
Comparative analysis of postpartum depression based on the Edinburgh scale in women of different age groups under and over 35 years
Subanova G.A., Subanova N.A., Askerov A.A., Yrysbaev E.Y., Nurbek kyzy A., Yrysbaev A.Y., Muratova G.K.
Objective: To determine the prevalence and severity of postpartum depression (PPD) symptoms among women in Osh using the Edinburgh Postpartum Depression Scale (EPDS) and to compare these symptoms across different age groups (under and over 35 years) and by parity.
Materials and methods: The study included 73 women from Osh, aged 18 to 49 years (mean age 33.5 years), and divided them into three age groups: 18–25 years, 25–35 years, and >35 years. Depressive symptoms were assessed using the Edinburgh Postpartum Depression Scale (EPDS), a 10-item questionnaire. Data were collected via electronic questionnaires in Google Forms, processed in Microsoft Excel, and analyzed using IBM SPSS Statistics 23. Statistical analysis included calculating means, standard deviations, and correlations between age, parity, and depressive symptoms.
Results: Depressive symptoms were identified in 57% of the women during the postpartum period. The highest severity of PPD symptoms was observed in women younger than 25 years, particularly during the first week postpartum (64%), with a gradual decrease by the sixth week (45%) and after the seventh week (39%). Primiparous women exhibited a higher level of depression (58%) than multiparous women. An inverse correlation was found between age and parity and the severity of depressive symptoms: as age and the number of births increased, depressive symptoms decreased. Women who experienced complications during pregnancy and childbirth more frequently reported anxiety and depression.
Conclusion: The study confirmed a high prevalence of PPD symptoms among women in Osh, particularly among young and primiparous women. Age and parity significantly influenced the level of depression, with older and multiparous women showing a lower propensity for PPD. Effective prevention and management of PPD require early screening, especially during the first week postpartum, development of psychological support programs, and increased awareness among women regarding available resources.
Authors' contributions: Subanova N.A., Askerov A.A. – conception and design of the study; Subanova G.A, Muratova G.K. – data collection and analysis; Yrysbaev Y.E. – statistical analysis; Nurbek kyzy A. – drafting of the manuscript; Yrysbaev Y.E., Yrysbaev Y.A. – editing of the manuscript.
Conflicts of interest: The authors have no conflicts of interest to declare.
Funding: There was no funding for this study.
Ethical Approval: The study was reviewed and approved by the Biomedical Ethics Committee of the International Medical Faculty of Osh State University on February 17, 2025.
Patient Consent for Publication: All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Subanova G.A., Subanova N.A., Askerov A.A., Yrysbaev E.Y., Nurbek kyzy A.,
Yrysbaev A.Y., Muratova G.K. Comparative analysis of postpartum depression based
on the Edinburgh scale in women of different age groups under and over 35 years.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (3): 85-94 (in Russian)
https://dx.doi.org/10.18565/aig.2025.237
Keywords
postpartum depression
Edinburgh scale
age
parity
anxiety-depressive states
screening
psychological support
Postpartum depression is a prevalent and serious disorder that diminishes women's quality of life and their ability to adapt to motherhood. According to Edel’khanova A. et al., the postpartum period is considered a time of increased risk for the development of depression due to the physiological, psychological, and social changes accompanying pregnancy, childbirth, and the early postpartum period [1]. At present, antenatal and postpartum depression (PPD) remain significant social problems, as emphasized by Ebina Y. et al. [2]. Women suffering from these disorders often struggle to fulfill parental responsibilities and function effectively in their social environments. Research indicates that maternal depression negatively impacts a child's cognitive and social development [3, 4]. Furthermore, the risk of depressive relapse increases with subsequent births, especially when psychotic symptoms are present.
Many countries are actively developing effective screening programs and diagnostic methods for the timely identification of PPD [3]. However, despite efforts to raise awareness of PPD and its adverse effects on mothers and families, approximately 50% of PPD cases remain undiagnosed, and most women with the condition do not seek professional help, as noted by Mazo G.E. et al. [5].
The World Health Organization predicts that depressive disorders will become the leading category of disease in the coming years, surpassing cardiovascular and oncological pathologies. The prevalence of antidepressant use among women in the United States and the United Kingdom (approximately 15%) highlights the relevance and scale of this problem [6]. Research by Tatarova N.A. et al. demonstrated that maternal depression can disrupt mother–child interactions, which subsequently affects the child's development and health [7].
Approximately 22% of women experience symptoms of depression during the first six months after childbirth, while depressive disorders within narrower time intervals (4–9 weeks) are diagnosed less frequently (13–16%) [7]. However, the true prevalence of PPD may be higher because many women do not seek medical assistance. In Kazakhstan, the prevalence of PPD is approximately 15%, according to Abdieva N. et al. [8].
