

Gam-COVID-Vac (Sputnik V) vaccine has no adverse effect on spermatogenesis in men
Relevance. During the pandemic and large-scale vaccination against COVID-19, studies of the effect of various types of vaccines on human reproductive function have become particularly important. Vaccination may have a negative impact on the reproductive organs and tissues due to the development of an autoimmune process involving the gonads. Currently, there are some studies on the effect of vaccination against coronavirus infection caused by SARS-CoV2 on the male and female reproductive function. The absence of a negative effect of vaccination on spermatogenesis in men has already been demonstrated in the results of three studies.Drapkina Yu.S., Dolgushina N.V., Shatylko T.V., Nikolaeva M.A., Menzhinskaya I.V., Ivanets T.Yu., Krechetova L.V., Gamidov S.I., Bairamova G.R., Sukhikh G.T.
Objective. To evaluate the effect of the Gam-COVID-Vac (Sputnik V) vaccine on spermatogenesis and the level of antiphospholipid antibodies in men.
Materials and methods. The prospective study included 45 men who were vaccinated against COVID-19 with Gam-COVID-Vac (Sputnik V). The criteria for inclusion in the study were the age from 18 to 55 years, the absence of a previous history of COVID-19, a negative RT-PCR result in SARS-CoV-2 testing, negative SARS-CoV-2 IgG results prior to vaccination, and the absence of severe somatic diseases. The patients were examined twice: immediately before vaccination and 90 days after the first dose was injected. We evaluated spermogram parameters, determined the levels of FSH, LH, TSH and total testosterone, and analyzed blood for IgM and IgG antiphospholipid antibodies (aPL) to cardiolipin (aCL), β2-glycoprotein-1 (aß2-GP1), annexin V (aAnV), phosphatidylserine (aPS), as well as IgG antibodies to SARS-CoV-2 using enzyme immunoassay.
Results. There were no significant changes in the parameters of spermogram and hormone levels before and after vaccination; men with moderate impairment of spermatogenesis (oligoasteno- and/or teratozoospermia) did not show considerable changes either. The level of aPL after vaccination did not increase compared to the baseline level. Besides, there was no correlation between the dynamics of the level of antisperm antibodies, aPL and spermogram parameters. These findings indirectly indicate that there are no changes in the reproductive function associated with this autoimmune factor after vaccination in men.
Conclusion. This is one of the first studies that has revealed the effect of the Gam-COVID-Vac vaccine on spermatogenesis, hormonal profile and aPL level in men. The obtained results demonstrate that the Gam-COVID-Vac vaccine does not have a negative effect on the reproductive function in men.
Keywords
vector-based vaccine
COVID-19
SARS-CoV-2
Gam-COVID-Vac (Sputnik V)
spermatogenesis
testosterone
autoimmune conditions
antiphospholipid antibodies
One of the most effective ways to prevent a new coronavirus infection SARS-CoV-2 is vaccination. The Gam-Covid-Vac vaccine containing a fragment of the SARS-CoV-2 genetic material was registered in 2020 [1]. Nowadays, people all over the world are vaccinated against the new coronavirus infection SARS-CoV-2, but the proportion of vaccinated people in different countries ranges from 75.6% (Malta) to 0.01% (Uganda). The proportion of the vaccinated population in Russia was 12.19% as of July 05, 2021 (https://yandex.ru/covid19/stat). Despite the confirmed high effectiveness of Gam-Covid-Vac in the prevention of severe forms of new coronavirus infection, a lot of men are concerned about the possible impact of vaccination on their reproductive health. Since vaccination may affect the development of autoimmune diseases involving gonads, the study of the influence of Gam-Covid-Vac on the reproductive health has been initiated [2–4].
For the entire period of vaccination, little data on the effect of various types of vaccines on human reproductive function has been collected in the literature [5–7]. Gam-Covid-Vac is a combined vector vaccine based on an adenovirus vector. Talotta et al. suggested in his study published in 2021 that vaccines based on adenovirus vectors can cause impaired regulation of the synthesis of type I interferons (IFN) [8]. Changes in the synthesis of type I IFN can theoretically lead to immuno-inflammatory rheumatic diseases, including systemic lupus erythematosus (SLE), antiphospholipid syndrome (APS) and rheumatoid arthritis (RA) [9].
