
Possibilities for the risk prediction of severe locomotive syndrome in 50–60-year-old women with climacteric syndrome
Dobrokhotova Yu.E., Khashukoeva A.Z., Naumov A.V., Nosova L.A., Proskuryakova A.S., Kuznetsov D.A.
Rationale: Ageing of population makes maintaining mobility in postmenopausal women a public health priority. Locomotive syndrome (LS) is known to be an integrated indicator of locomotor system disorders, which is found in 88% of women during this period. Existing tools (FRAX, SARC-F) assess bone or muscle tissue separately, disregarding the pathogenetic link between menopause and locomotor disorders.
Objective: To develop a prognostic model for the risk assessment of severe mobility impairments in musculoskeletal diseases in women with climacteric syndrome (CS).
Materials and methods: The study included 180 patients with CS aged 50–60. We conducted CS and LS severity assessment along with a comprehensive examination: GLFS-25, REMS densitometry, and bioimpedance analysis. A classification tree method was used to construct the model, ensuring the interpretability of risk classes. To assess the quality, we used ROC analysis (AUC, sensitivity, specificity).
Results: Stage III LS was detected in 24.4% of women. We identified six risk classes with the risk for severe mobility impairments development ranging from 3.5 to 66.7%. The extremely high-risk group (66.7%) is associated with a combination of moderate CS severity, postmenopausal duration ≥5 years, and a decrease in the REMS T-score < -1.5. Unlike FRAX, which assesses fracture risk, the model predicts the risk of functional loss (stage III LS) (AUC=0.82), which clinical significance appears earlier than that of a fracture.
Conclusion: For the first time, a model has been developed that combines the severity of cesarean section, clinical and history data, and musculoskeletal parameters to predict the risk of locomotor autonomy loss. The model allows gynecologists to perform screening in an outpatient setting.
Authors’ contributions: Dobrokhotova Yu.E., Khashukoeva A.Z., Naumov A.V., Nosova L.A. – study concept and design; Nosova L.A., Proskuryakova A.S., Kuznetsov A.D. – material collection and processing, data statistical processing; Khashukoeva A.Z., Nosova L.A. – manuscript conduction; Dobrokhotova Yu.E., Khashukoeva A.Z., Naumov A.V. – manuscript editing.
Conflicts of interest: The authors declare no possible conflict of interests.
Funding: The study had no financial support.
Ethical Approval: The study was approved by the independent Ethics Committee of the Pirogov Russian National Research Medical University, Ministry of Health of Russia (Protocol No. 213 of December 13, 2021).
Patient Consent for Publication: The patients signed informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Dobrokhotova Yu.E., Khashukoeva A.Z., Naumov A.V., Nosova L.A., Proskuryakova A.S., Kuznetsov D.A. Possibilities for the risk prediction of severe locomotive syndrome in 50–60-year-old women with climacteric syndrome.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (4): 134-142 (in Russian)
https://dx.doi.org/10.18565/aig.2026.117
Keywords
climacteric syndrome
menopause
locomotive syndrome
osteoporosis
osteoarthritis
sarcopenia
Over 21 million women in Russia suffer from peri- and postmenopause, spending more than one-third of their lives in progressive estrogen deficiency [1–3]. Due to increasing life expectancy, maintaining quality of life and physical activity in women during this period has become a priority medical and social task [3].
Menopause is associated with an increased risk of musculoskeletal disorders (osteoarthritis, osteoporosis, sarcopenia) [4–9]. However, such connection is often underestimated by both patients and physicians. While visiting a gynecologist, women often focus on vasomotor and psychoemotional symptoms, neglecting diffuse muscle and joint pain, decreased mobility, and difficulty walking [10].
In recent years, the term “locomotive syndrome” (LS) has been introduced to assess the functional status of the locomotor system, which refers to a mobility disorder caused by diseases of the musculoskeletal system [11–13].
The extremely high prevalence of LS in postmenopausal women (up to 88.4%) indicates an urgent need to study this condition with reference to hormonal changes [14, 15].
LS, which is known as an integral indicator of locomotor system disorders, is found in 88% of women during the postmenopausal period. Existing tools (FRAX, SARC-F) assess bone or muscle tissue separately, without taking into account the pathogenetic link between menopause and locomotor disorders.
At the same time, a gynecologist has a unique opportunity for early risk detection, prevention and interdisciplinary management of patients with mobility impairments.