Studies by Karlson K. et al., Beck C.T., and O'Hara M.W. et al. indicate that PPD is a common and potentially severe mood disorder affecting approximately one in seven women during the first year after childbirth. PPD arises from a combination of hormonal changes, genetic predisposition, and environmental factors. However, up to 50% of cases remain undiagnosed due to the stigma surrounding the condition and patients' reluctance to disclose their symptoms [9–11].
In recent decades, the study of emotional disturbances in women during pregnancy and the postpartum period has garnered increasing attention from specialists across various fields, including obstetricians, gynecologists, psychologists, and psychiatrists. While numerous studies have examined the influence of pregnancy, childbirth, and the postpartum period on affective disorders, the dynamics and manifestations of women's emotional states have not been fully elucidated. Disturbances in the emotional sphere may contribute to complications of varying severity in obstetric and gynecological practice. Research indicates that persistent emotional disturbances prevent up to 50% of mentally healthy mothers from developing an adequate attitude toward their child during the first year of life [12].
In our region, PPD poses an increased risk because women live in an area endemic for iodine deficiency [13]. Thyroid dysfunction, particularly hypothyroidism, may exacerbate depressive symptoms, as confirmed by Tatarova et al. and Beck et al. [7, 10]. Women with endocrine pathologies are at a higher risk of developing PPD. For example, anxiety–depressive states are more frequently detected in patients with hypothyroidism, whereas anxiety symptoms predominate in hyperthyroidism. In women with hyperprolactinemia, the severity of depressive symptoms is lower, consistent with data regarding the role of thyroid disorders in the pathogenesis of anxiety–depressive disorders [7, 10]. Thus, endocrine dysfunction is an important predictor of PPD development. Therefore, conducting comparative studies of PPD among women of different age groups using the Edinburgh Postnatal Depression Scale (EPDS) is relevant for identifying specific risk factors and adapting prevention and treatment strategies.
The statistical data on the prevalence of PPD vary depending on the geographical region. In the United States, postpartum depression is diagnosed in 9% of women [14], according to Alexander E.K. et al., while in Europe, this figure is approximately 10% [14]. Globally, between 10% and 26% of women experience PPD symptoms. In Russian samples, the prevalence of these symptoms reaches 30%. Despite the scale of the problem, the systems for diagnosing and treating postpartum disorders remain underdeveloped. This is further exacerbated by the stigmatization of mental disorders in society and insufficient awareness among women about available support methods. The presence of current psychoemotional difficulties in women is positively correlated with the severity of PPD symptoms. Women who have previously experienced mental health problems demonstrate more pronounced symptoms of postpartum disorders. According to Beck C.T. and Kharchenko A.A. et al., factors such as educational level, income, marital status, and place of residence significantly impact psychoemotional well-being and access to professional assistance. Higher education and income are associated with fewer diagnosed problems and a greater likelihood of seeking help [10, 15].
Anxiety and depressive conditions are considered the most common emotional disorders in women during pregnancy and after childbirth, and may manifest with varying degrees of severity [16]. The level of anxiety during pregnancy is an important factor distinguishing physiologically normal pregnancies from complicated pregnancies. Symptoms of anxiety may occur at least once in more than 50% of pregnant women, while persistent anxiety states are observed in more than 17% of women during the period of preparation for childbirth; however, anxiety disorders are often undiagnosed.
Despite the existence of numerous methods for studying women's attitudes toward pregnancy and childbirth, there remains a lack of reliable standardized methods for detecting anxiety states in the antenatal and postpartum periods [17, 18], according to Wang Y. et al. and Nakić Radoš S. et al. Standard methods for identifying the symptoms of affective disorders used in domestic clinical psychology are most commonly applied for diagnostic purposes [7]. However, these methods are not always sensitive to the specific features of emotional states during the antenatal and postpartum periods. The high prevalence of anxiety disorders among pregnant women underscores the importance of using specialized scales to assess anxiety levels [19], according to Korgozha M.A. and Evmenenko A.O.
According to Gibson J. et al. [20], two principal approaches to understanding the nature of PPD determine the choice of screening instruments. The first considers PPD as an independent mental disorder with a specific clinical structure, justifying the need to develop specialized scales for more accurate identification. The second assumes that PPD represents the onset of depressive or bipolar disorder, allowing the use of traditional screening scales for its assessment.
Currently available screening scales are generally self-report questionnaires and cannot be considered diagnostic tools. Their primary purpose is to identify women at a high risk of developing antenatal and postpartum depression who require further diagnostic evaluation. Early identification of women predisposed to these pathological conditions allows for the timely implementation of preventive measures to minimize negative consequences for women and their families, according to Gibson J. et al. and Mazo G.E. et al. [5, 20]
This study aimed to determine the prevalence and severity of PPD symptoms among women in Osh using the Edinburgh Postpartum Depression Scale (EPDS) and to compare these symptoms across different age groups (under and over 35 years) and by parity.