Bin Wang et al. (2017) performed a meta-analysis of 16 observational studies and found that vaccination increases the risk of developing SLE and RA [10]. Moreover, it was experimentally established that the administration of tetanus toxoid together with adjuvants in Th1 and Th2 prone mice was accompanied by the development of APS [11, 12]. The potential influence of vaccination on the development of immuno-inflammatory rheumatic diseases and consequently on the male reproductive health allows us to take a new look on the pathogenesis of autoimmune reactions developing in predisposed individuals in response to the introduction of adjuvant substances into the body (ASIA-syndrome). Currently, there are some studies on the effect of vaccination against coronavirus infection caused by SARS-CoV-2 on the male and female reproductive function (www.clinicaltrials.gov). The absence of a negative effect of vaccination on spermatogenesis in men has already been demonstrated in the results of the recent studies [13–15]. Therefore, the study of the effect of the vaccine against COVID-19 on the male reproductive function is of particular relevance. Due to the fact that among all Russian vaccines, only Gam-COVID-Vac (Sputnik V) has passed all the stages of clinical trials, it was chosen for studying the effect of vaccination on spermatogenesis in men [16].
The aim of the study was to evaluate the effect of the Gam-COVID-Vac (Sputnik V) vaccine on spermatogenesis, hormonal profile and the level of antiphospholipid antibodies in men.
Materials and methods
The prospective study included 45 men who were vaccinated against COVID-19 with Gam-COVID-Vac (Sputnik V). The criteria for inclusion in the study were the age from 18 to 55 years, normal or subnormal parameters of the spermogram before vaccination, the absence of a previous history of COVID-19, a negative RT-PCR result in SARS-CoV-2 testing, negative SARS-CoV-2 IgG results prior to vaccination. The criteria for non-inclusion were contraindications to vaccination according to the instructions, oncological diseases of any localization, rheumatic and autoimmune diseases, tuberculosis, chronic systemic infections, a history of allergic diseases, hormone therapy and any vaccination carried out 30 days before inclusion in the study, treatment with immunoglobulins and immunomodulatory drugs 3 months before inclusion in the study. The exclusion criteria were COVID-19 during the vaccination period, a severe undesirable reaction resulting in the cancelled 2nd dose of the vaccine, and the patient’s refusal to continue vaccination.
The concentration of luteinizing hormone (LH), follicle-stimulating hormone (FSH), and total testosterone was determined in blood serum with an electrochemiluminescent method on an automatic immunochemical analyzer “Cobas e411” (Roche Diagnostics GmbH, Germany) using commercial kits from this manufacturer. The concentration of thyroid-stimulating hormone (TSH) was determined in blood serum using an immunochemiluminescent method on an automatic immunochemical analyzer “IMMULITE 2000” (Siemens, USA). The analysis of blood for IgM and IgG antiphospholipid antibodies (aPL) to cardiolipin (aCL), β2-glycoprotein-1 (aß2-GP1), annexin V (aAnV), phosphatidylserine (aPS) was carried out with enzyme immunoassay using “ORGENTEC Diagnostika” kits (Germany). Also, IgG antibodies to SARS-CoV-2 in blood serum were determined with enzyme immunoassay using the test system “A set of reagents for detecting IgG specific to SARS-CoV-2 spike using enzyme immunoassay” (RPC “Diagnostic Systems”, Russia). The results were assessed using spectrophotometer “Infinite F50” (TECAN, USA).
According to the WHO laboratory manual [17], reference values of ejaculate parameters were used for evaluating sperm pathology (Table 1).
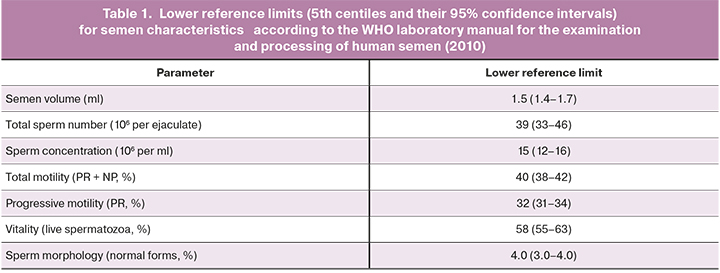
Sperm pathology had the following criteria:
- oligozoospermia characterized by a decrease in the concentration of spermatozoa <15 mln/ml;
- asthenozoospermia characterized by a decrease in sperm motility below normal values (total motility <40%, spermatozoa with progressive movement <32%);
- teratozoospermia characterized by an increase in the number of spermatozoa with abnormal morphology (96%).
