
vNOTES hysterectomy
Musin I.I., Berg E.A., Yashchuk A.G., Molokanova A.R., Murtazina G.Kh., Imelbaeva A.G., Kuznetsova R.R., Khusnutdinova M.N.
Vaginal natural orifice transluminal endoscopic surgery (vNOTES) hysterectomy is the most modern approach to this procedure, involving a transvaginal hysterectomy performed using an endoscope.
Objective: To evaluate the effectiveness of vNOTES hysterectomy compared with the traditional laparoscopic approach based on intraoperative and postoperative parameters.
Materials and methods: This study included 200 patients aged 45–75 years who had undergone hysterectomy. In the VEH group, a hysterectomy was performed using the vNOTES approach, whereas in the LH group, a laparoscopic hysterectomy was performed. The study cohort was analyzed for anthropometric and anamnestic characteristics, obstetric and gynecological history, total operative time, time to hysterectomy, total blood loss, surgical table angle, extension of the surgical procedure, intraoperative and postoperative complications, and number of days until hospital discharge.
Results: The groups were comparable in terms of anthropometric parameters, age, number of pregnancies, parity, total operative time, blood loss, hospital stay, and absolute number of complications. The VEH group showed statistically significant advantages in terms of shorter time to hysterectomy -17.0 (95% CI 0.54–1.12; р-value<0.001; dCohen=0.83); lower maximum CO2 pressure 2,0 (95% CI 1.06–1.68; р-value<0.001;
dCohen=1.37); a smaller operating table inclination -10.0 (95% CI 2,81–3,65; р-value<0,001; dCohen=3,2, shorter time of vaginal stump suturing -8.0 (95% CI, 2.52–3.32; p-value<0.001; dCohen= 2.92) and reduction of postoperative pain at 6 and 24 hours after surgery -1.0 (95% CI 0.24–0.8; p-value<0.001; dCohen=0.52) and -1.0 (95% CI 0.26–0.82; p-value<0.001; dCohen=0.54), respectively. The VEH group also had the advantage of not requiring an incision on the anterior abdominal wall, which had a beneficial effect in the postoperative period.
Conclusion: The results demonstrate the advantages of the vNOTES approach over the traditional laparoscopic approach to hysterectomy.
Authors' contributions: Musin I.I. – conception and design of the study, data collection; Berg E.A. – drafting of the manuscript, statistical analysis, data collection; Yashchuk A.G. – conception and design of the study, drafting of the manuscript, approval of the final version of the article; Molokanova A.R., Murtazina G.Kh. – editing of the manuscript, data collection; Imelbaeva A.G. – editing of the manuscript; Kuznetsova R.R., Khusnutdinova M.N. – data collection.
Conflicts of interest: The authors have no conflicts of interest to declare.
Funding: There was no funding for this study.
Ethical Approval: The study was reviewed and approved by the Research Ethics Committee of the Bashkir State Medical University, Ministry of Health of Russia.
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Musin I.I., Berg E.A., Yashchuk A.G., Molokanova A.R., Murtazina G.Kh.,
Imelbaeva A.G., Kuznetsova R.R., Khusnutdinova M.N. vNOTES hysterectomy.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (3): 95-103 (in Russian)
https://dx.doi.org/10.18565/aig.2025.332
Keywords
hysterectomy
vNOTES
vaginal endoscopic hysterectomy
laparoscopic hysterectomy
minimally invasive gynecology
comparative analysis of operations
Hysterectomy is one of the most frequently performed surgical procedures worldwide and ranks first among gynecological operative interventions [1–3]. Benign gynecologic diseases are the most common indications for hysteroscopy, accounting for over 90% of cases [2–4]. Uterine removal can be achieved through various surgical approaches, including the vaginal route, laparotomy, conventional laparoscopy, robotic-assisted laparoscopy, and their combinations. However, a 2023 Cochrane Library analysis recommends classifying endovideosurgical approaches as "minimally invasive".