Materials and methods
This cross-sectional study included postpartum women who received care at a municipal maternity hospital in Osh between November and December 2024.
The inclusion criteria were as follows: women in the postpartum period (1–12 months after delivery), residing in Osh, aged 18–49 years (mean age, 33.5 years), and able to complete an electronic questionnaire.
The exclusion criteria were a self-reported history of diagnosed mental disorders prior to pregnancy, refusal to participate, or incomplete questionnaires.
Participants were recruited via convenience sampling using a Google Forms questionnaire distributed in antenatal clinics and social media. The final sample comprised 73 women.
Eligible women completed a questionnaire that included five general questions and the Edinburgh Postnatal Depression Scale (EPDS). The EPDS assessed women 's mood over the preceding 7 days and consisted of 10 items, each scored from 0 to 3 (maximum total score: 30). A score of ≥10 was considered indicative of postpartum depression (PPD).
Statistical analysis
Data were analyzed using Microsoft Excel and IBM SPSS Statistics version 23. Descriptive statistics included medians (Me) and interquartile ranges [Q1; Q3] for quantitative variables (total EPDS score, age, and parity, the latter treated as an ordinal variable), as well as absolute frequencies (n) and proportions (%) for categorical variables (responses to individual EPDS items and presence of PPD symptoms, defined as EPDS ≥10).
The distribution of the total EPDS score was assessed for normality using the Shapiro–Wilk test, which confirmed a non-normal distribution (p<0.001). Consequently, only nonparametric methods were used in this study.
The Kruskal–Wallis test was used to compare total EPDS scores across three or more independent groups (age groups and parity groups). Where overall differences were statistically significant (p<0.05), pairwise comparisons were performed using the Mann–Whitney U test with Bonferroni correction (critical significance level p<0.0167 for three pairwise comparisons).
The Mann–Whitney U test was used to compare the total EPDS scores between the two groups (presence vs. absence of pregnancy or delivery complications).
Spearman's rank correlation coefficient (ρ) was used to assess the association of age and parity with the total EPDS score.
The distribution of responses to individual EPDS items across groups was analyzed using the χ² test or Fisher's exact test (when expected frequencies were <5 in ≥20% of cells in the contingency table). Where overall differences across more than two groups were statistically significant (p<0.05), pairwise comparisons were performed using Fisher's exact test with Bonferroni correction (critical significance level p<0.0167).
Statistical significance was set at p<0.05 (two-tailed) for all tests. The analysis was performed in accordance with the SAMPL guidelines and the methodological recommendations of Rebrova O.Yu. [21].
Results
The study included 73 postpartum women residing in Osh. The median age was 27 [22; 33] years and the median parity was 2 [1; 3].
The distribution by age group was as follows: 18–25 years: 36/73 (49.3%); 26–35 years: 25/73 (34.2%); ≥36 years: 12/73 (16.4%).
Distribution by parity: first child: 36/73 (49.3%); 2–3 children: 27/73 (37.0%); ≥4 children: 10/73 (13.7%).
Complications of pregnancy, delivery, or the postpartum period were reported by 19/73 women (26.0%).
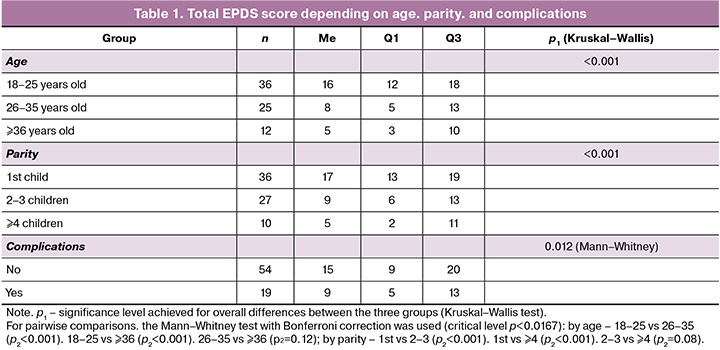
The total score on the Edinburgh Postnatal Depression Scale (EPDS) in the overall sample was 15 [5; 17]. Symptoms of PPD (total score ≥10) were identified in 44/73 women (60%).
Statistically significant differences were found between age groups (p<0.001) and parity groups (p<0.001).
Pairwise comparisons using the Mann–Whitney U test with Bonferroni correction (critical significance level, p<0.0167) showed the following:
- By age: significant differences were observed between the 18–25 and 26–35 age groups (p=0.001) and between the 18–25 and ≥36 age groups (p<0.001). Differences between the 26–35 and ≥36 age groups were not significant (p=0.12).
- By parity: significant differences were observed between primiparous women and women with 2–3 deliveries (p<0.001) and between primiparous and multiparous women (≥4 deliveries) (p<0.001). Differences between women with 2–3 deliveries and multiparous women were not statistically significant (p=0.08).
