В процессе внутриутробного развития под влиянием различных экзо- и эндогенных факторов возникает совокупность отклонений, которые называются аномалиями развития. Нарушение эмбриональной закладки может происходить с 3-й по 20-ю неделю беременности.
В норме два протока ответственны за образование женских половых путей, одним из которых является мезонефрический проток (вольфов проток), а другим – парамезонефрический проток (мюллеров проток). Двурогая матка относится к порокам слияния мюллеровых протоков. Эта относительно распространенная аномалия формируется из-за отсутствия сращения дна матки, что приводит к образованию двух полостей, которые связаны одной шейкой матки и влагалищем. Продольная перегородка влагалища не редкость при данной аномалии развития матки (АРМ) [1].
У пациенток с АРМ (встречаемость в общей популяции 4,3–12%) чаще возникают бесплодие (8% среди пациенток с бесплодием), осложнения гестации и родов (13% женщин с самопроизвольным выкидышем в анамнезе, 5–16,7% пациенток с привычным невынашиванием); поэтому своевременные диагностика и коррекция этих отклонений являются актуальной проблемой современной гинекологии [2–4].
Известно, что частота встречаемости двурогой матки составляет 0,4% среди населения в целом, 1,1% – среди женщин с бесплодием и 2,1% – у женщин с выкидышем [5, 6]. Истинную распространенность АРМ рассчитать затруднительно, так как клиническая картина при данных заболеваниях является неспецифичной.
Достоверная причина развития АРМ не ясна. На данный момент известны группы факторов, которые могут приводить к возникновению аномалий: наследственные, экзогенные и мультифакторные.
В некоторых исследованиях была доказана связь между аномальным строением женских половых органов и патологической экспрессией генов Pax, Lim1, Emx2, Wnt4, Wnt9b, которые участвуют в развитии мюллеровых протоков. Ген Wnt7a отвечает за экспрессию генов Hoxa 10 и Hoxa 11. Эта сегментарная экспрессия Hoxa 9, 10, 11 и 13 вдоль мюллерова протока по линейной схеме необходима для дифференциации протоков в фаллопиевы трубы, матку, шейку матки и влагалище [7].
Факторы окружающей среды также могут быть индукторами развития аномалий женских половых органов. Например, в 1940–1970-х гг. развитие Т-образной матки ассоциировалось с применением диэтилстильбэстрола во время беременности. Тем не менее частота этого заболевания снижается, поскольку в настоящее время препарат не используется [8].
Двурогая матка может быть обнаружена и как отдельная патология, в сочетании с другими вариантами пороков развития. Изолированная двурогая матка ассоциирована со значительными репродуктивными осложнениями. В метаанализе 25 сравнительных исследований сообщалось о значительном повышении риска потери беременности в I и II триместрах, преждевременных родов, рождения ребенка с низким показателем веса, тазового или поперечного положения плода [2].
У большинства пациенток с двурогой маткой в подростковом возрасте нет никаких симптомов. Некоторые женщины могут обратиться в клинику с меноррагией или дисменореей из-за наличия двух полостей матки. Некоторым ставят диагноз, когда они приходят на плановое обследование во время беременности. Значительному числу женщин ставится диагноз, когда у них возникают акушерские осложнения.
При ультразвуковой диагностике двурогой матки в сагиттальной проекции визуализируются две полости при отражении от цервикального канала, во фронтальной проекции перемещение датчика от шейки матки к дну позволяет определить симметрично расходящиеся одинаковой толщины срединные М-эхо [4, 9].
Чаще всего АРМ являются случайной находкой в ходе диагностического поиска. Несмотря на очевидный прогресс в диагностике и лечении гинекологических патологий, АРМ остаются одной из актуальных проблем. У 24–34% больных с АРМ диагноз не ясен или некорректно сформулирован, что влияет на эффективность лечения и реализацию репродуктивной функции пациенток [10]. В современной литературе чаще всего описано течение гестационного периода при АРМ, однако информация о родах у таких пациенток практически не представлена.
Клиническое наблюдение
Пациентка Р., 34 года, госпитализирована в акушерское физиологическое отделение Перинатального центра ГБУЗ Республики Крым «Республиканская клиническая больница им. Н.А. Семашко» с жалобами на развитие регулярной родовой деятельности.