Additionally, the number of IgG antisperm antibodies was determined using latex particles on the surface of spermatozoa (norm ≤ 50%); DNA fragmentation of spermatozoa was identified using the TUNEL method (norm <15%).
Statistical analysis
The statistical software package Statistica 10 (USA) was used for statistical analysis. The data were represented as absolute values and % for categorical data, medians (with an interquartile interval) for quantitative data. Medians were compared using pairwise testing methods, namely, paired Wilcoxon test for related samples due to the abnormal distribution of data for all values. Normal distribution of the data was evaluated using the Shapiro–Wilk criterion. The correlation was analyzed using Spearman’s criterion. The differences between the statistical values were considered statistically significant at р˂0.05.
The study was approved by the Local Ethics Committee of the Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Moscow, Russia.
Results
The average age of the men was 36.0 (30.0–44.0) years, the body mass index (BMI) was 25.9 (23.5–28.7) kg/m2. The assessment of clinical and anamnestic data revealed that the morbidity of patients was low: bronchial asthma was noted in 2 patients (4.4%), arterial hypertension – in 1 (2.2%), chronic tonsillitis – in 2 (4.4%), chronic gastritis – in 3 (6.7%), chronic prostatitis – in 3 (6.7%), pollinosis – in 3 men (6.7%).
The vaccine was generally well tolerated by the patients, there were no serious adverse events associated with the injection of the vaccine. The reaction to the vaccine was more frequently observed after injecting the 2nd dose and was short-term (1–2 days). Local reaction at the injection site was observed in 7 patients (15.5%), subfebrile temperature was noted in 43 (95.5%), intoxication symptoms such as headache and/or myalgia were observed in 13 cases (28.9%).
SARS-CoV-2 IgG antibodies were detected in almost all vaccinated patients, only in 3 (6.7%) patients their level did not reach the threshold value for positivity.
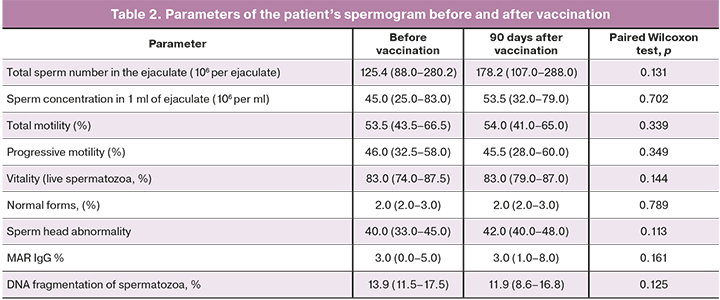
The comparison of the average parameters of the spermogram before and after vaccination did not reveal significant differences, including the level of MAR IgG and DNA fragmentation of spermatozoa (Table 2).
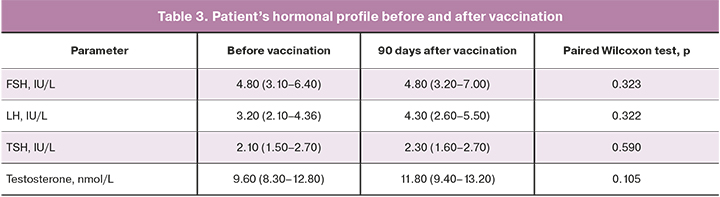
 The analysis of the dynamics of the spermogram parameters before and after vaccination in men with pathospermia (n=17) compared to men with normospermia (n=28) did not reveal a significant difference. The delta of sperm concentration in 1 ml of ejaculate in patients with pathospermia was 0.5 (-19.0–8.7), in patients with normospermia – 7.0 (-11.0–29.0) (p>0.05). The delta of total sperm motility in patients with pathospermia was –3.0 (-5.0–1.0)%, in patients with normospermia –3.0 (-5.0–1.0)% (p>0.05). The delta of the number of normal sperm forms in patients with pathospermia was 0.0 (0.0–0.0), with normospermia – 0.0 (0.0–0.0) (p>0.05). Leukocytospermia with a white blood cell concentration of more than 1 million/ml was not revealed in any patient either before or after vaccination. The comparison of the average parameters of the patient’s hormonal profile before and after vaccination did not show any significant differences in the parameters (Table 3).