In developed countries, 81.5% of the more than half a million hysterectomies performed annually are conducted endoscopically [5]. Nevertheless, a systematic analysis by Lefant L. et al., encompassing 24 large studies from different continents, reported that classical laparotomy is still used in 49.6% of cases [6].
Vaginal hysterectomy is the preferred approach for uterine removal in cases of benign pathology [6–8]. This preference is based on evidence of a faster return to normal activity, a lower rate of wound/abdominal wall infections, shorter hospital stays [6, 8], and the absence of cosmetic defects on the anterior abdominal wall.
However, the classical vaginal approach to intra-abdominal surgery presents technical challenges, including an acute operative angle and limited visualization of the surgical field [4, 8]. Patient-specific clinical features, such as obesity, absence of pelvic organ prolapse, large uterine size, and intra-abdominal adhesions, can complicate vaginal hysterectomy and may necessitate alternative surgical access methods [4, 6, 8, 9].
Minimally invasive approaches also include natural orifice transluminal endoscopic surgery (NOTES). This technique utilizes natural orifices as access routes for endovideosurgical instruments to perform surgery. The vagina is the preferred natural orifice for hysterectomy (vNOTES). Combining this approach with endoscopic instruments can overcome the limitations of classical vaginal surgery [2, 4, 10].
vNOTES hysterectomy is associated with a shorter hospital stay, a lower rate of infections, reduced costs, earlier return to usual activities, and the absence of abdominal scars [2, 4, 5, 8, 10].
Despite these advantages, recent systematic reviews have highlighted the need for continued research to assess the effectiveness of the vNOTES approach for hysterectomy.
This study aimed to evaluate the effectiveness of vNOTES hysterectomy compared to the conventional laparoscopic approach based on intraoperative and postoperative outcomes.
Materials and methods
Study object
A retrospective analysis was performed on the hysterectomy outcomes of 200 patients who underwent the procedure at the Gynecology Department of the Clinic of Bashkir State Medical University, Ministry of Health of Russia (Ufa), between September 2022 and June 2025.
The inclusion criteria were as follows: women aged 45 to 75 years with benign gynecological conditions requiring planned hysterectomy, provision of informed consent, and absence of or grade I–II (inclusive) pelvic organ prolapse according to the Pelvic Organ Prolapse Quantification (POP-Q) system.
The exclusion criteria were as follows: failure to meet the age criteria, refusal to participate, presence of malignant disease, pelvic organ prolapse greater than grade II (POP-Q), or retrocervical endometriosis.
Surgical procedures
The participants were divided into two groups based on the hysterectomy technique used.
In the LH group (n=100), a standard laparoscopic hysterectomy was performed according to the 2019 recommendations of the European Society for Gynecological Endoscopy (ESGE) [11]. This procedure involved creating a pneumoperitoneum using a Veress needle, inserting endoscopic trocars through the anterior abdominal wall, transecting the round and infundibulopelvic or ovarian ligaments, dissecting the vesicouterine fold, incising the posterior peritoneal leaf, transecting the uterine vessels, performing a colpotomy, removing the uterus through the colpotomy opening, closing the vaginal cuff with endoscopic hand sutures, verifying hemostasis, desufflating the abdomen, removing the trocars, and closing the skin. A Clermont-Ferrand-type uterine manipulator was used to position the uterus in the abdominal cavity.
In the VEH group (n=100), a hysterectomy was performed using the vaginal natural orifices transluminal endoscopic surgery (vNOTES) approach in the following sequence: vaginal stage: the cervix was exposed using a vaginal speculum. A circumferential incision was made in the cervical mucosa, followed by transection of the cardinal and uterosacral ligaments. An anterior or posterior colpotomy was performed, and a self-retaining retractor (Fig. 1) and glove-port system with pre-mounted disposable or metal endoscopic trocars (Fig. 2) were inserted. Endoscopic stage: The uterine vessels (Fig. 3), broad ligaments, ovarian ligament (Fig. 4), and isthmic portion of the fallopian tubes were sequentially and bilaterally transected.
