24 hours in a 10% formalin buffered solution. Histological (hematoxylin and eosin staining) and Van Gieson's picrofuchsin (muscle tissue stained yellow and connective tissue stained red) were performed on serial paraffin sections.
Between 2014 and 2021, 9 patients who underwent organ-preserving surgery for the placenta accreta spectrum reported pregnancy. Their medical history and clinical characteristics are presented in Table 1. Five patients had multiple comorbidities, including chronic arterial hypertension, diabetes mellitus, anemia in pregnant women, kidney, liver, heart, and vascular disease, and bronchial asthma.
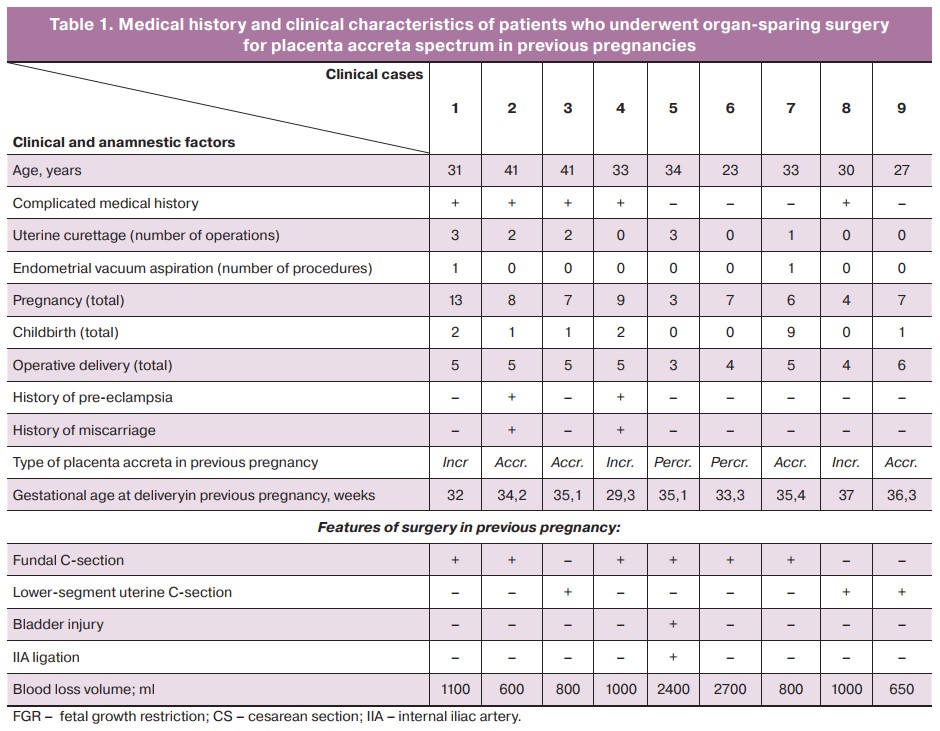
Worth noting is a high parity in this group of patients. Only one patient had her third pregnancy; 5 patients had 4 to 7 prior pregnancies; 3 had from 8 to 13 pregnancies and complicated obstetric-gynecological history. A total of 10 pregnancies were recorded in the study group; their specific course and outcomes are given in Table 2.

Consecutive pregnancy occurred one year after organ-sparing surgery in 5 patients, 3 patients after two years, and one after three years.
Only one patient was diagnosed with a Cesarean scar pregnancy and underwent a surgical termination at nine weeks. One patient had two pregnancies during the follow-up period that ended in spontaneous abortion at 5 and 20 weeks. One patient had an ongoing uncomplicated pregnancy at the time of publication of the study, with a gestational age of 16 weeks.
Of the six pregnancies that ended in delivery, in one case, there was operative emergency delivery at 33 weeks performed at the patient's place of residence for hemorrhage and suspected fundal scar dehiscence. Outpatient follow-up of 5 patients was performed at the V.I. Kulakov NMRC for OG&P. During the follow-up, 2 patients were diagnosed with moderate pre-eclampsia and late fetal growth restriction, but no clinical or ultrasound signs of scar dehiscence or placental accreta spectrum were found in any of the patients (Fig. 1).