Materials and methods
The open-label, cross-sectional (one-stage) study enrolled 180 postmenopausal women.
Inclusion criteria: 50–60-year-old women with climacteric syndrome, 1 to 10 years postmenopause duration, and presence of musculoskeletal diseases.
Non-inclusion criteria: Cerebrovascular disorders (including a history of stroke), neurodegenerative pathologies, hematological disorders, rheumatic diseases, connective tissue dysplasia, and chronic renal failure. History of oncological pathology or its discovery during the study was also regarded as the non-inclusion criterion. The same was true for the use of menopausal hormone therapy and antiresorptive therapy. Intake of vitamin D and calcium supplementation during the study, gastrointestinal diseases requiring parenteral nutrition, malabsorption syndrome, gastrointestinal ulcers, inflammatory bowel disease, unexplained weight loss, and fever also were the reasons for non-inclusion of such patients into the study.
All patients underwent a general clinical examination, including a medical history taking, physical and gynecological screening, Pap smear, mammography, pelvic and breast ultrasound, lipid profile, and complete blood count. To assess the severity of menopausal syndrome we used the Greene Climacteric Scale. The severity of the locomotive syndrome was identified based on the most unfavorable result of three tests: the chair rise test, the two-step test, and the Lokomo-25 questionnaire. Muscle mass was assessed using bioimpedance analysis. To assess muscle strength, we used wrist dynamometry and the five times sit-to-stand test. Bone mineral density of the lumbar spine and proximal femoral neck was measured using radiofrequency echographic multispectrometry (REMS). Based on the sum of points of the scale, which assesses the severity of climacteric disorders, all patients were divided into three groups: Group 1 included 58/180 (32.2%) mild degree (1-11 points) women, Group 2 enrolled 66/180 (36.7%) patients with moderate degree (12-19 points) climacteric symptoms, Group 3 comprised 56/180 (31.1%) severe degree (20 points or more) women.
The study was approved by the independent ethics committee of the Pirogov Russian National Research Medical University of the Ministry of Health of Russia (Ethics Committee Protocol No. 213 of December 13, 2021). The study was carried out in compliance with ethical norms and standards.
Statistical analysis
Statistical processing of the collected data was carried out in the SAS JMP 11 and Statistica 10 software packages. The significance level was less than 0.05. Numerical variables were described by the arithmetic mean (M) and standard deviation (SD) in the M±SD format.
The type of measurement scale and the number of groups compared determined the statistical method. We used the Kruskal-Wallis test to analyze data from three or more groups, the nonparametric Mann-Whitney test – to compare numerical indicators between two groups. Also we assessed differences in binary and nominal variables using the Pearson chi-square test. Relationships between variables were analyzed with the nonparametric Spearman rank correlation.
To model target indicators, we used the classification tree method, which predicts event probabilities based on independent factor values and classifies subjects into risk categories. This tool sequentially analyzes the influence of individual variables and performs univariate branching while assessing the contribution of each factor. ROC analysis allowed us to evaluate the quality of the resulting models.
Results
The average age of patients in the 1st group was 55.91 (3.47) years, while in the 2nd group it was 57.35 (2.85) years, and in the 3rd – 55.46 (2.8) years (p<0.05). The characteristics of the groups are presented in Tables 1 and 2.
