
Characteristics of patinets with different outcomes of functional hypothalamic amenorrhea: long-term catamnestic follow-up data
Rakhmonova F.S., Ermakova D.M., Dolgushina N.V.
Functional hypothalamic amenorrhea (FHA) is a reversible disorder that causes menstrual irregularity due to energy deficiency as a result of excessive exercise, dietary restrictions, and stress. Despite extensive study of the pathogenesis of FHA, the data on the predictors and timing of restoration of menstrual cycle regularity remain limited. This necessitates an in-depth analysis of clinical and anamnestic characteristics of patients.
Objective: Based on analysis of long-lasting FHA to define particular characteristics of patients, who experienced or not experienced menstrual restoration.
Materials and methods: Analysis included the data of 431 patients with FHA aged 18–35 years, who underwent treatment at V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology from 2015 to 2025. The telephone survey was conducted at the end of 2025 and yielded responses from 123 women. Their data on the cause of the disease and treatment methods were stored in the data matrix. The final statistical sample included 94 patients with a follow-up period of more than one year.
Results: Long-term follow-up showed, that menstrual cycle was restored in most patients with FHA. However, 20% of women still experienced amenorrhea. Poor prognosis was associated with higher age and body mass index (BMI) at the onset of the disorder, as well as profound hypothalamic-pituitary-ovarian axis suppression according to the laboratory test results. Menstrual restoration happened most often in women with reduced BMI as the leading factor in the development of FHA, and with increased energy availability and reduced stress during treatment.
Conclusion: FHA is characterized by clinical heterogeneity. At the same time, restoration of spontaneous menstrual cycle is largely determined by correction of modifiable risk factors. Personalized approach to patient management is necessary taking into account a combination of anthropometric, clinical, anamnestic, and laboratory parameters.
Authors' contributions: Rakhmonova F.S. – analysis of literature data and primary medical documentation, preparation and performance of telephone survey; writing the manuscript; Ermakova D.M. – the study concept, analysis and data systematization of the primary medical documentation and patient feedback, manuscript editing; Dolgushina N.V. - the study concept and design, scientific consulting, analysis and data systematization of the primary medical documentation and patient feedback, critical review of the manuscript, approval of the final version of the manuscript.
Conflicts of interest: The authors confirm that they have no conflict of interest to declare.
Funding: The study was conducted within the framework of dissertation of Rakhmonova F.S. for the degree of candidate of medical sciences “Prediction of the severity of functional hypothalamic amenorrhea and the effectiveness of therapy based on analysis of serum autoantibodies of different specificities, tissue-specific and free mRNA"
Patient Consent for Publication: Before starting telephone survey, oral consent was obtained from patients to process their data for research purposes and publication on the condition of anonymity.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Rakhmonova F.S., Ermakova D.M., Dolgushina N.V. Characteristics of patinets with
different outcomes of functional hypothalamic amenorrhea: long-term catamnestic follow-up data.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (4): 114-120 (in Russian)
https://dx.doi.org/10.18565/aig.2026.100
Keywords
functional hypothalamic amenorrhea
stress
energy deficiency
excessive exercise
Functional hypothalamic amenorrhea (FHA) is one of the most common causes of secondary amenorrhea in women of reproductive age. It is a form of reversible hypogonadotropic hypogonadism that develops as a result of dysregulation in the hypothalamic-pituitary-ovarian axis due to energy deficiency, psychoemotional stress, excessive physical exercise, or a combination of these factors [1, 2]. Despite functional impairments, the clinical significance of FHA goes beyond menstrual dysfunction and anovulation, since prolonged hypoestrogenism is associated with reduced bone mineral density [3], metabolic changes [4], and negative pcycho-emotional outcomes [5].
Currently, FHA is considered to be a clinically heterogeneous condition that develops as a result of metabolic and stress effects with different degree of severity [6]. Even after elimination of these effects, duration of recovery of spontaneous menstruation varies, and recovery happens not in all patients [7]. This indicates the need for an in-depth exploration of the factors that determine the course of the disease and the prognosis for restoration of reproductive function.
Despite numerous data on the pathogenesis of FHA, there is limited information on long-term outcomes of the disease and the predictors of menstrual cycle restoration, especially in the studies with long-term follow-up [7]. Therefore, exploration of clinical, anamnestic, anthropometric and hormonal characteristics of patients with FHA depending on menstrual function recovery or non-recovery is undoubtedly of scientific and practical interest, since it can contribute to improvement of the prognostic approach and individualization of disease management strategies for this category of patients.