Differences in total EPDS scores between women with and without pregnancy or delivery complications were assessed using the Mann–Whitney U test. The scores were significantly lower in the group with complications (p=0.012) (Table 1).
The main results of the study conducted using the Edinburgh PPD scale showed significant differences in the severity of emotional states between women of different age groups (Table 2).
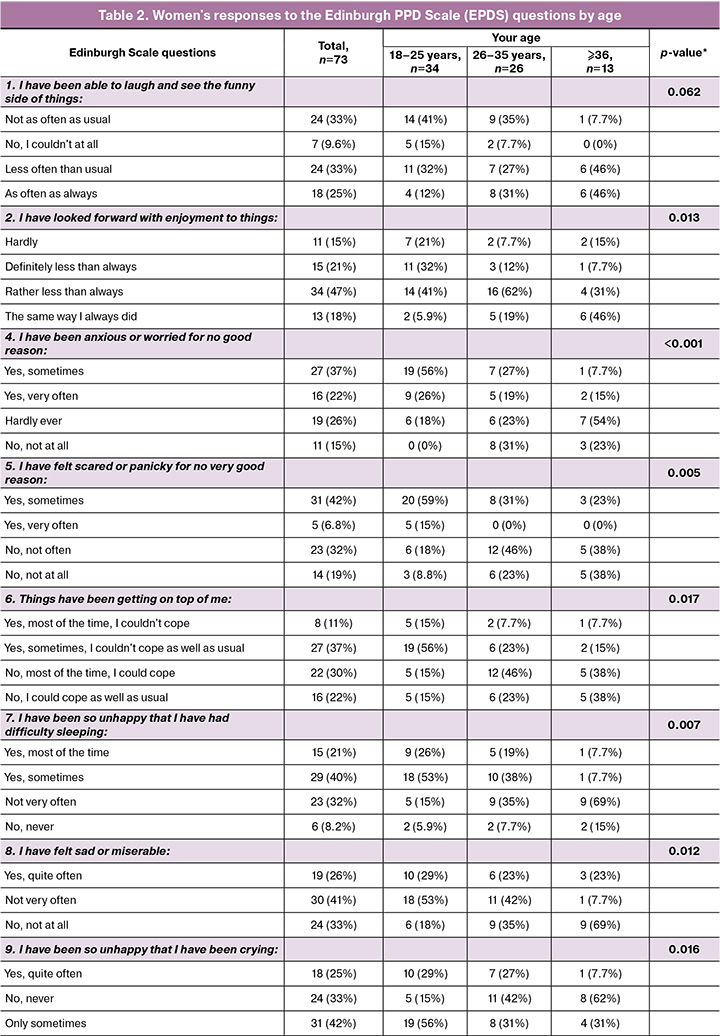
The most pronounced symptoms of anxiety, depression, and feelings of being overwhelmed were observed in women aged 18–25 years. It was in this group that manifestations of anxiety without an apparent cause (p<0.001), feelings of fear or panic without significant cause (p=0.005), feelings of inability to cope with what was happening (p=0.017), sleep disturbances (p=0.007), and increased tearfulness (p=0.016) were observed. It was also in this age group that there were more frequent cases of decreased interest in life events (p=0.013) and episodes of depressed mood (p=0.012).
Participants aged 26–35 occupied an intermediate position: they showed moderate manifestations of anxiety and emotional instability; however, the indicators were lower than in the younger group.
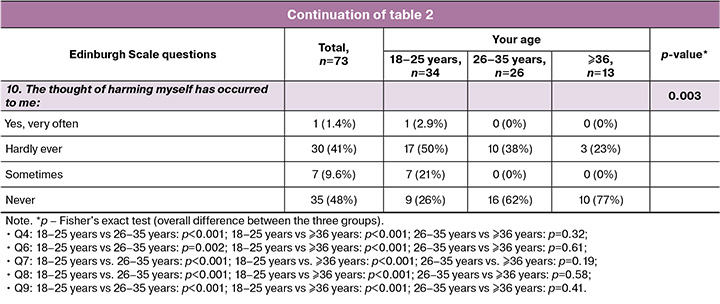
Women over 36 years showed the least pronounced symptoms of depression and anxiety. They were more likely to retain the ability to enjoy themselves and perceive the positive aspects of what was happening, less likely to experience feelings of fear and overload, and reported almost no sleep disturbances or thoughts of self-harm (p=0.003).
Thus, with age, there is a marked tendency toward a decrease in anxiety and depressive symptoms. Young women, especially those under the age of 25, were found to be the most vulnerable group in need of additional psychological support and preventive measures to prevent PPD.