Врожденная аномалия развития внутренних половых органов у пациентки была выявлена в возрасте 21 года, в ходе ультразвукового исследования органов малого таза вне беременности. Отмечались следующие эхографические признаки: увеличение поперечного размера матки и раздвоение М-эхо за счет наличия равноценно развитых маточных рогов, полости которых (на уровне внутреннего зева) сообщаются с цервикальным каналом неудвоенной шейки матки. Консилиумом врачей был выставлен диагноз: Двурогая матка, полная форма, тип 6А (по Makiyan Z., 2021 [11], Q51.3 (по МКБ-10)).
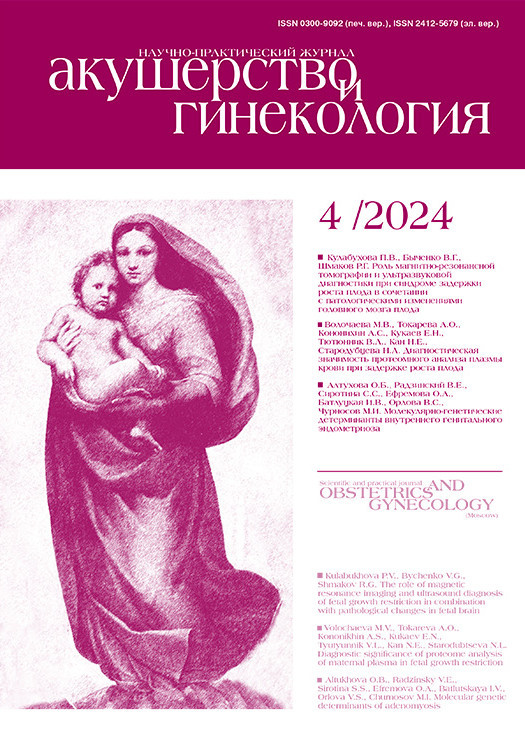
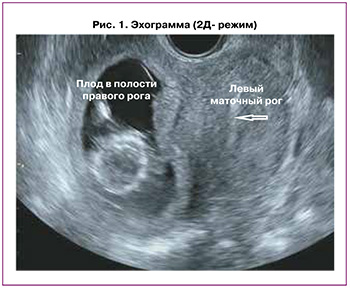
Данная беременность третья. Первая беременность (2012 г.) завершилась операцией кесарева сечения в сроке 37 недель в связи с отслойкой нормально расположенной плаценты. Вторая беременность (2016 г.) – самопроизвольный аборт в сроке 4 недели. Третья беременность (2018 г.) завершилась оперативным лечением внематочной беременности в сроке 3 недели в объеме: лапаротомия, тубэктомия слева. Четвертая беременность настоящая, не индуцированная. В 12 недель взята на учет по беременности в женскую консультацию. Проведено клинико-лабораторное обследование согласно действующему приказу № 1130н Министерства здравоохранения Российской Федерации от 20 октября 2020 г. на этапе женской консультации в полном объеме. Перинатальные скрининги проведены в регламентируемые сроки. По данным 1-го ультразвукового скрининга (в 12 недель 5 дней гестации): в полости правого маточного рога определялся 1 живой плод без пороков развития; полость левого рога умеренно расширена (до 16 мм), заполнена гипоэхогенным содержимым; толщина миометрия в области рубца (кесарево сечение) составляла до 4,0 мм; расположенная по задней стенке плацента достигала области внутреннего зева (эхограммы в двухмерном режиме и трехмерной реконструкции представлены на рисунках 1 и 2).
На момент поступления при влагалищном исследовании: влагалище нерожавшей, шейка матки сглажена, открытие маточного зева 2 см, плодный пузырь цел, предлежит головка плода, прижата к I плоскости малого таза. Во влагалище определяется продольная перегородка влагалища толщиной 1 см. Выделения умеренные, слизистые. Установлен предварительный диагноз: Роды II срочные в 40 недель, I период родов. Рубец на матке после операции кесарева сечения в 2012 г. Двурогая матка. По настоятельному желанию пациентки была выбрана предварительная тактика родоразрешения: роды вести через естественные родовые пути под кардиотокографическим мониторингом и контролем гемодинамических показателей. Пациентка была обследована в акушерском физиологическом отделении, результаты клинико-лабораторного обследования в пределах физиологической нормы.
Первый период родов протекал без особенностей, согласно выработанной тактике. Применялась одна доза эпидуральной аналгезии. В 17 ч 20 мин. схватки приобрели потужной характер. Осмотрена врачом. При влагалищном исследовании определялось полное раскрытие шейки матки. Головка плода в плоскости входа в малый таз. Перегородка во влагалище, толщиной 1 см, идущая от переднего к заднему своду. Было принято решение о выполнении операции рассечения перегородки влагалища.