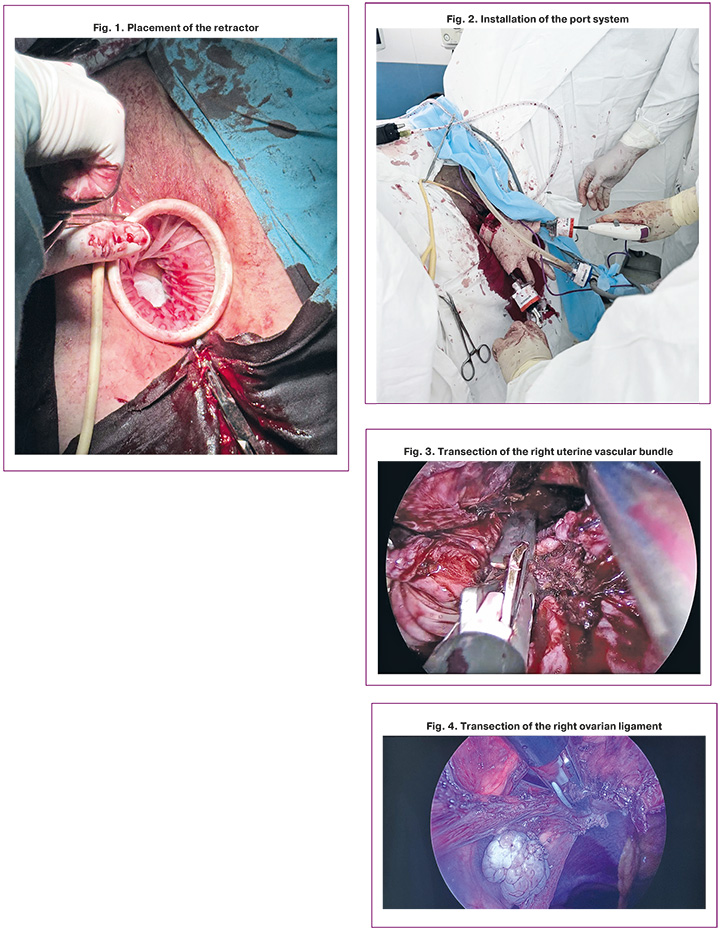
The specimen was removed through the vagina, and the tubal stumps were excised at the mesosalpinx level. Hemostasis was verified, and the vaginal cuff was closed, followed by pelvic floor reconstruction or other surgical interventions if indicated.
All patients underwent a preoperative clinical evaluation. Antibacterial prophylaxis was administered as a 2 g dose of antibiotic (ATC code: J01DB04) 30–60 min before surgery. All procedures were performed with the patient in the standard lithotomy position, with the table tilt angle adjusted as needed under endotracheal anesthesia.
Outcome measures
Successful surgical outcome was defined as the complete removal of the uterus and fallopian tubes. Comparative analysis between the groups included assessment of anthropometric and background characteristics, obstetric and gynecologic history, total operative time, time to uterus extirpation, intraoperative blood loss, table tilt angle, need for extended surgical intervention, intraoperative and postoperative complications, pain scores on a visual analog scale (VAS) at 6 and 24 h postoperatively, and length of hospital stay.
Pain intensity was assessed using a 10 cm horizontal VAS, ranging from 0 to 10, where 0 indicated "no pain" and 10 indicated "worst imaginable pain".
Statistical analysis
Statistical analysis was performed using Microsoft Excel, Statistica 10.0, and GraphPad software. A p-value of less than 0.05 (p<0.05) was considered statistically significant. The Shapiro–Wilk test was used to assess the normality of the data distribution. The Mann–Whitney U test was used to compare two independent groups with quantitative or ordinal variables that did not follow normal distribution. Non-normally distributed data were presented as the median (Me) and interquartile range (IQR) in the format Me [Q1; Q3].