The results of a study conducted using the Edinburgh PPD scale showed that the level of emotional stress in women is related to the order number of the child. The most pronounced depressive symptoms were observed in mothers with one child. Thus, when assessing the statement “I felt unhappy,” women with their first and second children more often reported that they did not feel unhappy (59% and 41%, respectively), while among women with four and five children, the proportion of “yes, quite often” responses increased to 17–20%, and there were no “no, not at all” responses in the group with four children (p=0.002).
A similar trend was found in the question “I was unhappy and cried often.” Among women with one child, the frequency of “yes, quite often” responses was 14%, which increased to 50% among women with three children and 75% among women with four children. This indicates an increase in emotional instability and tearfulness with an increase in the number of children (p=0.007).
Particular attention should be paid to indicators that reflect the presence of thoughts of self-harm. Women with one or two children reported such thoughts in 53–55% of cases, while with three or more children, the frequency of such responses reached 60–80%. At the same time, the number of “never” responses decreased significantly (p=0.035).
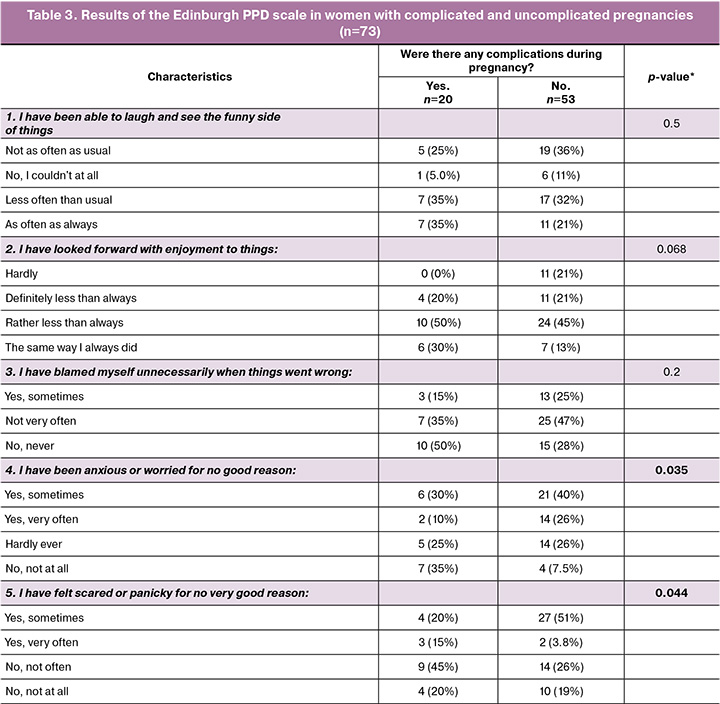
Women who experienced complications during pregnancy tended to demonstrate a more stable emotional state and less severe depressive symptoms than those with complication-free pregnancies (Table 3). Thus, when asked, “I felt unhappy,” 65% of women with complications answered “no, not at all,” while among women without complications, this figure was only 21%, and the proportion of those who felt unhappy “quite often” was higher, at 32% (p=0.001).
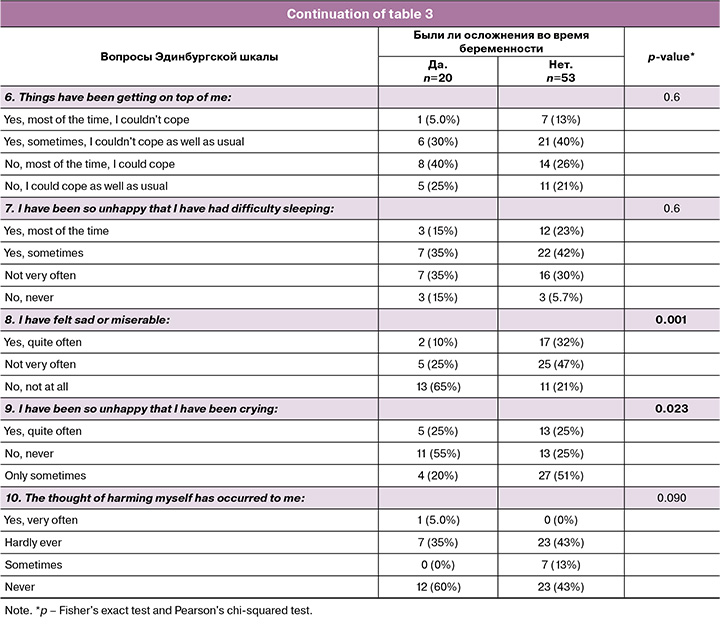
A similar trend was observed in response to the question “I was unhappy and cried often.” More than half of the women with complications (55%) reported that they had never experienced such a state, while among women without complications, this figure dropped to 25%. At the same time, the proportion of “only sometimes” responses was 51%, indicating more frequent episodes of tearfulness and emotional instability (p=0.023).