The analysis of the dynamics of the spermogram parameters before and after vaccination in men with pathospermia (n=17) compared to men with normospermia (n=28) did not reveal a significant difference. The delta of sperm concentration in 1 ml of ejaculate in patients with pathospermia was 0.5 (-19.0–8.7), in patients with normospermia – 7.0 (-11.0–29.0) (p>0.05). The delta of total sperm motility in patients with pathospermia was –3.0 (-5.0–1.0)%, in patients with normospermia –3.0 (-5.0–1.0)% (p>0.05). The delta of the number of normal sperm forms in patients with pathospermia was 0.0 (0.0–0.0), with normospermia – 0.0 (0.0–0.0) (p>0.05). Leukocytospermia with a white blood cell concentration of more than 1 million/ml was not revealed in any patient either before or after vaccination. The comparison of the average parameters of the patient’s hormonal profile before and after vaccination did not show any significant differences in the parameters (Table 3).
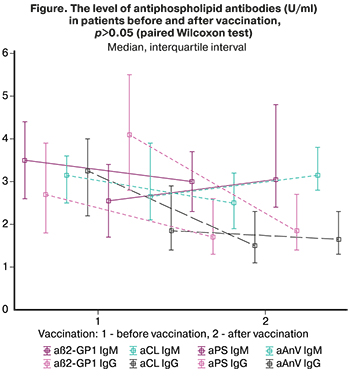
The level of aPL was subsequently analyzed before and after vaccination (Figure). There was a slight decrease in the level of aß2-GP1 IgG, aCL IgM and aPS IgG after vaccination compared to the baseline values. The level of aPL did not exceed the reference values in all patients.
There was a correlation analysis of the dependence of changes in the parameters of the spermogram (total sperm number, total sperm motility, viability, percentage of morphologically normal forms, percentage of progressively mobile forms) and IgM and IgG aPL to aCL, aß2-GP1, aAnV and aPS. The results of this analysis did not reveal any significant correlations (r<0.20, p>0.05). The vaccine has no effect on spermatogenesis in men, but there is evidence of a negative effect of COVID-19 on the male reproductive function. The analysis revealed a wide representation of receptors for SARS-CoV-2 (angiotensin-converting enzyme (ACE2), transmembrane serine protease 2 (TMPRSS2), CD147 (basigin) in human reproductive organs and tissues [18–22]. It should be emphasized that spike protein of SARS-CoV-2 binds to the ACE2 receptor contributing to the penetration of the virus into the target cell [23]. The study of Haghpanah A. et al. showed that the penetration of the SARS-CoV-2 virus into spermatogonia, Leydig cells, as well as Sertoli cells can lead to the changes in the level of sex hormones, increased DNA fragmentation, and decreased sperm motility [24]. The results of other studies confirm the negative impact of COVID-19 on spermatogenesis [25] and hormonal profile of men [26]. It cannot be excluded that the interaction of the SARS-CoV-2 virus with the ACE2 receptor can initiate the development of specific epididymo-orchitis due to the development of systemic vasculitis [27, 28].
Conclusion
This is one of the first studies that has revealed the effect of the Gam-COVID-Vac vaccine on spermatogenesis, hormonal profile and aPL level in men. All patients included in the study initially had normal or subnormal spermogram parameters and did not experience any severe somatic diseases. Factors that could influence the excessive autoimmune response were also excluded from the study.
According to the preliminary data of the study, Gam-COVID-Vac does not have a negative effect on spermatogenesis and hormonal profile in men, including men with moderate pathospermia (oligoasteno- and/or teratozoospermia). Moreover, vaccination does not cause an increase in the level of aPL, as well as antisperm antibodies (MAR), which may indirectly be indicative of the absence of changes in the reproductive function of autoimmune genesis under the influence of the vaccine. The research will continue and further study will include 200 men.
References
- Минздрав России зарегистрировал первую в мире вакцину от COVID-19. Министерство здравоохранения Российской Федерации11.08.2020. Дата обращения: 11 августа 2020 г. Архивировано 12 августа 2020 г. [The Russian Ministry of Health has registered the world's first vaccine against COVID-19. Ministry of Health of the Russian Federation (11.08.2020). Circulation date: August 11, 2020 Archived August 12, 2020. (in Russian)].