For binary outcomes, effect size was expressed as relative risk or risk difference with 95% confidence intervals (CI). For continuous data, the effect size was expressed as the difference in means or medians with 95% CI. Cohen's d coefficient (dCohen) was used to provide a standardized measure of effect size.
Results and discussion
Anthropometric and anamnestic data
A comparative analysis of the groups was performed based on the number of pregnancies and deliveries, body mass index, and age (Table 1). Analysis of the patients’ anthropometric characteristics revealed no significant differences between the groups.
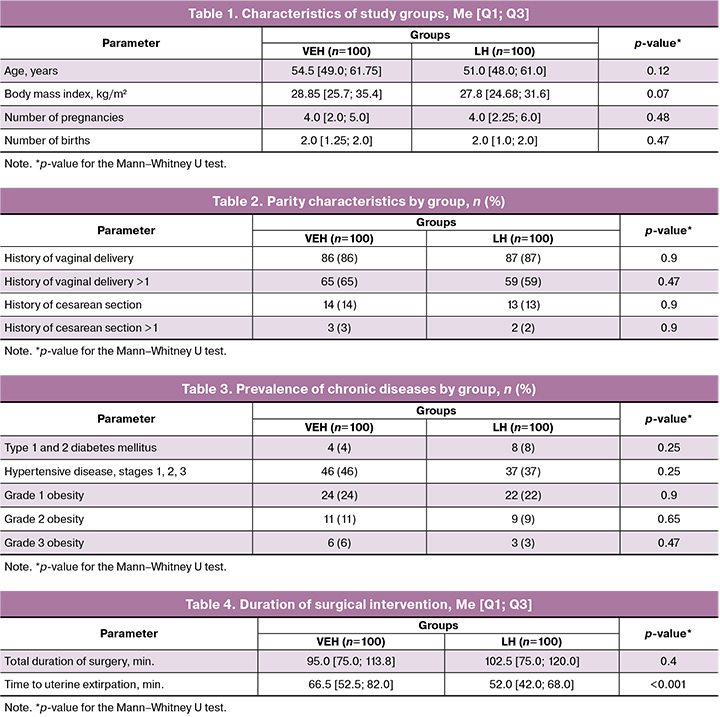
The patients’ age in both groups generally corresponded to the postmenopausal period (VEH group: 54.5 [49.0; 61.75] years; LH group: 51.0 [48.0; 61.0] years) and did not differ significantly between the groups (p=0.12, U = 4360).
Analysis of reproductive history revealed no statistically significant differences (Table 2). Likewise, no significant group differences were observed in the prevalence of the most common somatic diseases (Table 3).
The duration of menopause was 2.0 [0.0; 11.75] years in the VEH group and 2.0 [0.0; 10.0] years in the LH group (p=0.34, U = 4529).
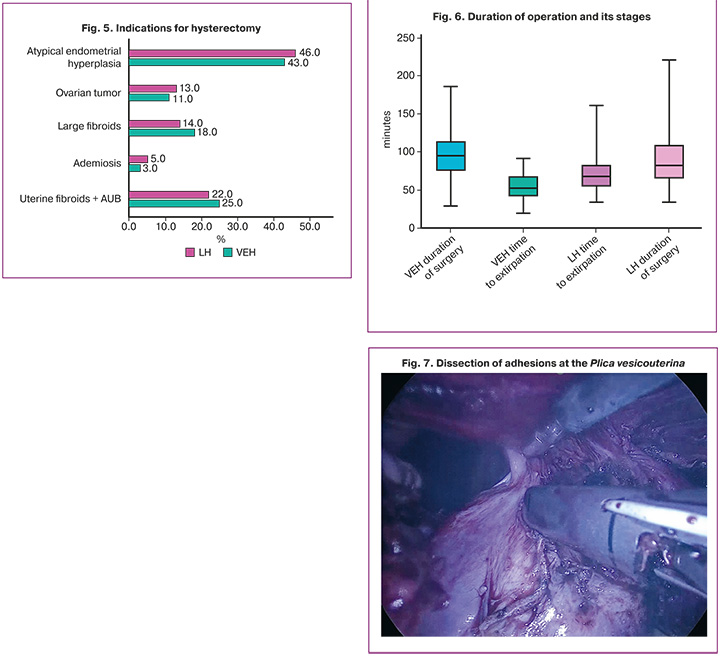
The indications for hysterectomy are presented in Figure 5. Analysis revealed no differences between the groups for any indication (p>0.1 in all cases).