The aim of the study was to define particular characteristics of patients who experienced or not experienced menstrual restoration based on analysis of long-lasting FHA.
Materials and methods
Patient search and selection for this descriptive epidemiological study was done using electronic patient records in Medialog system of V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of Russia. The patients sought care in the Department of Gynecological Endocrinology from 2015 to 2025.
Inclusion criteria for women were the diagnosis of FHA confirmed by anamnestic data, the results of clinical, laboratory and instrumental tests, age from 18 to 35 years, and normal ovarian reserve (anti-Müllerian hormone (AMH) level >1,2 ng/mL, the number of antral follicles ≥5 in both ovaries). Non-inclusion criteria were oncological diseases, severe somatic pathology, central nervous system diseases, mental disorders, other types of amenorrhea and oligomenorrhea.
Patient database was compiled using Microsoft Excel. Electronic medical records of 431 women met eligibility criteria.
The specialized telephone interview script (protocol) was developed as a communication tool. To minimize bias and ensure compliance with ethical standards, the script underwent internal validation taking into account medical ethics principles and clinical guidelines for obstetrics and gynecology.
The telephone survey was conducted by trained medical personnel from November to December, 2025. Telephone calls were made from 10 a.m. to 7 p.m. With unanswered phone calls, at least two attempts of repeated calls were made on different days of the week. At the beginning of telephone conversation oral consent was obtained from patients to process their data for research purposes and publication on the condition of anonymity. Thus, the responses were obtained from 123 patients.
Real-time respondent’s answers were recorded. Microsoft Excel matrix was developed to formalize the data including the following variables: the causes of amenorrhea, weight changes (if any), restoration of the cycle using/not using medication (if drug therapy was used, the name of medication, dosage, and duration of administration were specified), referral to other specialists, and other established diagnoses.
Statistical analysis
After completion of data collection, the primary data were statistically analyzed using Statistica 10.0 software package. The continuous quantitative variables were described as the median (Me) and quartiles (Q1; Q3). The qualitative variables were described as absolute (n) and relative (%) frequencies. Patients who were followed-up for less than 1 year were excluded from the study. A total of 94 patients were included in the final analysis.
Results
Characteristics of patients included in the study
The first stage of analysis was assessment of clinical, anamnestic and laboratory data of all patients included in the study. The median overall duration of patient follow-up was 63.0 (44.0; 94.5) months.
The most common diseases among the participants of the study were digestive system diseases – 14/94 (14.9%), allergic diseases – 10/94 (10.6%), chronic autoimmune thyroiditis (8/94 (8.5%). In addition, 14/94 (14.9%) were smokers.
The median age at menarche was 13 (13.0) years. The median length of the menstrual cycle was 29.0 (29.0; 44.0) days, the duration of menstruation was 5 days.
Primary menstrual cycle disorders (oligo-/amenorrhea) were found in 7/94 7.4%) women, and secondary in 87/94 (92.6%). Polycystic ovarian syndrome (PCOS) was previously diagnosed in 16/94 (17.0%) women.
Coitarche before the onset of FHA was in 61/94 (64.9%) patients. Previous pregnancies were in 10/94 (10.6%) women and ended with livebirths in 9/94 (9,6%) women.
The median age of patients in the study at the onset of functional menstrual disorders was 24.0 (20.0; 28.3) years. Gynecologic age (GA), which is defined as age at getting passport minus age at menarche and according to the latest data associated with the risk of developing FHA [8] was 11.5 (7.0; 15.0) years.
The factors influencing the onset of FHA
At the onset of FHA, the median BMI was 18.6 (17,3; 19.9) kg/m2. At the same time, almost half of women included in the study (46/94 (48,9%) were underweight, and another half – 47/94 (50.0%) had normal BMI. Only one (1.1%) woman was overweight.
Among the respondents, 65/94 (69.1%) women experienced stress, 60/94 (63.8%) responded about dietary restrictions and adherence to a diet, and 40/94 (42,6%) reported vigorous physical activity. More than half of patients – 51/94 (54,3%) reported the presence of two or more risk factors.