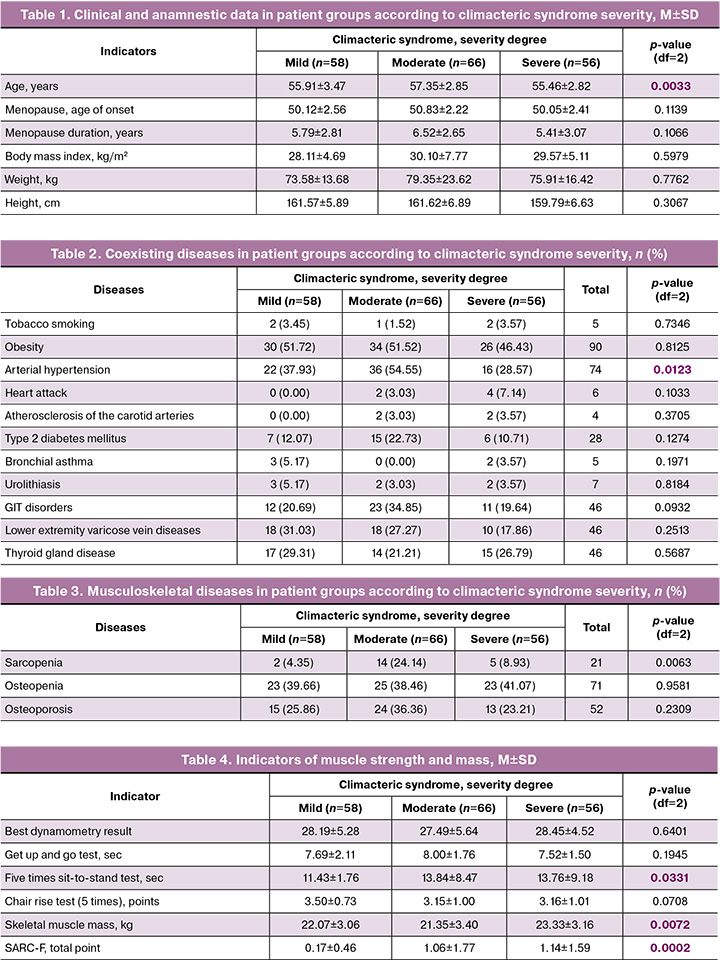
A statistically significant difference was found for the “arterial hypertension” in the 2nd group compared to the 3rd patient group (by 26.0%; p=0.0123).
When assessing musculoskeletal diseases in the overall cohort, osteoarthritis turned out to be the most common (72.8%) disease, compared to osteopenia (39.4%) and osteoporosis (28.9%). Sarcopenia was diagnosed in 11.6% of women patients. The structure of musculoskeletal diseases in the groups is presented in Table 3.
Sarcopenia was statistically significantly more often diagnosed in women with moderate climacteric syndrome than in women with mild climacteric symptoms (by 19.8%; p=0.0063).
The indicators of muscle strength (dynamometry) and mass (bioimpedancemetry) are presented in Table 4.
When analyzing the results of hand dynamometry, no statistically significant differences were found in the groups (p=0.64). The most prominent differences were detected for the “five times sit-to-stand test” in the group with moderate climacteric syndrome in comparison to the 1st patient group (on average by 2.4 sec; p=0.0331). The skeletal muscle mass was statistically significantly lower in the 2nd group when comparing to group 3 (on average by 2.0 kg; p=0.0072). A statistically significant difference was found for the indicator “SARC-F, total score” in the 3rd group comparing to group 1 (on average by 1.0 point; p=0.0002).
The structure of LS detection in groups is presented in Figure 1.
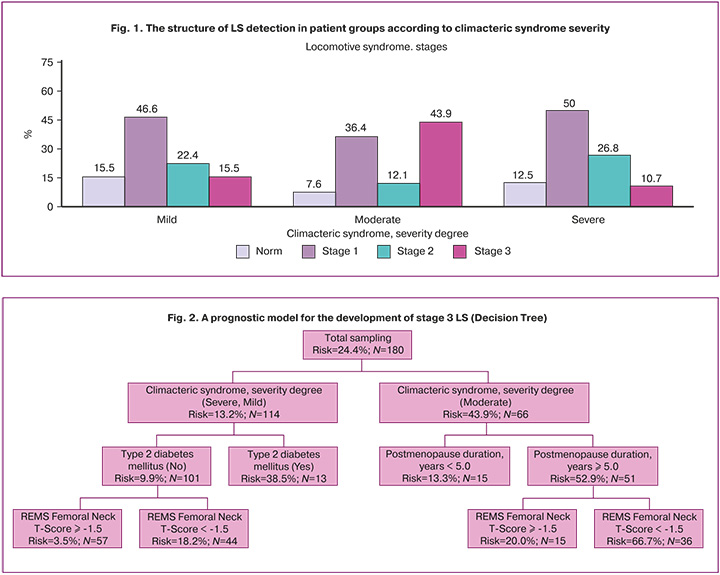
A statistically significant difference was found for stage 3 LS in the group of women with moderate climacteric syndrome while comparing to the patient group with severe climacteric syndrome (by 33.2%; p<0.0001) (Table 5).