Intraoperative characteristics
The mean duration of the procedure was 95.0 [75.0; 113.8] min in the VEH group and 102.5 [75.0; 120.0] min in the LH group, without statistically significant differences (Δ=13.0, 95% CI -0.56–0.004; p=0.4; dCohen=-0.275).
When the individual operative stages were analyzed, the time to uterine extirpation was longer in the LH group (66.5 [52.5; 82.0] min) than in the VEH group (52.0 [42.0; 68.0] min), with a statistically significant difference (Δ=-17.0, 95% CI 0.54–1.12; p<0.001; dCohen=0.83) (Fig. 6, Table 4).
All patients in the LH group underwent surgery using a uterine manipulator, as dictated by the laparoscopic hysterectomy technique. In contrast, all manipulations of the uterus in the VEH group were performed externally (traction on the cervix and ligament stumps), which provides certain technical advantages and reduces the number of personnel required during surgery. In oncological cases with unverified diagnoses, the absence of a manipulator may also confer a beneficial ablastic effect.
A distinctive feature of the procedures in the VEH group was the frequent combination of hysterectomy with simultaneous interventions, such as unilateral or bilateral tubectomy, unilateral or bilateral adnexectomy, bilateral fixation of the vaginal vault to the midportion of the uterosacral ligaments, or reconstruction of pelvic connective tissue structures. For both the LH and VEH groups, the only routinely added procedure was tubectomy, which was performed in all cases except when adnexectomy was performed (Table 5).
The more frequent use of adhesiolysis techniques in the LH group likely reflects the more difficult access to the uterus due to pelvic adhesions in this group.
Transvaginal access offers distinct advantages in managing hysterectomy in patients with adhesions between the posterior bladder wall and uterus. When adhesions are localized at the isthmus, performing the vaginal stage and establishing the port system allows separation of the uterus from the ligaments and tubes, followed by dissection of adhesions in the plica vesicouterina, thereby minimizing the risk of bladder injury (Fig. 7).
It should be noted that dissection of adhesions between the uterus and bladder dome was not a separate stage in VEH procedures but occurred naturally after uterine extirpation, as the subsequent dissection of the broad ligament and partial blunt separation of the anterior visceral peritoneum posed no technical difficulties.
The maximal intra-abdominal pressure was 12.0 [12.0; 14.0] mmHg in the LH group and 10.0 [9.0; 11.0] mmHg in the VEH group, a significant difference (Δ=-2.0, 95% CI 1.06–1.68; p<0.001; dCohen= 1.37). The CO₂ flow rate was 0.5–0.6 L/min in all the cases.
The difference in gas pressure largely reflected variation in the angle of table inclination: 5.0 [5.0; 7.0] degrees in VEH and 15.0 [12.0; 15.0] degrees in LH (Δ=-10.0, 95% CI 2.81–3.65; p<0.001; dCohen= 3.2). These differences arise from the anatomical characteristics of the approaches. In vNOTES, the trocar is inserted in a plane nearly horizontal to the uterus and its ligaments, allowing tissue division with minimal Trendelenburg positioning (primarily for the protection of intra-abdominal organs) (Fig. 8). In contrast, laparoscopic hysterectomy generally requires a table inclination of approximately 12°, highlighting one of the ergonomic advantages of the vaginal approach.