At the onset of FHA, the median level of luteinizing hormone (LH) was decreased – 1.35 (0.5; 3.1) mIU/ml, follicle-stimulating hormone (FSH) level was 4.68 (3.2; 6.0) mIU/ml. Hypogonadotropic amenorrhea/oligomenorrhea was observed in 71/94 (75.5%) patients, and normogonadotropic amenorrhea/oligomenorrhea in 23/94 (24.5%) women. LH/FSH ratio <1 was observed in 86/94 (91.5%) patients, and the median ratio was 0.3 (0.2; 0.6). The median estradiol level was 43.5 (27.0; 99.0) pmol/L. Ovarian reserve was preserved in all patients (AMH level was 6.1 (3.9: 9.4) ng/mL).
Analysis of patient data depending on spontaneous menstruation recovery or non-recovery
By the time of conducting the telephone survey, recovery of menstrual cycle was in 75/94 (79.8%) patients, 19/94 (20.2%) reported absence of spontaneous menstruation. Based on these data the patients were divided into two groups – group 1 and group 2, respectively.
It is important to note that follow-up duration in patient with recovery and non-recovery of the menstrual cycle was comparable – 66.0 (48.0; 101.0) and 50.0 (36.0; 87.0) months, р=0.093 (Table).
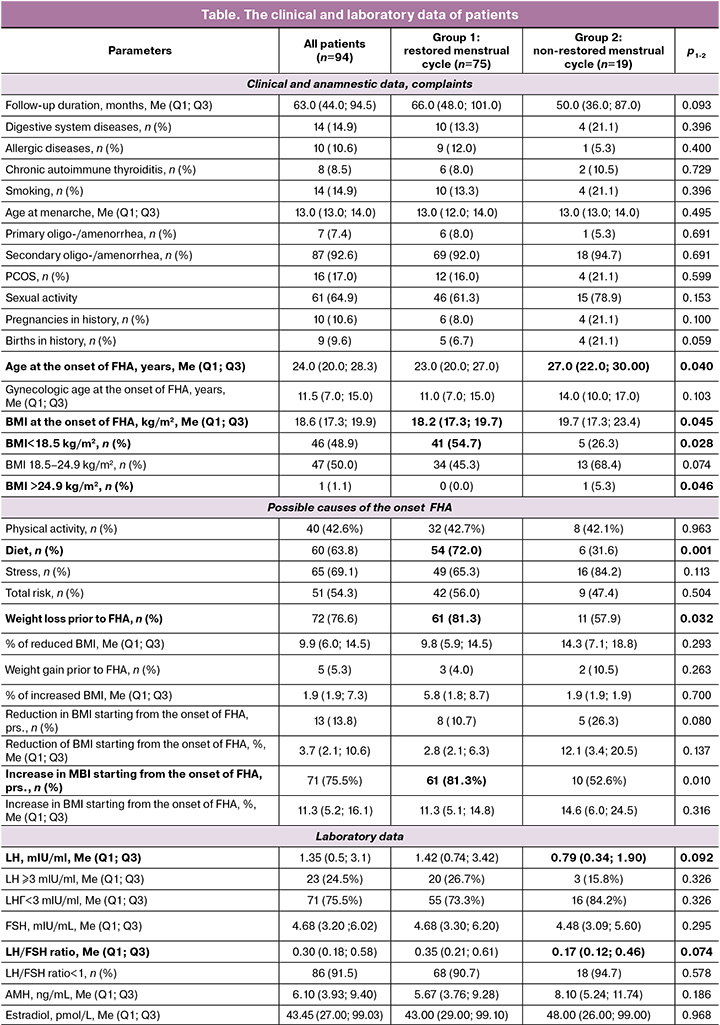
There were no differences in the incidence of somatic and gynecological diseases between the groups. Smoking was more common among women with the absence of spontaneous menstruation – 4/19 (21.1%) compared with 10/75 (13.3%) women with restored menstrual cycle. However, the differences were not statistically significant (р=0.396). Pregnancy rates and the number of births in history were also comparable between the groups (р=0.100 and р=0.059, respectively).
In women in group 2, FHA occurred at a later age compared with patients in group 1 – 27.0 (22.0; 30.0) and 23.0 (23.0; 28.3) years, respectively, p=0.40. Moreover, the trend toward higher gynecologic age was noted at the onset of FHA – 14.0 (10.0; 17.0) versus 11.0 (7.0; 15.0) years, respectively, р=0,103.