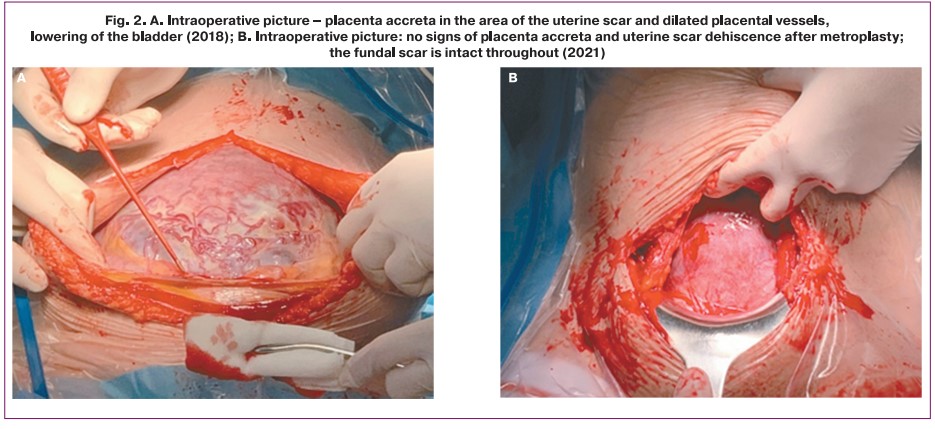
All five patients delivered routinely at 37–38 weeks' gestation at the V.I. Kulakov NMRC for OG&P (Fig. 2). No clinical signs of uterine scar dehiscence were observed at surgical delivery (Fig. 2B).
Histological examination of myometrium samples of the post-metroplasty lower uterine segment stained with hematoxylin and eosin, taken after cesarean section, was performed and compared with myometrial samples taken from the area outside the area of invasion and dense attachment, where no metroplasty was performed. The myometrium in the metroplasty area showed no signs of thinning or defects (Fig. 3), separated by thin interlayers of connective tissue, as confirmed by Van Gieson's picrofuchsin staining for connective tissue (Fig. 3); blood vessels of various diameters were present, with no thickened wall. This histological pattern was consistent with an uncomplicated pregnancy without significant tissue architectonics abnormalities. Histological examination of the myometrium in the area of the previously performed metroplasty confirmed that its structure was comparable to that of myometrium without placental invasion (Fig. 3). Thus, the myometrium samples after metroplasty with the restoration of the uterine wall integrity corresponded to myometrium with regular architectonics of smooth muscle fibers, a moderate number of vessels, the amount of connective tissue was not significantly increased. There were no signs of invasion and dense attachment, i.e., myometrium was comparable to myometrium without abnormal placentation. The postoperative period was without complications in all cases.
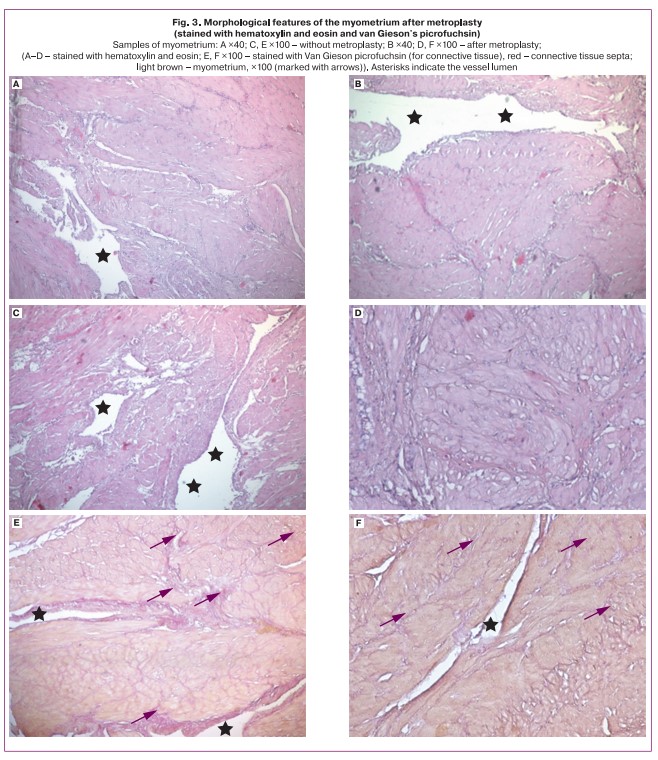
Samples of myometrium: A ×40; C, E ×100 without metroplasty; B ×40; D, F ×100 after metroplasty; (A–D – stained with hematoxylin and eosin; E, F ×100 – stained with Van Gieson picrofuchsin (for connective tissue), red – connective tissue septa; light brown – myometrium, ×100 (marked with arrows). Asterisks indicate the vessel lumen
Conclusion
In this pilot study of 10 pregnancies in 9 patients who underwent organ-sparing surgery for morphologically confirmed placenta accreta spectrum in a previous pregnancy, recurrent pathological chorionic invasion into the scar was detected in one patient. Of the six pregnancies that ended in delivery, most patients delivered as planned and had no hemorrhagic complications or clinical and histological signs of myometrial dehiscence. Despite a complicated obstetric history and a high incidence of complications, such as spontaneous miscarriage, preeclampsia, fetal growth restriction, and anemia, six patients gave birth to live-viable babies. Further research is needed to assess the factors influencing the development of complications and to develop predictive algorithms and methods to improve pregnancy outcomes in post-metroplasty patients.