Второй период родов осложнился развитием интранатального дистресса плода: на фоне активной потужной деятельности отмечалась стойкая брадикардия плода со снижением базального ритма до 80–70 ударов в минуту. Вне потуги и при перемене положения тела базальный ритм не восстанавливался. Учитывая интранатальный дистресс плода и наличие условий для экстренного родоразрешения через естественные родовые пути было решено родоразрешить пациентку путем операции вакуум-экстракции плода в экстренном порядке.
В 17 ч 53 мин. в родильном зале за головку извлечен живой доношенный мальчик весом 3030 г, ростом 50 см. Состояние ребенка по шкале Апгар на 1-й минуте – 8 баллов, на 5-й минуте – 9 баллов.
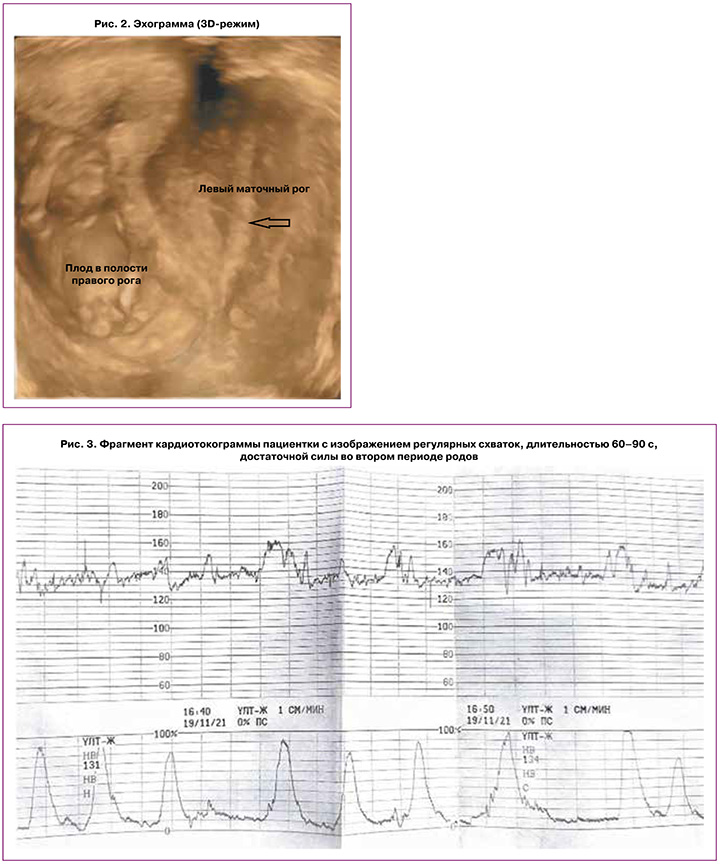
Обращают на себя внимание данные кардиотокографического исследования: сократительная активность матки на протяжении всего периода родов представляла собой регулярные схватки длительностью от 30 с в первом периоде родов до 1,5 минуты в потужном периоде, достаточной силы (рис. 3).
Обсуждение
Распространенность и клиническое значение врожденных аномалий матки среди населения в целом остаются в значительной степени неизвестными. АРМ чаще всего являются случайной находкой в ходе обследования женщины. Это связано с тем, что клиническая картина при данных патологиях крайне неспецифична. У большинства пациенток нет никаких симптомов. Некоторые женщины могут обратиться в клинику с меноррагией или дисменореей из-за наличия двух полостей матки. Некоторым ставят диагноз, когда они приходят на плановое обследование во время беременности. Значительному числу женщин ставится диагноз, когда у них возникают акушерские осложнения. Также женщины могут узнать об АРМ в ходе диагностического поиска причины акушерских осложнений, имея в анамнезе роды в срок доношенным ребенком. Физикальный осмотр при изолированных аномалиях обычно неинформативен.
Данных о репродуктивных исходах при АРМ крайне мало. Важно отметить, что в современной литературе не представлены проспективные рандомизированные контролируемые исследования, в которых бы сравнивались варианты метропластики на этапе прегравидарной подготовки и ведения беременности без оперативного вмешательства. В связи с этим каждый описанный клинический случай родов при АРМ представляет интерес и вклад в изучение проблемы.
Заключение
Роды при АРМ матки возможны через естественные родовые пути. Данная патология требует дальнейшего изучения, обобщения и систематизации данных с целью разработки диагностических алгоритмов и лечебных подходов для применения в рутинной практике врачей-клиницистов.