It is interesting to note that at the onset of FHA, the median BMI was higher in patients who did not experience restoration of their menstrual cycle rhythm – 19.7 (17.3; 23.4 kg/m2) compared with women with restored cycle – 18.2 (17.3; 19.7) kg/m2), р=0.045. Moreover, significantly higher number of women were underweight in group 1 – 41/75 (54.7%) compared with group 2 – 5/19 (26.3%), р=0.028. Also, the number of women who associated FHA with diet change was higher – 54/75 (72.0%) versus 6/19 (31.6%), respectively, р=0.001. This could be explained by the fact that weight loss before the onset of FHA was noted in a higher number of women in group 1 – 61/75 (81.3%) compared with group 2 – 11/19 (57.9%) (р=0.032). However, the trend toward greater reduction in BMI (%) was noted in those who did not experience subsequent restoration of their spontaneous menstrual rhythm – 14.3 (7.1; 18.8)% and 9.8 (5.9; 14,5)%, р=0.293.
Laboratory test results showed that with similar incidence of hypogonadotropic state in patients in both groups – 20/75 (26.7%) and 3/19 (15.8%), р=0.326), LH levels were lower in group 2 – 0.79 (0.3; 1.9) mIU/ml versus 1.42 (0.7; 3.4) mIU/ml, as well the LH/FSH ratio was lower – 0.2 (0.1; 0.5) versus 0.4 (0.2; 0.6). However, the differences did not reach statistical significance (р=0.092 and р=0.074, respectively). The results of AMH test used as a test for ovarian reserve were comparable in patients in both groups (р=0.186).
It is notable that estrogen levels in the blood of 14/94 (14.9%) smoking women were lower compared with 80/94 (85.1%) non-smokers – 32.0 (16,0; 35,0) pmol/L and 32.0 (16.0; 35.0) pmol/L, respectively, р=0.025. At the same time, gonadotropin levels were higher. LH levels – 2.5 (0.9; 4.9) mIU/ml in the group of smokers, and 1.3 (0.5; 2.3) mIU/ml in the group of non-smokers, р=0.054; FSH levels – 6,2 (4.1; 7.5) mIU/ml and 4.4 (3.2; 5.7) mIU/ml, respectively, p=0.017. Also, the trend toward lower prolactin levels were found in smokers – 112.6 (59.4; 180.0) mIU/ml versus 159.5 (119.5; 263.5) mIU/ml, р=0.059.
Recovery of menstrual cycle in 40/75 (53.3%) women was associated with eating energy-boosting foods, in 16/75 (21.3%) with lower intensity of physical activity, and 27/75 (36.0%) with reduced impact of external stressors. Drug therapy was required in 59/75 (78.7%) patients. At the same time, weight loss after the onset of FHA was observed in 8/75 (10.7%) women, and was less common compared with patients who did not experience recovery of their menstrual cycle – 5/19 (26.3%), р=0.080. The percentage of reduced BMI among women in group 1 was also lower compared with group 2 – 2.8 (2.1; 6.3)% versus 12.1 (3.4; 20.5)%, р=0.137). The women who experienced restoration of their spontaneous menstrual rhythm were characterized by increased body weight more often – (61/75 (81.3%) versus 10/19 (52.6%), р=0.010.
Discussion
The obtained results showed that restoration of spontaneous menstrual cycle happened in the majority of patients with FHA during many years of follow-up. However, every 1 in 5 women had amenorrhea. At the same time, the patients with unfavorable treatment outcome were characterized by higher age at the onset of FHA, higher BMI in the occurrence of the disease, as well as the tendencies towards lower LH levels and LH/FSH ratio. On the contrary, the women with restored menstrual cycle were most often underweight at the onset of the disease. FHA was associated with diet change, and subsequent weight gain was observed in these women. In addition, recovery of menstruation was most often associated with eating energy-boosting foods and reduction of stress.
The obtained data are generally consistent with modern concepts of FHA as a multifactorial functional disorder, which develops against the backdrop of energy deficiency, psycho-emotional stress, excessive physical exercise, or a combination of these factors [6]. The fact that most patients in the study indicated not only one, but a combination of potential triggers of the disease, additionally confirms the heterogeneity of FHA.