- Перминова С.Г. Бесплодие у женщин с аутоиммунной патологией щитовидной железы. Медицинский совет. 2012; 7: 40-4. [Perminova S.G. Infertility in women with autoimmune thyroid pathology. Medical Council. 2012; 7: 40-4. (in Russin)].
- Toussirot É., Bereau M. Vaccination and induction of autoimmune diseases. Inflamm. Allergy Drug Targets. 2015; 14(2): 94-8. https://dx.doi.org/10.2174/1871528114666160105113046.
- Зайцевская С.А., Долгушина Н.В., Сухих Г.Т. Влияние вакцин на репродуктивную систему. Акушерство и гинекология. 2020; 9: 5-10. https://dx.doi.org/10.18565/aig.2020.9.5-10. [Zaitsevskaya S.A., Dolgushina N.V., Sukhikh G.T. The effect of vaccines on the reproductive system. Odstetrics and Gynecology. 2020; 9: 5-10. (in Russian)]. https://dx.doi.org/10.18565/aig.2020.9.5-10.
- Wacholder S., Chen B.E., Wilcox A., Macones G., Gonzalez P., Befano B. et al. Risk of miscarriage with bivalent vaccine against human papillomavirus (HPV) types 16 and 18: pooled analysis of two randomised controlled trials. BMJ. 2010; 340: c712. https://dx.doi.org/10.1136/bmj.c712.
- Panagiotou O.A., Befano B.L., Gonzalez P., Rodríguez A.C., Herrero R., Schiller J.T. et al. Effect of bivalent human papillomavirus vaccination on pregnancy outcomes: long term observational follow-up in the Costa Rica HPV vaccine trial. BMJ. 2015; 351: h4358. https://dx.doi.org/10.1136/bmj.h4358.
- Wiesen A.R., Littell C.T. Relationship between prepregnancy anthrax vaccination and pregnancy and birth outcomes among US army women. JAMA. 2002; 287(12): 1556-60. https://dx.doi.org/10.1001/jama.287.12.1556.
- Talotta R., Robertson E.S. Antiphospholipid antibodies and risk of post-COVID-19 vaccination thrombophilia: The straw that breaks the camel's back? Cytokine Growth Factor Rev. 2021; 60: 52-60. https://dx.doi.org/10.1016/j.cytogfr.2021.05.001.
- Насонов Е.Л., Авдеева А.С. Иммуновоспалительные ревматические заболевания, связанные с интерфероном типа I: новые данные. Научно-практическая ревматология. 2019; 55(4): 452-61. [Nasonov E.L., Avdeeva A.S. Immuno-inflammatory rheumatic diseases associated with interferon type I: new data. Scientific and practical rheumatology. 2019; 55(4): 452-61. (in Russian)].
- Wang B., Shao X., Wang D., Xu D., Zhang J.A. Vaccinations and risk of systemic lupus erythematosus and rheumatoid arthritis: A systematic review and meta-analysis. Autoimmun. Rev. 2017; 16(7): 756-65. https://dx.doi.org/10.1016/j.autrev.2017.05.012.
- Zivkovic I., Stojanovic M., Petrusic V., Inic-Kanada A., Dimitrijevic L. Induction of APS after TTd hyper-immunization has a different outcome in BALB/c and C57BL/6 mice. Am. J. Reprod. Immunol. 2011; 65(5): 492-502. https://dx.doi.org/10.1111/j.1600-0897.2010.00922.x.
- Cruz-Tapias P., Blank M., Anaya J.M., Shoenfeld Y. Infections and vaccines in the etiology of antiphospholipid syndrome. Curr. Opin. Rheumatol. 2012; 24(4): 389-93. https://dx.doi.org/10.1097/BOR.0b013e32835448b8.
- Safrai M., Reubinoff B., Ben-Meir A. BNT162b2 mRNA Covid-19 vaccine does not impair sperm parameters. medRxiv preprint. May, 2021. https://dx.doi.org/10.1101/2021.04.30.21255690.