The severity of anxiety symptoms also differed between the groups. Among women without complications, the answers “yes, very often” to the question “I was anxious for no particular reason” (26% vs. 10%) and “I felt fear or panic without significant cause” (51% vs. 20%), reflecting increased anxiety in this group (p=0.035 and p=0.044, respectively).
Statistically significant differences were found in the total EPDS scores between groups with and without complications (p=0.012). The median EPDS score was lower in women who had complications. A moderate negative correlation was found between a woman's age and the total EPDS score (ρ=-0.42; p=0.0002) and between parity and EPDS scores (ρ=-0.43; p=0.0001), according to Spearman's correlation coefficient. Older age and higher parity were associated with lower severity of depressive symptoms.
Discussion
This study revealed that PPD symptoms are a significant issue for women of all age groups in Osh. More than half (57%) of the women surveyed experienced depressive symptoms during the postpartum period, indicating a high prevalence of this condition. The results demonstrate that young mothers (especially those under 25 years) are at a higher risk of developing depression than women in older age groups. While women over 35 also exhibited a tendency toward depressive states, the prevalence was lower than that in the younger groups. This analysis highlights the need to identify specific age groups for targeted support and preventive measures, which is consistent with Beck C.T. [10].
A comparative analysis showed that the severity of depressive symptoms in the postpartum period was significantly higher among women aged <25 years than among women aged 25–35 years and those aged >35 years. Younger mothers experienced the highest levels of emotional stress and depressive symptoms, particularly during the first weeks postpartum. Women of middle reproductive age (25–35 years) demonstrated lower levels of depressive symptoms, potentially indicating better psychological adaptation and resilience. Among women aged >35 years, depressive symptoms were less frequent but remained clinically significant, especially in the postpartum period. Thus, as reported by Alexander E.K. et al., maternal age influences the severity of depression, and younger age groups require additional attention and support during the postpartum period [14].
The study also showed that the level of depression was higher among primiparous women; 58% of primiparous women experienced symptoms of depression, which is higher than among multiparous women, among whom the risk of depression is somewhat lower, consistent with the findings of Li B. et al. [22]. A relationship was also identified between the time elapsed postpartum and the level of depression; the highest severity of depressive symptoms was observed during the first week (64%), followed by a gradual decrease (to 45% by the sixth week and 39% after the seventh week). This finding underscores the importance of early intervention, particularly for primiparous women, and the need to ensure sustained support throughout the postpartum period, consistent with Qi W. et al. [23].
Women with no complications during pregnancy experienced anxiety, feelings of unhappiness, and emotional fluctuations more frequently during the postpartum period. This may reflect lower psychological preparedness for stress or more pronounced postpartum emotional reactions. Conversely, women who experienced complications during pregnancy demonstrated greater emotional resilience and adaptation, potentially associated with previously developed psychological defense mechanisms and experience in overcoming difficulties. These results contradict the findings of Malgina G.B. et al. [24], which may be related to the small number of women with complications included in the study.
Conclusion
This study revealed a high prevalence of PPD symptoms (60%) in Osh women. The most vulnerable groups were young (18–25 years) and primiparous women who demonstrated significantly higher total EPDS scores and a higher frequency of pronounced depressive and anxiety symptoms. An inverse relationship was observed among age, parity, and symptom severity. These results indicate the importance of early PPD screening (especially during the first week postpartum) and strengthening psychological support for young and primiparous women.
References
- Эдельханова А.И., Зубков Д.В., Скворцова А.В., Нурмухамбетова А.Н., Шайзадина, А.А., Рымбек К.А. Связь между методом родоразрешения и послеродовой депрессией: обзор литературы. Репродуктивная медицина (Центральная Азия). 2024; 2: 88-94. [Edelkhanova A.I., Zubkov D.V., Skvortsova A.V., Nurmukhambetova A.N., Shaizadina A.A., Rymbek K.A. The connection between the method of delivery and postpartum depression: a literature review. Reproductive medicine (Central Asia). 2024; 2: 88-94 (in Russian)]. https://dx.doi.org/10.37800/RM.2.2024.88-94
- Ebina Y., Ito S., Yamaguchi T., Iwata H., Kishi R. Stability and variability of Edinburgh Postnatal Depression Scale networks among postpartum women: Insights from the Japan Environment and Children's Study. J. Affect. Disord. 2025; 391: 119992. https://dx.doi.org/10.1016/j.jad.2025.119992
- Gelaye B., Rondon M.B., Araya R., Williams M.A. Epidemiology of maternal depression, risk factors, and child outcomes in low-income and middle-income countries. Lancet Psychiatry. 2016. 3(10), 973-82. https://dx.doi.org/10.1016/S2215-0366(16)30284-X
- Sindalovsky A., Geisler K., Huddleston H. G., Cedars M. I., Jaswa E. G., Huddleston R. et al. The association between perinatal maternal mental health during the COVID-19 pandemic and offspring neurodevelopment at 24 months of age. J. Affect. Disord. 2025; 391: 119884. https://dx.doi.org/10.1016/j.jad.2025.119884
- Мазо Г.Э., Вассерман Л.И., Шаманина В.М. Выбор шкал для оценки послеродовой депрессии. Обозрение психиатрии и медицинской психологии. 2012; 2: 41-50. [Mazo G.E., Vasserman L.I., Shamanina V.M. Diagnostic methods for postpartum depression. Review of psychiatry and medical psychology. 2012; 2: 41-50 (in Russian)].