The mean duration of vaginal vault closure differed significantly between the groups: 9.0 [7.0; 10.0] min in the VEH group versus 17.0 [15.0; 19.0] min in the LH group (Δ=-8.0, 95% CI 2.52–3.32; p<0.001; dCohen= 2.92). A longer suturing time during laparoscopic hysterectomy is often due to adjacent organs losing part of their connective support after uterine removal, limiting visualization of vault edges, an effect that is more pronounced in obese patients.
A notable finding was the substantial reduction in the median time to uterine extirpation with accumulated experience in performing vNOTES (VEH group). Between 2022 and 2023, the mean duration was 68.5 [46.5; 79.25] min (n=30), whereas in 2024–2025, it decreased by approximately one-third (31.3%) to 47.0 [40.0; 58.5] min (n=70).
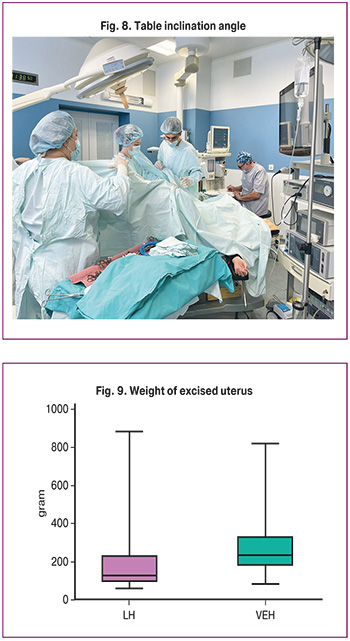
The excised uterine weights differed significantly between the groups: 232.2 [181.0; 334.3] g in VEH and 128.0 [99.25; 230.0] g in LH (p<0.001) (Fig. 9). For larger uteri, laparoscopic procedures often require assistance from an additional surgeon to provide organ traction, as the uterine manipulator alone may not allow for optimal positioning. In contrast, vaginal access enables direct traction on the cervix or ligament stumps.
Specimen removal was performed through the vaginal vault in all cases, requiring morcellation in 70% (140/200) of the cases. In 46% of LH cases, however, extraction necessitated an extension of the abdominal wall incision. Notably, the vaginal retractor used in the first stage of VEH completely isolates the operative field, serving as a barrier to protect the surrounding tissues during morcellation.
The analysis of intraoperative blood loss revealed no significant difference between groups (Δ=-45.0, 95% CI -0.28–0.28; p=0.06; dCohen= 0.001): 150.0 [120.0; 202.0] mL in the VEH group and 125.0 [50.0; 237.5] mL in the LH group.
Intraoperative complications occurred in 1% (1/100) of VEH cases (bladder wall injury in a patient with a history of repeated cervical electrosurgical procedures) and in 8% (8/100) due to blood loss >200 mL. In the LH group, excessive bleeding was observed in 10% (10/100), bladder injury in 2% (2/100), and ureteral injury in 2% (2/100) of the patients.
Postoperative complications included vaginal vault infection in 10% (10/100) of VEH and 12% (12/100) of LH cases; vault hematoma requiring suture removal occurred in 2% (2/100) of VEH and 1% (1/100) of LH cases.
In our view, the rate of preventable intraoperative complications is directly correlated with surgical experience; accordingly, based on the present data, it is not possible to assert a clear advantage of either approach in preventing complications.
No patient in either group required postoperative intensive care unit admission.
Pain intensity 6 h after surgery differed significantly between groups: median VAS 4 [4; 6] in VEH versus 5 [5; 6] in LH (Δ=-1.0, 95% CI 0.24–0.8; p<0.001; dCohen=0.52).
At 24 h postoperatively, the VAS scores also differed (VEH: 2 [1, 3]; LH: 3 [2, 4]; Δ=-1.0, 95% CI 0.26–0.82; p<0.001; dCohen=0.54).
In our view, pain reduction is one of the main advantages of the vaginal approach, facilitating early postoperative mobilization.