- Елагин В.В., Адамян Л.В., Вечорко В.И., Дорошенко Д.А., Дашко А.А., Филиппов О.С., Степанян А.А., Медведева И.В. Вакцинация против COVID-19 и репродуктивное здоровье мужчин (предварительные данные). Проблемы репродукции. 2021; 27(4). https://dx.doi.org/10.17116/repro2021270410. [Elagin V.V., Adamyan L.V., Vechorko V.I., Doroshenko D.A. et al. Vaccination against COVID-19 and reproductive health of men (preliminary data). Russian Journal of Human Reproduction. 2021; 27(4). (in Russin)]. https://dx.doi.org/10.17116/repro2021270410.
- Gonzalez D.C., Nassau D.E., Khodamoradi K., Ibrahim E., Blachman-Braun R., Ory J., Ramasamy R. Sperm parameters before and after COVID-19 mRNA vaccination. JAMA. 2021 Jun 17. https://dx.doi.org/10.1001/jama.2021.9976. Online ahead of print.
- Logunov D.Y., Dolzhikova I. V, Shcheblyakov D. V, Tukhvatulin A.I., Zubkova O.V., Dzharullaeva A.S. et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: an interim analysis of a randomised controlled phase 3 trial in Russia. Lancet. 2021; 397(10275): 671-81. https://dx.doi.org/10.1016/S0140-6736(21)00234-8.
- World Health Organization. WHO laboratory manual for the examination and processing of human semen. 5th ed. 2010. 287p.
- Li M.Y., Li L., Zhang Y., Wang X.S. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect. Dis. Poverty. 2020; 9(1): 45. https://dx.doi.org/10.1186/s40249-020-00662-x.
- Jing Y., Run-Qian L., Hao-Ran W., Hao-Ran C., Ya-Bin L., Yang G. et al. Potential influence of COVID-19/ACE2 on the female reproductive system. Mol. Hum. Reprod. 2020; 26(6): 367-73. https://dx.doi.org/10.1093/molehr/gaaa030.
- Smedts A.M., Lele S.M., Modesitt S.C., Curry T.E. Expression of an extracellular matrix metalloproteinase inducer (basigin) in the human ovary and ovarian endometriosis. Fertil. Steril. 2006; 86(3): 535-42. https://dx.doi.org/10.1016/j.fertnstert.2006.01.042.
- Li K., Nowak R.A. The role of basigin in reproduction. Reproduction. 2019; REP-19-0268.R1. https://dx.doi.org/10.1530/REP-19-0268.
- Долгушин Г.О., Романов А.Ю. Влияние SARS-COV-2 репродукцию человека. Акушерство и гинекология. 2020; 11: 6-12. [Dolgushin G.O., Romanov A.Yu. Effects of SARS-CoV-2 on human reproduction. Obstetrics and Gynecology. 2020; 11: 6-12. (in Russian)]. https://dx.doi.org/10.18565/aig.2020.11.6-12.
- Walls A.C., Park Y.J., Tortorici M.A., Wall A., McGuire A.T., Veesler D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell. 2020; 181(2): 281-92. e6. https://dx.doi.org/10.1016/j.cell.2020.02.058.
- Haghpanah A., Masjedi F., Alborzi S., Hosseinpour A., Dehghani A., Malekmakan L., Roozbeh J. Potential mechanisms of SARS-CoV-2 action on male gonadal function and fertility: Current status and future prospects. Andrologia. 2021; 53(1): e13883. https://dx.doi.org/10.1111/and.13883.
- Holtmann N., Edimiris P., Andree M., Doehmen C., Baston-Buest D., Adams O., Kruessel J.S., Bielfeld A.P. Assessment of SARS-CoV-2 in human semen – a cohort study. Fertil. Steril. 2020; 114(2): 233-8. https://dx.doi.org/10.1016/j.fertnstert.2020.05.028.
- Ma L., Xie W., Li D., Shi L., Ye G., Mao Y. et al. Evaluation of sex-related hormones and semen characteristics in reproductive-aged male COVID-19 patients. J. Med. Virol. 2021; 93(1): 456-62. https://dx.doi.org/10.1002/jmv.26259.
- Xu J., Qi L., Chi X., Yang J., Wei X., Gong E. et al. Orchitis: a complication of severe acute respiratory syndrome (SARS). Biol. Reprod. 2006; 74(2): 410-6. https://dx.doi.org/10.1095/biolreprod.105.044776.