According to the REMS data, the lowest femoral neck T-score values were observed in the group of patients with severe climacteric syndrome, as well as in women with moderate climacteric syndrome (on average, by 0.7; p=0.0078). It was found that women with moderate climacteric syndrome were significantly more often diagnosed with severe climacteric syndrome (stage 3) compared to the patients with mild and severe climacteric syndrome (p1-2=0.0057, p2-3=0.0006).
Figure 2 shows a prognostic model for the development of stage 3 LS, which is a “Decision Tree” diagram for assessing the risk of severe stage LS development based on a combination of four influencing factors: “Climacteric syndrome, severity degree”, “Postmenopause duration”, “Type 2 diabetes mellitus” and “REMS Femoral Neck T-Score”.
We identified six risk groups using the "Decision Tree" (Table 6), of which the highest probability of progression to stage 3 LS (66.7% of 36 patients in the group) is demonstrated by patients with a postmenopausal period of 5 years, a REMS Femoral Neck T-Score ≤ -1.5, and moderate climacteric syndrome. The minimum risk (3.5% with a group size of 57 people) for stage 3 LS development is typical for patients with the following combination of factors: severe and mild climacteric syndrome, type 2 diabetes mellitus (No), and REMS Femoral Neck T-Score ≥ -1.5.
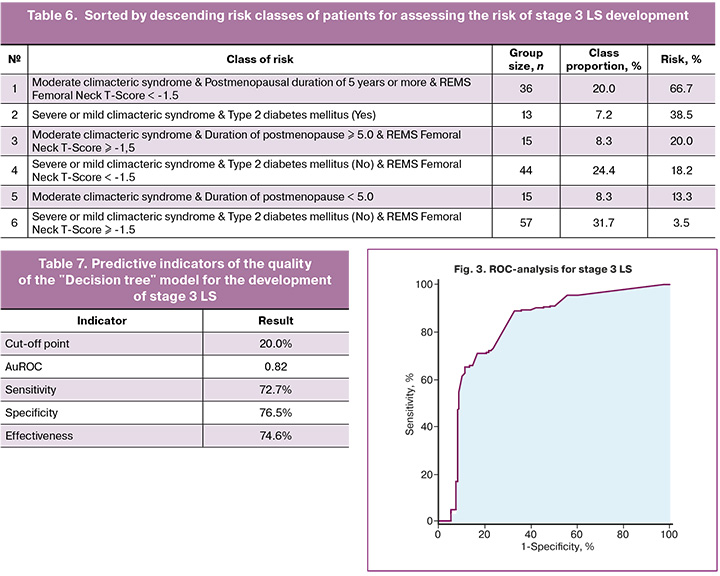
The results of the ROC analysis and the predictive pattern of the Decision Tree model are presented in Table 7 and Figure 3.
The simulated Decision Tree has a moderate predictive pattern with an AuROC value of 0.82, where a prediction is considered to be positive for a risk assessment of 20.0% or higher, and negative for lower values. A negative result is correctly identified in 76.5% of cases, while a positive result can be detected in 72.7%.
Stage 3 LS was diagnosed in 24.4% of women patients. We identified six risk classes using the "Decision Tree" method, with the risk of severe disorders development ranging from 3.5 to 66.7%. The extremely high-risk group (66.7%) is associated with a combination of moderate climacteric syndrome, a postmenopausal duration of ≥5 years, and a decrease in the REMS T-score to <-1.5. The predictive quality of the model is high. Its reliability was confirmed by the bootstrap procedure (1000 replicates), demonstrating the stability of the coefficients (p=0.001) and the absence of significant bias.
Unlike FRAX, which assesses the risk of fractures, the model predicts the risk of functional loss, i.e. the risk of a severe LS development (AUC=0.82), which is clinically and significantly more important than a fracture.
Discussion
Among the constantly growing adult population aged over 50, postmenopausal women are at particular risk for locomotor system disorders. A
Age-associated changes in these women are exacerbated by severe estrogen deficiency, which can accelerate the development and progression of osteoarthritis, osteoporosis, and other pathologies [16–18]. Diseases of the musculoskeletal system and the presence of climacteric syndrome significantly undermine the health of postmenopausal women, resulting in the reduction of the quality of life and shortening of its active period [19]. Low-energy fractures turn out to be the greatest threat among other complications: in elderly people they often lead to disability, while within a year after injury mortality rate remains high [20–22]. Over the past three decades, locomotor system diseases have remained the leading cause of disability among adults aged over 50 [16].