The postoperative hospital stay did not differ significantly between the two groups, with a median of 4 days in both groups.
Conclusion
vNOTES is an effective alternative to the laparoscopic approach for hysterectomy. The absence of an incision on the anterior abdominal wall is a distinct advantage over any transabdominal intervention, facilitating postoperative rehabilitation and improving the aesthetic outcomes. vNOTES hysterectomy offers additional benefits, including no statistically significant differences in blood loss and operative time; a significant reduction in the time required for uterine removal; lower maximum intraperitoneal gas pressure values; smaller table tilt angles; a shorter time required for closure of the vaginal cuff; and statistically significant reductions in postoperative pain at 6 and 24 hours after surgery.
Additional advantages include eliminating the need for a uterine manipulator, separating the vaginal cuff from the removed organ during morcellation using a retractor, and the possibility of performing simultaneous procedures to prevent post-hysterectomy prolapse and injury to the ureters and adjacent organs during uterine ventrofixation.
References
- Wright J.D., Huang Y., Li A.H., Melamed A., Hershman D.L. Nationwide estimates of annual inpatient and outpatient hysterectomies performed in the United States. Obstet. Gynecol. 2022; 139(3): 446-8. https://dx.doi.org/10.1097/AOG.0000000000004679
- Marchand G.J., Ulibarri H., Arroyo A., Blanco M., Herrera D.G., Hamilton B. et al. Systematic review and meta-analysis of vaginal natural orifice transluminal endoscopic surgery hysterectomy versus vaginal hysterectomy for benign indications. AJOG Glob. Rep. 2024; 4(2): 100355. https://dx.doi.org/10.1016/j.xagr.2024.100355
- Ищенко А.И., Ищенко А.А., Хохлова И.Д., Джибладзе Т.А., Горбенко О.Ю., Александров Л.С., Гадаева И.В., Гаврилова Т.В., Тарасенко Ю.Н., Асамбаева А., Тевлина Е.В. Опыт использования линейных сшивающе-режущих и сшивающих аппаратов при влагалищной гистерэктомии. Вопросы гинекологии, акушерства и перинатологии. 2022; 21(5): 125-8. [Ishchenko A.I., Ishchenko A.A., Khokhlova I.D., Dzhibladze T.A., Gorbenko O.Yu., Aleksandrov L.S., Gadaeva I.V., Gavrilova T.V., Tarasenko Yu.N., Asambaeva A., Tevlina E.V. Experience of using linear cutting-stapling and stapling devices in vaginal hysterectomy. Gynecology, Obstetrics and Perinatology. 2022; 21(5): 125-8 (in Russian)]. https://dx.doi.org/10.20953/1726-1678-2022-5-125-128
- Baron C., Netter A., Tourette C., Pivano A., Agostini A., Crochet P. Initial experience with vNOTES hysterectomy for benign conditions in a French university hospital. Facts Views Vis. Obgyn. 2022; 14(2): 147-53. https://dx.doi.org/10.52054/FVVO.14.2.018
- Cohen S.L., Ajao M.O., Clark N.V., Vitonis A.F., Einarsson J.I. Outpatient hysterectomy volume in the United States. Obstet. Gynecol. 2017; 130(1): 130-7. https://dx.doi.org/10.1097/AOG.0000000000002103
- Lenfant L., Canlorbe G., Belghiti J., Kreaden U.S., Hebert A.E., Nikpayam M. et al. Robotic-assisted benign hysterectomy compared with laparoscopic, vaginal, and open surgery: a systematic review and meta-analysis. J. Robot. Surg. 2023; 17(6): 2647-62. https://dx.doi.org/10.1007/s11701-023-01724-6
- Aarts J.W., Nieboer T.E., Johnson N., Tavender E., Garry R., Mol B.W. et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst. Rev. 2015; 2015(8): CD003677. https://dx.doi.org/10.1002/14651858.CD003677.pub5
- Pickett C.M., Seeratan D.D., Mol B.W.J., Nieboer T.E., Johnson N., Bonestroo T. et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst. Rev. 2023; 8(8): CD003677. https://dx.doi.org/10.1002/14651858.CD003677.pub6
- Oliva R., Forgione A., Akladios C., Querleu D., Mastrovito S., Pavone M. et al. Is vaginal hysterectomy outdated? A systematic overview of reviews with future perspectives. J. Gynecol. Obstet. Hum. Reprod. 2025; 54(7): 102968. https://dx.doi.org/10.1016/j.jogoh.2025.102968
- Housmans S., Stuart A., Bosteels J., Deprest J., Baekelandt J. Standardized 10-step approach for successfully performing a hysterectomy via vaginal natural orifice transluminal endoscopic surgery. Acta Obstet. Gynecol. Scand. 2022; 101(6): 649-56. https://dx.doi.org/10.1111/aogs.14367
- Working group of ESGE. Surgical steps of total laparoscopic hysterectomy: Part 1: Benign disease by the European Society for Gynaecological Endoscopy (ESGE). Facts Views Vis. Obgyn. 2019; 11(2): 103-10.