It is important to note that the age of patients who did not experience subsequent restoration of their menstrual cycle was higher at the onset of FHA, and BMI was also higher. At first glance, these findings seem to be paradoxical, but factually they are consistent with the modern concept that energy availability assessed in dynamics, but not absolute body weight, plays a key role in regulation of the hypothalamic-pituitary-ovarian axis. Furthermore, in women of higher ager (including gynecologic age), functional amenorrhea manifests itself as a result of long-term and intensive exposure to stress [8].
The trend toward lower LH levels and LH/FSH ratio in patients without restored menstrual rhythm seems to be pathophysiologically justified. It is known that FHA is accompanied by decreased hypothalamic gonadotropin-releasing hormone secretion and subsequent suppression of pituitary-gonadal function [1]. The results obtained in our study confirm the findings in the study by Boegl М. et al. (2024), who reported that LH/FSH ratio ≤1 is specific for most patients with FHA [9]. It is conceivable that less favorable prognosis for spontaneous restoration of menstrual function is associated with greater inhibition of the hypothalamic-pituitary-ovarian axis manifested by significantly low LH level and LH/FSH ratio. At the same time, AMH levels in the groups were comparable, that consistently confirms preservation of ovarian reserve and functional rather than organic nature of the disorder [10].
The prevalence of smoking among the patients included in the study (14.9%) was comparable to that among women in high-income countries according to the WHO report on tobacco use for 2024 (14.6%) [11]. However, it exceeds the average percentage of smoking women in Russia according to the Federal State Statistics Service (8%) [12]. According to the data in scientific publications, active and passive smoking significantly affects human endocrine system, that is manifested by changes in the levels of sex hormones, as well as orexigenic and anorexigenic peptides [13]. Taking into account smoking (lower levels of estrogens and prolactin, higher levels of FSH), the differences in the hormonal profile in patients in our study are consistent with the existing data on the effect of chronic exposure to nicotine on the female reproductive system [13], and indicates the potential pathogenetic role of metabolic factors associated with smoking in regulation of the hypothalamic-pituitary-ovarian axis.
From the clinical standpoint, the results of this study confirm that recovery of menstrual cycle in FHA is largely associated with correction of modifiable risk factors – increasing energy availability, reducing physical activity and exposure to external stressors. This is consistent with current data according to which non-pharmacological interventions aimed at normalizing eating behavior, reducing energy deficiency, and psychotherapeutic interventions form the basic principles in management of FHA in patients [14]. It is important to note that recovery of the menstrual cycle does not always mean appropriate restoration of ovarian steroidogenesis and ovulatory function, that emphasizes the importance of long-term dynamic monitoring of patients’ condition [8].
Conclusion
Thus, the course of FHA is characterized by clinical heterogeneity. Recovery of spontaneous menstrual cycle is primarily associated with correction of modifiable risk factors. Higher age at the onset of FHA, higher BMI at the onset of the disease and the trend toward greater reduction in LH level and LH/FSH ratio can be considered as the signs of less favorable prognosis. The data obtained in our study indicate the need for personalized approach to management of patients with FHA taking into account a combination of anthropometric, clinical, anamnestic, and laboratory parameters.
Limitations of the study. Limitations of this study include the design (this is a descriptive epidemiological study), relatively small sample size, and the use of the telephone survey as a tool for collection of catamnestic data. At the same time, long-term follow-up period and analysis of clinically significant factors make it possible to consider the obtained data as an important grounding for subsequent prospective studies aimed at development of prognostic models for the course of FHA.