- La Marca A., Busani S., Donno V., Guaraldi G., Ligabue G., Girardis M. Testicular pain as an unusual presentation of COVID-19: a brief review of SARS-CoV-2 and the testis. Reprod. Biomed. Online. 2020; 41(5): 903-6. https://dx.doi.org/10.1016/j.rbmo.2020.07.017.
Received 14.07.2021
Accepted 20.07.2021
About the Authors
Yulia S. Drapkina, Ph.D., Obstetrition-Gynecologist at the B.V. Leonov Department of Assisted Technologies for the Treatment of Infertility, V.I. Kulakov NMRC for OG&P,Ministry of Healthcare of the Russian Federation. E-mail: julia.drapkina@gmail.com. 4 Oparin str., 117997, Moscow, Russia.
Nataliya V. Dolgushina, Dr. Med. Sci., Deputy Director – Head of the Department of Research Administration, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare
of the Russian Federation. Tel.: +7(495)438-49-77. E-mail: n_dolgushina@oparina4.ru 4 Oparin str., 117997, Moscow, Russia.
Taras V. Shatylko, Ph.D., urologist at the Department of Andrology and Urology, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation.
Tel.: +7(927)620-49-25. E-mail: dialectic.law@gmail.com. 4 Oparin str., 117997, Moscow, Russia.
Marina A. Nikolaeva, Dr. Med. Sci., Leading Researcher at the Laboratory of Clinical Immunology, V.I. Kulakov NMRC for OG&P,
Ministry of Healthcare of the Russian Federation. Tel.: +7(495)438-11-83. E-mail: MNikolaeva@oparina4.ru. 4 Oparin str., 117997, Moscow, Russia.
Irina V. Menzhinskaya, Dr. Med. Sci., Senior Researcher at the Laboratory of Clinical Immunology, V.I. Kulakov NMRC for OG&P,
Ministry of Healthcare of the Russian Federation. Tel.: +7(915)345-06-59. E-mail: i_menzinskaya@oparina4.ru. 4 Oparin str., 117997, Moscow, Russia.
Tatiana Yu. Ivanets, Dr. Med. Sci., Head of the Clinical Diagnostic Laboratory, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation.
Tel.: +7(495)438-25-66. E-mail: t_ivanets@oparina4.ru. 4 Oparin str., 117997, Moscow, Russia.
Lyubov V. Krechetova, Dr. Med. Sci., Head of the Laboratory of Clinical Immunology, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation.
Tel.: +7(495)438-11-83. E-mail: k_l_v_@mail.ru. 4 Oparin str., 117997, Moscow, Russia.
Alexey M. Krasnyi, PhD, Head of the Laboratory of Cytology, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation. Tel.: +7(963)750-35-35.
E-mail: a_krasnyi@oparina4.ru. 4 Oparin str., 117997, Moscow, Russia. Safar I. Gamidov, Dr. Med. Sci., Head of Department of Andrology and Urology,
Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation. Tel.: +7(963)750-30-28. E-mail: safargamidov@yandex.ru. 4 Oparin str., 117997, Moscow, Russia.
Gyuldana R. Bayramova, Dr. Med. Sci., Clinical Care Supervisor at the Polyclinic Department, V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation. Tel.: +7(909)994-77-00. E-mail: g_bairamova@oparina4.ru. 4 Oparin str., 117997, Moscow, Russia.
Gennady T. Sukhikh, Dr. Med. Sci., Professor, Academician of the RAS, Director of the V.I. Kulakov NMRC for OG&P, Ministry of Healthcare of the Russian Federation.
Tel.: +7(495)438-18-00. E-mail: secretariat@oparina4.ru. 4 Oparin str., 117997, Moscow, Russia.
For citation: Drapkina Yu.S., Dolgushina N.V., Shatylko T.V., Nikolaeva M.A., Menzhinskaya I.V., Ivanets T.Yu., Krechetova L.V., Krasnyi A.M., Gamidov S.I., Bairamova G.R., Sukhikh G.T. Gam-COVID-Vac (Sputnik V) vaccine has no adverse effect on spermatogenesis in men.
Akusherstvo i Ginekologiya / Obstetrics and gynecology. 2021; 7: 88-94 (in Russian)
https://dx.doi.org/10.18565/aig.2021.7.88-94
Similar Articles