Received 17.11.2025
Accepted 29.01.2026
About the Authors
Ilnur I. Musin, Dr. Med. Sci., Professor, Department of Obstetrics and Gynecology No. 2, Bashkir State Medical University, Ministry of Health of Russia, 450008, Russia, Ufa, Lenin str., 3, +7(917)467-10-64, ilnur-musin@yandex.ru, https://orcid.org/0000-0001-5520-5845Edward A. Berg, PhD, Associate Professor, Department of Obstetrics and Gynecology No. 2, Bashkir State Medical University, Ministry of Health of Russia, 450008, Russia, Ufa, Lenin str., 3, +7(927)337-90-03, nucleardeer@gmail.com, https://orcid.org/0000-0002-2028-7796
Alfiya G. Yashchuk, Dr. Med. Sci., Professor, Head of the Department of Obstetrics and Gynecology No. 2, Bashkir State Medical University, Ministry of Health of Russia, 450008, Russia, Ufa, Lenin str., 3, +7(347)264-96-50, alfiya_galimovna@mail.ru, https://orcid.org/0000-0002-6725-2603
Angella R. Molokanova, PhD, Assistant Lecturer, Department of Obstetrics and Gynecology No. 2, Bashkir State Medical University, Ministry of Health of Russia,
450008, Russia, Ufa, Lenin str., 3, +7(917)349-04-72, angella1210@mail.ru, https://orcid.org/0000-0003-1115-6775
Gulnaz H. Murtazina, PhD, Associate Professor, Department of Obstetrics and Gynecology No. 2, Bashkir State Medical University, Ministry of Health of Russia,
450008, Russia, Ufa, Lenin str., 3, +7(917)349-04-72, karamelka5@inbox.ru, https://orcid.org/0000-0001-9529-3747
Albina G. Imelbaeva, PhD, Associate Professor, Department of Obstetrics and Gynecology No. 2, Bashkir State Medical University, Ministry of Health of Russia,
450008, Russia, Ufa, Lenin str., 3, +7(917)349-04-72, albina220588@gmail.com, https://orcid.org/0000-0002-0558-1364
Regina R. Kuznetsova, resident, Department of Obstetrics and Gynecology No. 2, Bashkir State Medical University, Ministry of Health of Russia, 450008, Russia, Ufa,
Lenin str., 3, +7(917)421-87-84, regina18402@gmail.com, https://orcid.org/0009-0000-9139-5375
Mariia N. Khusnutdinova, resident, Department of Obstetrics and Gynecology No. 2, Bashkir State Medical University, Ministry of Health of Russia, 450008, Russia, Ufa,
Lenin str., 3, +7(982)283-00-95, maria.medartz@gmail.com, https://orcid.org/0009-0006-7806-0013
Similar Articles