Depending on the fracture site and gender, overall survival varies significantly from 67.7% to 95.3% in 1 year and from 32.3% to 78.6% in 5 years of follow-up among patients with low-energy fractures aged ≥66 [23].
Thus, the ability to move independently and care for oneself gradually declines and eventually is completely lost, and the person then requires constant assistance from others. Osteoporosis affects 19.7% of the world's population. The disease is diagnosed in 27% of men and 34% of women over 50 years in Russia. One in eight men and one in four women of this age group have already suffered a pathological fracture [24–26]. Treatment and rehabilitation of such patients is difficult, so it is a serious medical and social problem.
LS was diagnosed in 88.3% of women, which is comparable to the data obtained by Topolyanskaya S.V. et al. (up to 88.4% in postmenopausal women) [12]. It is important that stage 3 LS, associated with a high risk of loss of self-care, was detected in 24.4% of patients. This is significantly higher than in the young population – 20% [27], which emphasizes the role of menopausal changes in the LS progression.
In the context of the progressive aging of the world's population, the creation of new interdisciplinary scientific fields aimed at limiting the long-term consequences of locomotor system diseases is becoming extremely essential.
The predictive model we developed (Decision Tree) allowed us to identify six risk classes with a sensitivity of 72.7% and a specificity of 76.5% (AUC=0.82). The most significant factors were moderate menopausal syndrome, postmenopausal duration of ≥5 years, and a decrease in the REMS T-score to <-1.5 SD.
From a practical perspective, the resulted prognostic model, which includes easily assessed parameters, makes it possible to identify high-risk groups for mobility impairment at the outpatient stage and to initiate preventive measures timely. This justifies the need for early screening and a multidisciplinary approach involving gynecologists.
Study limitations. When interpreting the results, several limitations should be taken into account. Firstly, the cross-sectional design does not allow for establishing causal relationships. Secondly, the relatively small patient group size (n=180) and a single center study base limit the generalization of the results. Finally, the REMS method we used, although validated, is not the “gold standard” for densitometry (like DXA). However, its non-ionizing nature and portability make it convenient for screening.
Conclusion
During the study, for the first time we elaborated a model that combines the severity of climacteric syndrome, clinical and anamnestic data and parameters of the musculoskeletal system to predict the risk of autonomy loss.
Despite its limitations, this study is the first to demonstrate a strong link between the severity of menopausal syndrome and mobility impairments assessed using the LS concept. These findings support the need to incorporate LS screening into the standard examination of postmenopausal women and to develop interdisciplinary approaches for the management of such patients. Prospective studies to improve the model's prognostic value and to study the impact of menopausal therapy on LS dynamics are promising areas of research.
This model makes it possible for gynecologists to perform screening in an outpatient setting.
References
- Schoenaker D.A., Jackson C.A., Rowlands J.V., Mishra G.D. Socioeconomic position, lifestyle factors and age at natural menopause: a systematic review and meta-analyses of studies across six continents. Int. J. Epidemiol. 2014; 43(5): 1542-62. https://dx.doi.org/10.1093/ije/dyu094
- Sun X., Zhang R, Wang L., Shen X, Lu X., An J. et al. Association between parity and the age at menopause and menopausal syndrome in Northwest China. Asia Pacific Journal of Public Health. 2021; 33(1): 60-6. https://dx.doi.org/10.1177/1010539520960987
- Министерство здравоохранения Российской Федерации. Клинические рекомендации. Менопауза и климактерическое состояние у женщины. 2025. [Ministry of Health of the Russian Federation. Clinical guidelines. Menopause and climacteric state in women. 2025 (in Russian)].