- Rodas N.V., Liu S.R., Chavira D.A., Godino J.G. Depression among Latina women in the United States from pregnancy to early postpartum: longitudinal examination of risk factors. BMC pregnancy and childbirth. 2025; 25(1): 501. https://dx.doi.org/10.1186/s12884-025-07548-6
- Татарова Н.А., Шаманина М.В., Сохадзе Х.С., Савина Л.В. Эндокринные факторы риска развития тревожно-депрессивных состояний у женщин в послеродовом периоде. Гинекология. 2013; 15(6): 74-8. [Tatarova N.A., Shamanina M.V., Sokhadze Kh.S., Savina L.V. Endocrine risk factors for the development of anxiety-depressive conditions in women in the postpartum period. Gynecology. 2013; 15(6): 74-8 (in Russian)].
- Abdieva N., Kosherbaeva L., Sagyndykova Z. Postpartum depression in Kazakhstan amid global data. Vestnik KazNMU №1. 2020; (1-1): 578-81.
- Carlson K., Mughal S., Azhar Y., Siddiqui W. Perinatal Depression. 2025 Jan 22. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan–. Available at: https://www.ncbi.nlm.nih.gov/books/NBK519070/
- Beck C.T. Predictors of postpartum depression: an update. Nurs. Res. 2001; 50(5): 275-85. https://dx.doi.org/10.1097/00006199-200109000-00004
- O'Hara M.W., McCabe J.E. Postpartum depression: current status and future directions. Annu. Rev. Clin. Psychol. 2013; 9: 379-407. https://dx.doi.org/10.1146/annurev-clinpsy-050212-185612
- Neupane S., Vuong A.M., Haboush-Deloye A., Mancha K., Buccini G. Association between postpartum anxiety and depression and exclusive and continued breastfeeding practices: a cross-sectional study in Nevada, USA. Int. Breastfeed. J. 2025; 20(1): 39. https://dx.doi.org/10.1186/s13006-025-00734-4
- Gebrekristos L.T., Ajayi A.I., Groves A.K., Kabiru C.W. Examining the associations between social support and postpartum depression symptoms among adolescent mothers in Nairobi, Kenya. Reprod. Health. 2025; 22(1): 11. https://dx.doi.org/10.1186/s12978-025-01943-0
- Alexander E.K., Pearce E.N., Brent G.A., Brown R.S., Chen H., Dosiou C. et al. 2017 Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and the postpartum. Thyroid. 2017; 27(3): 315-89. https://dx.doi.org/10.1089/thy.2016.0457
- Харченко А.А., Юрьева В.С., Якупова В.А., Суарэз А.Д. Психологическая и фармакологическая помощь при послеродовой депрессии и послеродовом ПТСР в России: социоэкономические факторы. Консультативная психология и психотерапия, 2024; 32(2): 9-30. [Kharchenko A.A., Yurieva V.S., Yakupova V.A., Suarez A.D. Psychological and pharmacological assistance for postpartum depression and postpartum PTSD in Russia: socioeconomic factors. Counseling psychology and psychotherapy. 2024; 32(2): 9-30 (in Russian)]. https://dx.doi.org/10.17759/cpp.2024320201
- Прибытков А.А. Психогенные послеродовые депрессии непсихотического уровня (клиническая картина и опыт терапии). Социальная и клиническая психиатрия. 2011; 21(1): 9-13. [Pribytkov A.A. Psychogenic postpartum non-psychotic depression (clinical picture and treatment experience). Social and clinical psychiatry. 2011; 21(1): 9-13 (in Russian)].
- Wang Y., Mao K., Deng J., Gu J. Comparison of symptoms of depression, anxiety, and stress in postpartum women with and without pain: a network analysis. BMC Pregnancy Childbirth. 2025; 25(1), 732. https://dx.doi.org/10.1186/s12884-025-07858-9
- Nakić Radoš S., Brekalo M., Matijaš M., Žutić M. Obsessive-compulsive disorder (OCD) symptoms during pregnancy and postpartum: prevalence, stability, predictors, and comorbidity with peripartum depression symptoms. BMC Pregnancy Childbirth. 2025; 25(1), 176. https://dx.doi.org/10.1186/s12884-025-07302-y
- Коргожа M.A., Евмененко A.O. Скрининговая шкала перинатальной тревоги (PASS-R). Краткое руководство по использованию. Методическое пособие. СПб.: СПбГПМУ; 2021. 20 с. [Korgozha M.A., Evmenenko A.O., eds. Screening scale of perinatal anxiety (PASS-R). A brief guide to use. Methodological guide. St. Petersburg: SPbSPMU; 2021. 20 p. (in Russian)].