References
- Sukhikh G.T., Stenyaeva N.N. Reproduction and sexuality. Obstetrics and Gynecology. 2014; 7: 4-8. (in Russian).
-
De Mucio B., Serruya S., Alemán A., Castellano G., Sosa C.G. A systematic review and meta-analysis of cesarean delivery and other uterine surgery as risk factors for placenta accreta. J. Gynaecol. Obstet. 2019; 147(3): 281-91.
https://dx.doi.org/10.1002/ijgo.12948.
- Poder L., Weinstein S., Maturen K.E., Feldstein V.A., Mackenzie D.C., Oliver E.R. et al.; Expert Panel on Women’s Imaging. ACR Appropriateness criteria® placenta accreta spectrum disorder. J. Am. Coll. Radiol. 2020; 17(5, Suppl.): S207-14. https://dx.doi.org/10.1016/j.jacr.2020.01.031.
- Morlando M., Buca D., Timor-Tritsch I., Cali G., Palacios-Jaraquemada J., Monteagudo A. et al. Reproductive outcome after cesarean scar pregnancy: A systematic review and meta-analysis. Acta Obstet. Gynecol. Scand. 2020; 99(10): 1278-89. https://dx.doi.org/10.1111/aogs.13918.
-
Wei J., Dai Y., Wang Z., Gu N., Ju H., Xu Y. et al. Intrauterine double-balloon tamponade vs gauze packing in the management of placenta previa: A multicentre randomized controlled trial. Medicine (Baltimore). 2020; 99(7): e19221.
https://dx.doi.org/10.1097/MD.0000000000019221.
-
Timmermans S., van Hof A.C., Duvekot J.J. Conservative management of abnormally invasive placentation. Gynecol. Surv. 2007; 62(8): 529-39.
https://dx.doi.org/10.1097/01.ogx.0000271133.27011.05.
-
Hecht J.L., Baergen R., Ernst L.M., Katzman P.J., Jacques S.M., Jauniaux E. et al.
Classification and reporting guidelines for the pathology diagnosis of placenta accreta spectrum (PAS) disorders: recommendations from an expert panel. Pathol. 2020; 33(12): 2382-96. https://dx.doi.org/10.1038/s41379-020-0569-1.
- Brännström M., Dahm Kähler P., Greite R., Mölne J., Díaz-García C., Tullius S.G. Uterus Transplantation: a rapidly expanding field. Transplantation. 2018; 102(4): 569-77. https://dx.doi.org/10.1097/TP.0000000000002035.
-
Tardieu A., Dion L., Collinet P., Ayoubi J.M., Garbin O., Agostini A. et al.; CNGOF French Uterus Transplantation Committee (CETUF). Uterus transplantation: Which indications? J. Gynecol. Hum. Reprod. 2019; 48(1): 7-8.
https://dx.doi.org/10.1016/j.jogoh.2018.10.003.
- Brännström M., Kurtser M.A., Polstyanoy A.M., Gubarev K.K. Uterus transplantation – the current state of the problem in the world (literature review). Reproduction problems. 2019; 25(5): 15-21. (in Russian). https://dx.doi.org/10.17116/ repro20192505115.
- Shmakov R.G., Pirogova M.M., Vasilchenko O.N., Chuprynin V.D., Pyregov A.V., Khodzhaeva Z.S., Klimenchenko N.I., Fedorova T.A., Ezhova L.S., Bychenko V.G., Boykova Yu.V. Organ-preserving operations in case of abnormal invasion of the placenta (5-year experience of the National Medical Research Center for Obstetrics, Gynecology and Perinatology named after Academician V.I. Kulakov). Doctor.Ru. 2019; 11(166): 29-34. (in Russian). https://dx.doi.org/10.31550/1727-2378-2019-166-11-29-34.
- Shmakov R.G., Pirogova M.M., Vasilchenko O.N., Chuprynin V.D., Ezhova L.S. Surgical tactics for ingrowth of the placenta with different depths of invasion. Obstetrics and gynecology. 2020; 1: 78-82. (in Russian). https://dx.doi.org/10.18565/aig.2020.1.78-82.