- Tulloh L. Restoring trust in menopause management: menopause hormone therapy is not a panacea, and physical activity remains a critical intervention. Br. J. Sports Med. 2025; 59(12): 828-9. https://dx.doi.org/10.1136/bjsports-2025-110217
- Сулима А.Н., Булюк В.В., Митрофанова О.А. Постменопаузальный остеопороз. Акушерство и гинекология. 2023; 9: 52-9. [Sulima A.N., Bulyuk V.V., Mitrofanova O.A. Postmenopausal osteoporosis. Obstetrics and Gynecology. 2023; (9): 52-9 (in Russian)]. https://dx.doi.org/10.18565/aig.2023.103
- Mishra G.D., Dobson A.J. Using longitudinal profiles to characterize women’s symptoms through midlife: results from a large prospective study. Menopause. 2012; 19(5): 549-55. https://dx.doi.org/10.1097/gme.0b013e3182358d7c
- Jin Z., Tian C., Kang M., Hu S., Zhao L., Zhang W. The 100 top-cited articles in menopausal syndrome: a bibliometric analysis. Reproductive Health. 2024; 21(1): 47. https://dx.doi.org/10.1186/s12978-024-01770-9
- Di Martino A., Barile F., D'Agostino C., Castafaro V., Cerasoli T., Mora P. et al. Are there gender-specific differences in hip and knee cartilage composition and degeneration? A systematic literature review. Eur. J. Orthop. Surg. Traumatol. 2024; 34(4): 1901-10. https://dx.doi.org/10.1007/s00590-024-03871-4
- Носова Л.А., Хашукоева А.З., Наумов А.В., Соловьева А.М., Смагина Ю.А. Тяжесть климактерического синдрома и нарушений мобильности при заболеваниях костно-мышечной системы у женщин с разными типами менопаузы. Акушерство и гинекология. 2025; 3: 92-100. [Nosova L.A., Khashukoeva A.Z., Naumov A.V., Soloveva A.M., Smagina Yu.A. The severity of the climacteric syndrome and mobility impairments in women with musculoskeletal disorders and different types of menopause. Obstetrics and Gynecology. 2025; (3): 92-100 (in Russian)]. https://dx.doi.org/10.18565/aig.2025.50
- Harlow S.D., Gass M., Hall J.E., Lobo R., Maki P., Rebar R.W. et al. Executive summary of the Stages of reproductive aging workshop + 10: addressing the unfinished agenda of staging reproductive aging. Menopause. 2012; 19(4): 387-95. https://dx.doi.org/10.1097/gme.0b013e31824d8f40
- Nakamura K. A "super-aged" society and the "locomotive syndrome". J. Orthop. Sci. 2008; 13(1): 1-2. https://dx.doi.org/10.1007/s00776-007-1202-6
- Shibata S., Kon S. Functional ingredients associated with the prevention and suppression of locomotive syndrome: a review. Biol. Pharm. Bull. 2024; 47(12): 1978-91. https://dx.doi.org/10.1248/bpb.b24-00443
- Наумов А.В., Ховасова Н.О., Мороз В.И., Мешков А.Д., Маневич Т.М., Деменок Д.В. Локомотивный синдром: новое представление о хрупкости в пожилом возрасте. Российский журнал гериатрической медицины. 2021; 3: 372-8. [Naumov A.V., Khovasova N.O., Moroz V.I., Meshkov A.D., Manevich T.M., Demenok D.V. Locomotive syndrome: a new view of fragility in older age. Russian Journal of Geriatric Medicine. 2021; 3: 372-8 (in Russian)]. https://dx.doi.org/10.37586/2686-8636-3-2021-364-370
- Тополянская С.В., Романова М.А., Вакуленко О.Н., Бубман Л.И., Елисеева Т.А., Ларина Д.С., Рачина С.А., Дворецкий Л.И. «Локомотивный синдром» в практике гериатрического стационара. Медицинский алфавит. 2023; (13): 36-41. [Topolyanskaya S.V., Romanova M.A., Vakulenko O.N., Bubman L.I., Eliseeva T.A., Larina D.S., Ratchina S.A., Dvoretski L.I. «Locomotive syndrome» in patients in the geriatric hospital. Medical alphabet. 2023; (13): 36-41 (in Russian)]. https://dx.doi.org/10.33667/10.33667/2078-5631-2023-13-36-41
- Ikemoto T., Arai Y.C. Locomotive syndrome: clinical perspectives. Clin. Interv. Aging. 2018; 13: 819-27. https://dx.doi.org/10.2147/CIA.S148683