References
- Roberts R.E., Farahani L., Webber L., Jayasena C. Current understanding of hypothalamic amenorrhoea. Ther. Adv. Endocrinol. Metab. 2020; 11: 2042018820945854. https://dx.doi.org/10.1177/2042018820945854
- Ермакова Д.М., Рахмонова Ф.С., Долгушина Н.В. Функциональная гипоталамическая аменорея: этиология и патогенез, роль генетических факторов. Акушерство и гинекология. 2025; 11: 53-61. [Ermakova D.M., Rakhmonova F.S., Dolgushina N.V. Functional hypothalamic amenorrhea: etiology and pathogenesis, the role of genetic factors.. Obstetrics and Gynecology. 2025; (11): 53-61 (in Russian)]. https://dx.doi.org/10.18565/aig.2025.284
- Behary P., Comninos A.N. Bone perspectives in functional hypothalamic amenorrhoea: an update and future avenues. Front. Endocrinol. (Lausanne). 2022; 13: 923791. https://dx.doi.org/10.3389/fendo.2022.923791
- Meczekalski B., Katulski K., Czyzyk A., Podfigurna-Stopa A., Maciejewska-Jeske M. Functional hypothalamic amenorrhea and its influence on women’s health. J. Endocrinol. Invest. 2014; 37(11): 1049-56. https://dx.doi.org/10.1007/s40618-014-0169-3
- Bonazza F., Politi G., Leone D., Vegni E., Borghi L. Psychological factors in functional hypothalamic amenorrhea: a systematic review and meta-analysis. Front. Endocrinol. (Lausanne). 2023; 14: 981491. https://dx.doi.org/10.3389/fendo.2023.981491
- Morrison A.E., Fleming S., Levy M.J. A review of the pathophysiology of functional hypothalamic amenorrhoea in women subject to psychological stress, disordered eating, excessive exercise or a combination of these factors. Clin. Endocrinol. (Oxf). 2021; 95(2): 229-38. https://dx.doi.org/10.1111/cen.14399
- Pape J., Herbison A.E., Leeners B. Recovery of menses after functional hypothalamic amenorrhoea: if, when and why. Hum. Reprod. Update. 2021; 27(1): 130-53. https://dx.doi.org/10.1093/humupd/dmaa032
- De Souza M.J., Williams N.I., Misra M., Nattiv A., Joy E., Barrack M. et al. Update to the female athlete Triad coalition consensus statement Part 1: state of the science and introduction of a new adolescent model. Sports Med. 2026; 56(2): 327-73. https://dx.doi.org/10.1007/s40279-025-02333-z
- Boegl M., Dewailly D., Marculescu R., Steininger J., Ott J., Hager M. The LH:FSH ratio in functional hypothalamic amenorrhea: an observational study. J. Clin. Med. 2024; 13(5): 1201. https://dx.doi.org/10.3390/jcm13051201
- Practice Committee of the American Society for Reproductive Medicine. Current evaluation of amenorrhea: a committee opinion. Fertil. Steril. 2024; 122(1): 52-61. https://dx.doi.org/10.1016/j.fertnstert.2024.02.001
- World Health Organization. WHO global report on trends in prevalence of tobacco use 2000–2024 and projections 2025–2030. Available at: https://www.who.int/publications/i/item/9789240116276
- Федеральная служба государственной статистики. Федеральные статистические наблюдения по социально-демографическим проблемам. Доступно по: https://rosstat.gov.ru/itog_inspect [Federal State Statistics Service. Federal statistical observations on socio-demographic issues. Available at: https://rosstat.gov.ru/itog_inspect (in Russian)].
- Tweed J.O., Hsia S.H., Lutfy K., Friedman T.C. The endocrine effects of nicotine and cigarette smoke. Trends Endocrinol. Metab. 2012; 23(7): 334-42. https://dx.doi.org/10.1016/j.tem.2012.03.006
- Министерство здравоохранения Российской Федерации. Клинические рекомендации. Аменорея и олигоменорея. 2024. [Ministry of Health of the Russian Federation. Clinical guidelines. Amenorrhea and oligomenorrhea. 2024 (in Russian)].
Received 25.03.2026
Accepted 03.04.2026
About the Authors
Farzona S. Rakhmonova, PhD student, obstetrician-gynecologist, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of the Russian Federation, 117997, Russia, Moscow, Ac. Oparina str., 4, f_rakhmonova@oparina4.ru, https://orcid.org/0009-0000-6615-9426Daria M. Ermakova, PhD, Senior Researcher, obstetrician-gynecologist, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of the Russian Federation, 117997, Russia, Moscow, Ac. Oparina str., 4, d_ermakova@oparina4.ru, https://orcid.org/0000-0002-8558-4687
Nataliya V. Dolgushina, Dr. Med. Sci., Professor, Deputy Director for Research, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of the Russian Federation, 117997, Russia, Moscow, Ac. Oparina str., 4, n_dolgushina@oparina4.ru, https://orcid.org/0000-0003-1116-138X
Corresponding author: Farzona S. Rakhmonova, f_rakhmonova@oparina4.ru
Similar Articles