- Shahin A.Y., Farghaly T.A., Mohamed S.A., Shokry M., Abd-El-Aal D.E.M., Youssef M.A. Bilateral uterine artery ligation plus B-Lynch procedure for atonic postpartum hemorrhage with placenta accreta. J. Gynaecol. Obstet. 2010; 108(3): 187-90. https://dx.doi.org/10.1016/j.ijgo.2009.08.035.
- Vinitskiy A.A., Shmakov R.G., Chuprynin V.D. Comparative evaluation of the effectiveness of surgical hemostasis methods for organ-preserving delivery in patients with placental ingrowth. Obstetrics and gynecology. 2017; 7: 68-74. (in Russian). https://dx.doi.org/10.18565/aig.2017.7.68-74.
- Roeca C., Little S.E., Carusi D.A. Pathologically diagnosed placenta accreta and hemorrhagic morbidity in a subsequent pregnancy. Obstet. Gynecol. 2017; 129(2): 321-6. https://dx.doi.org/10.1097/AOG.0000000000001843.
- Baldwin H.J., Nippita T.A., Torvaldsen S., Ibiebele I., Ford J.B., Patterson J.A. Outcomes of subsequent births after placenta accreta spectrum. Obstet. Gynecol. 2020; 136(4): 745-55. https://dx.doi.org/10.1097/AOG.0000000000004051.
- Vinograd A., Wainstock T., Mazor M., Mastrolia S.A., Beer-Weisel R., Klaitman V., Erez O. A prior placenta accreta is an independent risk factor for post-partum hemorrhage in subsequent gestations. Eur. J. Gynecol. Reprod. Biol. 2015; 187: 20-4. https://dx.doi.org/10.1016/j.ejogrb.2015.01.014.
Received 29.11.2021
Accepted 14.12.2021
About the Authors
Alexandra A. Mikheeva, Ph.D. Student, V.I. Kulakov NMRC for OG&P, Ministry of Health of the Russian Federation, shuratora@mail.ru, https://orcid.org/0000-0002-8159-6373, 117997, Russia, Moscow, Oparina str., 4.Roman G. Shmakov, Dr. Med. Sci., Professor, Director of the Institute of Obstetrics, V.I. Kulakov NMRC for OG&P, Ministry of Health of the Russian Federation, +7(495)438-72-00, r_shmakov@oparina4.ru, https://orcid.org/0000-0002-2206-1002, 117997, Russia, Moscow, Oparina str., 4.
Oleg V. Rogachevskiy, Dr. Med. Sci., Head of the Department of Extracorporal Methods of Treatment and Detoxification, Professor at the Department of Anesthesiology and Resuscitation, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation, +7(495)438-71-35, о_rogachevskiy@oparina4.ru, https://orcid.org/0000-0002-4332-430X, 117997, Russia, Moscow, Oparina str., 4.
Tamara A. Yarygina, PhD, Diagnostic Medical Sonographer, Researcher, Perinatal Cardiology Center of A.N. Bakulev NMRC, +7(495)414-78-75, tamarayarygina@gmail.com, https://orcid.org/0000-0001-6140-1930, 121552, Russia, Moscow, Roublyevskoe Shosse, 135.
Natalia V. Nizyaeva, PhD, Senior Researcher at the Department of Anatomic Pathology, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation, +7(926)248-28-93, niziaeva@gmail.com, https://orcid.org/0000-0001-5592-5690, SPIN 9893-2630, 117997, Russia, Moscow, Oparina str., 4.
Elrad Yu. Amiraslanov, PhD, Head of the Department of Obstetrics, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation, eldis@mail.ru, https://orcid.org/0000-0001-5601-1241, 117997, Russia, Moscow, Oparina str., 4.
Authors' contributions: Mikheeva A.A., Yarygina T.A., Shmakov R.G., Rogachevskiy O.V. - conception and design of the study; Mikheeva A.A., Yarygina T.A., Nizyaeva N.V., Amiraslanov E.Yu. - data collection and analysis, manuscript drafting; Mikheeva A.A., Yarygina T.A., Amiraslanov E.Yu. - data analysis; Shmakov R.G., Rogachevskiy O.V. - manuscript editing. Conflicts of interest: The authors have no conflicts of interest to declare.
Funding: There was no funding for this study.
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Mikheeva A.A., Shmakov R.G., Rogachevskiy O.V., Yarygina T.A., Nizyaeva N. V., Amiraslanov E. Yu. Fertility preservation in women with placenta accreta spectrum undergoing organ-sparing surgery. Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2022; 1:90-96 (in Russian) https://dx.doi.org/10.18565/aig.2022.1.90-96
Similar Articles