- Guan S.Y., Zheng J.X., Zhang S.X., Xu S., Shuai Z., Cai H.Y. et al. Global burden of musculoskeletal disorders in adults aged 50 and over, 1990-2021: risk factors and sociodemographic inequalities. J. Cachexia Sarcopenia Muscle. 2025; 16(4): e70008. https://dx.doi.org/10.1002/jcsm.70008
- Lobo R.A., Gompel A. Management of menopause: a view towards prevention. Lancet Diabetes Endocrinol. 2022; 10(6): 457-70. https://dx.doi.org/10.1016/S2213-8587(21)00269-2
- Gulati M., Dursun E., Vincent K., Watt F.E. The influence of sex hormones on musculoskeletal pain and osteoarthritis. Lancet Rheumatol. 2023; 5(4): e225-38. https://dx.doi.org/10.1016/S2665-9913(23)00060-7
- Балан В.Е., Тихомирова Е.В., Журавель А.С., Титченко Ю.П., Ловыгина Т.В. Новые тенденции в современной менопаузальной гормональной терапии. Гинекология. 2021; 23(1): 33-6. [Balan V.E., Tikhomirova E.V., Zhuravel A.S., Titchenko Yu.P., Lovygin T.V. New trends in current menopausal hormone therapy. Gynecology. 2021; 23(1): 33-6 (in Russian)]. https://dx.doi.org/10.26442/20795696.2021.1.200635
- Исмаилов С.И., Ходжамбердиева Д.Ш., Рихсиева Н.Т. Остеопороз и низкоэнергетические переломы шейки бедра как осложнение различных эндокринных заболеваний (обзор литературы). Международный эндокринологический журнал. 2013; 5(53): 113-20. [Ismailov S.I., Khodjamberdiyeva D.Sh., Rikhsiyeva N.T. Osteoporosis and low-energy hip fractures as complication of various endocrine diseases (literature review). International journal of endocrinology. 2013; 5(53): 113-20 (in Russian)].
- Лобанова К.Г., Ушанова Ф.О. Диагностика и лечение остеопороза: смена парадигмы. FOCUS Эндокринология. 2024; 5(1): 65-73. [Lobanova K.G., Ushanova F.O. Diagnosis and treatment of osteoporosis: a paradigm shift. FOCUS Endocrinology. 2024; 5(1): 65-73 (in Russian)]. https://dx.doi.org/10.62751/2713-0177-2024-5-1-09
- Walter N., Szymski D., Kurtz S., Alt V., Lowenberg D.W., Lau E. et al. Factors associated with mortality after proximal femoral fracture. J. Orthop. Traumatol. 2023; 24(1): 31. https://dx.doi.org/10.1186/s10195-023-00715-5
- Vincent G., Adachi J.D., Schemitsch E., Tarride J.E., Ho N., Wani R.J. et al. Postfracture survival in a population-based study of adults aged ≥ 66 years: a call to action at hospital discharge. JBMR Plus. 2024; 8(5): ziae002. https://dx.doi.org/10.1093/jbmrpl/ziae002
- Xiao P.L., Cui A.Y., Hsu C.J., Peng R., Jiang N., Xu X.H. et al. Global, regional prevalence, and risk factors of osteoporosis according to the World Health Organization diagnostic criteria: a systematic review and meta-analysis. Osteoporos Int. 2022; 33(10): 2137-53. https://dx.doi.org/10.1007/s00198-022-06454-3
- Белая Ж.Е., Белова К.Ю., Бирюкова Е.В., Дедов И.И., Дзеранова Л.К., Драпкина О.М., Древаль А.В., Дубовицкая Т.А., Дудинская Е.Н., Ершова О.Б., Загородний Н.В., Илюхина О.Б., Канис Д.А., Крюкова И.В., Лесняк О.М., Мамедова Е.О., Марченкова Л.А., Мельниченко Г.А., Никанкина Л.В., Никитинская О.А., Петряйкин А.В., Пигарова Е.А., Родионова С.С., Рожинская Л.Я., Скрипникова И.А., Тарбаева Н.В., Ткачева О.Н., Торопцова Н.В., Фарба Л.Я., Цориев Т.Т., Чернова Т.О., Юренева С.В., Якушевская О.В. Федеральные клинические рекомендации по диагностике, лечению и профилактике остеопороза. Остеопороз и остеопатии. 2021; 24(2): 4-47. [Belaya Zh.E., Belova K.Yu., Biryukova E.V., Dedov I.I., Dzeranova L.K., Drapkina O.M., Dreval A.V., Dubovitskaya T.A., Dudinskaya E.N., Ershova O.B., Zagorodniy N.V., Ilyukhina O.B., Kanis J.A., Kryukova I.V., Lesnyak O.M., Mamedova E.O., Marchenkova L.A., Mel’nichenko G.A., Nikankina L.V., Nikitinskaya O.A., Petryaikin A.V., Pigarova E.A., Rodionova S.S., Rozhinskaya L.Ya., Skripnikova I.A., Tarbaeva N.V., Tkacheva O.N., Toroptsova N.V., Farba L.Ya., Tsoriev T.T., Chernova T.O., Yureneva S.V., Yakushevskaya O.V. Federal clinical guidelines for diagnosis, treatment and prevention of osteoporosis. Osteoporosis and Bone Diseases. 2021; 24(2): 4-47 (in Russian)]. https://dx.doi.org/10.14341/osteo12930