- Gibson J., McKenzie-McHarg K., Shakespeare J., Price J., Gray R. A systematic review of studies validating the Edinburgh postnatal depression scale in antepartum and postpartum women. Acta Psychiatr. Scand. 2009; 119(5): 350-64. https://dx.doi.org/10.1111/j.1600-0447.2009.01363.x
- Реброва О.Ю. Статистический анализ медицинских данных. Применение пакета прикладных программ STATISTICA. М.: МедиаСфера; 2006. 305 c. [Rebrova O.Yu. Statistical analysis of medical data. Application of the STATISTICA application package. Moscow: MediaSfera; 2006. 305 p. (in Russian)].
- Li B., Liu T., Ma D., Sun J., Liu J. Association of fear of childbirth and postpartum depression with perceived partner response during pregnancy. BMC Pregnancy Childbirth. 2005; 25(1): 211. https://dx.doi.org/10.1186/s12884-025-07332-6
- Qi W., Wei Z., Lv H., Zhao J., Hu Y., Wang Y., Guo Q., Hu J. Postpartum depression and maternal-infant bonding: the mediating role of mentalizing and parenting self-efficacy. BMC Pregnancy Childbirth. 2025; 25(1): 667. https://dx.doi.org/10.1186/s12884-025-07762-2
- Мальгина Г.Б., Шафиева К.А., Шихова Е.П. Сверхранние преждевременные роды как предиктор послеродовой депрессии. Акушерство и гинекологии. 2017; 2: 39-44. [Malgina G.B., Shafieva K.A., Shikhova E.P. Very early premature birth as a predictor of postpartum depression. Obstetrics and Gynecology. 2017; (2): 39-44 (in Russian)]. https://dx.doi.org/10.18565/aig.2017.2.39-44
Received 25.08.2025
Accepted 12.02.2026
About the Authors
Guljamal A. Subanova, PhD, Associate Professor at the Department of Clinical Disciplines 2, International Medical Faculty, Osh State University, Kyrgyzstan, Osh city,Abiya Kabylova str., 215/2, bldg. 2, +996(772)23-05-19, gsubanova@oshsu.kg, https://orcid.org/0000-0003-1003-678X
Nargiza A. Subanova, Assistant at the Department of Obstetrics and Gynecology No. 2, Kyrgyz State Medical Academy named after I.K. Akhunbayev, 720020 Kyrgyzstan, Bishkek, Isa Akhunbayeva str., 92, 1st floor, +996(507)50-55-05, nargiza.subanova@bk.ru , https://orcid.org/0000-0003-1455-7902
Arsen A. Askerov, MD, Associate Professor, Head of the Department of Clinical Disciplines, Bishkek International Medical Institute, 720065, Kyrgyzstan, Bishkek,
Shabdan Baatyr Ave., 4a, +996(550)33-17-31, askerov.arsen@inbox.ru, https://orcid.org/0000-0003-4447-9650
Erzamat Y. Yrysbaev, Lecturer at the Department of General, Clinical Biochemistry and Pathophysiology, Faculty of Medicine, Osh State University, Kyrgyzstan, Osh city, Abiya Kabylova str., 215/2, bldg. 1, 996(706)82-03-50, yrysbaev@oshsu.kg, https://orcid.org/0000-0003-0476-2654
Aiperi Nurbek kyzy, Resident at the Center for Postgraduate and Continuous Medical Education, Osh State University, Kyrgyzstan, Osh city, Abiya Kabylova str., 215/2,
bldg. 2, +996(555)36-35-15, aiperinurbekova01@gmail.com, https://orcid.org/0009-0000-7707-6634
Azamat Y. Yrysbayev, Lecturer at the Department of Morphophysiologic Subjects, International European University, 720080, Kyrgyzstan, Bishkek, Muchtar Auezova str., 3, +996(704)24-52-96, yrysbaev1996@gmail.com , https://orcid.org/0009-0009-4978-994X
Gulkayir K. Muratova, PhD, Department of Obstetrics and Gynecology, Medical Education, Osh State University, Kyrgyzstan, Osh city, Abiya Kabylova str., 215/2, bldg. 2, +996(555)12-11-91, gulkayir78@gmail.com, https://orcid.org/0000-0002-2425-1854
Corresponding author: Erzamat Y. Yrysbaev, yrysbaev@oshsu.kg
Similar Articles