- Ершова О.Б., Белова К.Ю., Белов М.В., Ганерт О.А., Романова М.А., Синицына О.С., Гладкова Е.Н., Ходырев В.Н., Лесняк О.М., Пилюкова Р.И., Давтян В.Г. Эпидемиология переломов проксимального отдела бедренной кости у городского населения Российской Федерации: результаты многоцентрового исследования. Боль. Суставы. Позвоночник. 2012; 3: 88-90. [Ershova O.B., Belova K.Yu., Belov M.V., Ganert O.A., Romanova M.A., Sinitsyna O.S., Gladkova E.N., Khodyrev V.N., Lesnyak O.M., Pilyukova R.I., Davtyan V.G. The epidemiology of fractures of the proximal femur in the urban population of the Russian Federation: the results of a multicenter study. Bol’. Sustavy. Pozvonochnik. 2012; 3: 88-90. (in Russian)].
- Sawaya Y., Hirose T., Onuma S., Nakajima R., Fujita S., Muroi S. et al. Prevalence and associated factors of locomotive syndrome in young Japanese adults: a cross-sectional study. BMC Musculoskelet. Disord. 2024; 25(1): 366. https://dx.doi.org/10.1186/s12891-024-07493-z
Received 08.04.2026
Accepted 23.04.2026
About the Authors
Yulia E. Dobrokhotova, Dr. Med. Sci., Professor, Head of the Department of Obstetrics and Gynecology, Institute of Surgery, Pirogov Russian National Research Medical University, Ministry of Health of Russia, 117997, Russia, Moscow, Ostrovityanova str., 1, pr.dobrohotova@mail.ru, https://orcid.org/0000-0002-7830-2290Asiyat Z. Khashukoeva, Dr. Med. Sci., Professor, Professor at the Department of Obstetrics and Gynecology, Institute of Surgery, Pirogov Russian National Research Medical University, Ministry of Health of Russia, 117997, Russia, Moscow, Ostrovityanova str., 1; obstetrician-gynecologist, Russian Gerontological Research and Clinical Center, 129226, Russia, Moscow, 1st Leonova str., 16, azk05@mail.ru, https://orcid.org/0000-0001-7591-6281
Anton V. Naumov, Dr. Med. Sci., Professor at the Department of Diseases of Aging, Faculty of Additional Professional Education, Pirogov Russian National Research Medical University, Ministry of Health of Russia, 117997, Russia, Moscow, Ostrovityanova str., 1; Head of the Laboratory of Diseases of the Musculoskeletal System, Russian Gerontological Research and Clinical Center, 129226, Russia, Moscow, 1st Leonova str., 16, nanton@mail.ru, https://orcid.org/0000-0002-6253-621X
Lilia A. Nosova, Teaching Assistant at the Department of Obstetrics and Gynecology, Institute of Surgery, Pirogov Russian National Research Medical University,
Ministry of Health of Russia, 117997, Moscow, Ostrovityanova str., 1, karelina_lilia@mail.ru, https://orcid.org/0000-0002-0925-3755
Arina S. Proskuryakova, Student, Medical Faculty, Pirogov Russian National Research Medical University, Ministry of Health of Russia, 117997, Moscow, Ostrovityanova str., 1, 2368618al@mail.ru, https://orcid.org/0009-0004-6128-8420
Dmitriy A. Kuznetsov, Resident at the Department of Obstetrics and Gynecology, Institute of Surgery, Pirogov Russian National Research Medical University,
Ministry of Health of Russia, 117997, Moscow, Ostrovityanova str., 1, kda7117@yandex.ru, https://orcid.org/0009-0003-9230-1109
Corresponding author: Asiyat Z. Khashukoeva, azk05@mail.ru
Similar Articles

