
Psychoemotional state of women undergoing in vitro fertilization treatment
Yasnaya D.V., Likhacheva V.V., Proskuryakova L.A., Alontseva V.V., Azarova O.V.
Background: A combination of factors causing infertility and consisting of somatic, mental and social determinants of health, requires a comprehensive study of strategies to improve the effectiveness of assisted reproductive technologies (ART). At the same time, exploration of the psychoemotional state of patients undergoing ART treatment, requires both psychophysiological and psychodiagnostic research methods to obtain more objective data.
Objective: To explore specific characteristics of the psychoemotional state of women undergoing in vitro fertilization (IVF) treatment.
Materials and methods: The psycho-emotional state of women was assessed using psychophysiological methods (electroencephalography (EEG) analysis), psychodiagnostic methods: Psychological Stress Measure (PSM-25) (R. Tessier, L. Lemyre, L. Fillion, adapted by N.E. Vodopyanova) and Anxiety and Depression Questionnaire – a shortened version of the Clinical Questionnaire for Identification and Assessment of Neurotic States (K.K. Yakhin, D.M. Mendelevich), as well as statistical methods.
Results: Data analysis found statistically significant differences in the properties of EEG alpha rhythm frequency, as well as in manifestation of irritative changes — diffuse asynchronous beta activity in the group of women undergoing repeated IVF cycles. Nonconforming data were also found between objective (EEG) and subjective (psychodiagnostic methods) assessment of the psychoemotional state of women undergoing repeated IVF treatment. Objective assessment showed that regardless of the number of IVF attempts, the signs of stress were present in women in both groups and became more intense with repeated IFV failures. According to subjective assessment, women in both groups did not report experiencing stress, anxiety, or depression, even after failed IVF attempts.
Conclusion: The obtained data indicate the necessity to use objective methods, such as EEG analysis for assessment of the psychoemotional state in women undergoing IVF treatment for infertility. This approach will allow timely correction of the identified impairments, improved adherence of infertile patients to continue treatment, and will improve the effectiveness of ART programs.
Authors' contributions: Yasnaya D.V., Likhacheva V.V., Proskuryakova L.A., Alontseva V.V., Azarova O.V. – the concept and design of the study, obtaining data for analysis, literature review, material processing and analysis on the topic of the article, manuscript writing and editing.
Conflicts of interest: The authors confirm that they have no conflict of interest to declare.
Funding: The study was carried out without any sponsorship.
Acknowledgment: The authors express their deep gratitude to I.D. Martynov, Ph.D., for EEG interpretation.
Ethical Approval: The study was approved by the local Ethics Committee of Novokuznetsk State Institute of Postgraduate Medical Education – a branch of the Russian Medical Academy of Continuous Professional Education of the Ministry of Health of Russia/Kuzbass Humanitarian and Pedagogical Institute of Kemerovo State University
Patient Consent for Publication: The patients have signed informed consent for publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Yasnaya D.V., Likhacheva V.V., Proskuryakova L.A., Alontseva V.V., Azarova O.V.
Psychoemotional state of women undergoing in vitro fertilization treatment.
Akusherstvo i Gynekologiya/Obstetrics and Gynecology. 2025; (3): 136-143 (in Russian)
https://dx.doi.org/10.18565/aig.2024.310
Keywords
infertility
in vitro fertilization (IVF)
electroencephalography
stress
anxiety
depression
IVF failure
beta rhythm
Infertility is defined as inability of married couples, who want to have children, to achieve pregnancy after one year of regular unprotected sexual intercourse [1], and remains a serious challenge in reproductive medicine. Assisted reproductive technologies (ART), in particular in vitro fertilization (IVF), through intervention targeted toward the etiological factors of infertility, demonstrate the success rate of 20–35% per cycle, that exceeds the rate of spontaneous conception in the population of healthy young people [2].
Infertility has a significant impact on quality of life, adversely affecting psychosocial well-being and increasing susceptibility to stress and psycho-emotional stress. Research data show that due to increased stress and emotional burden, about 23% of couples discontinue IVF treatments prematurely [3].
It was also found that depression, personal and situational anxiety can affect the outcome of treatment: in women, who had a favorable treatment outcome, depression and anxiety levels were low [4, 5]. Other researchers also report that the factors, such as duration of infertility, drug therapy, and multiple unsuccessful attempts to conceive are associated with high levels of anxiety, depression and stress in women [6]. However, the psychodiagnostic tools are far from perfect, as they measure the subjective perception of respondents’ experience, and thereby can be exposed to distortion [7], that leads to contradictory data. Some researchers note that there is no relationship between stress, other psycho-emotional states and the causes of infertility, and the effectiveness of ART methods [8, 9]. There is an obvious need for objective diagnostics, where the use of electroencephalography (EEG) seems to be promising. EEG is a tool to record postsynaptic potentials of the brain especially in the neocortex, and is a non-invasive method providing a precise measure of brain function. The studies on psycho-emotional states using EEG reported that EEG activity correlates with mental stress in terms of decreased electroencephalographic alpha power, increased beta power, and increased interhemispheric asymmetry [10, 11]. Comparative analysis of bioelectrical brain activity in women preparing for IVF and in women of reproductive age who did not need IVF treatment found statistically significant differences indicating the presence of stress reaction in the first group of women [12].
Consequently, the purpose of the study was to explore specific characteristics of the psycho-emotional state of women undergoing in vitro fertilization (IVF) treatment.
Materials and methods
A comparative cross-sectional study was conducted involving two groups of patients undergoing IVF treatment for infertility. The psycho-emotional state of women was assessed using the objective (electroencephalography (EEG)) and subjective (psychodiagnostic methods). The study was conducted before starting IVF cycle. The study sample included 2 groups. Group 1 consisted of women undergoing the first IVF cycle (n=35), and group 2 consisted of women undergoing the repeated IVF cycle (n=23). Inclusion criteria were women of reproductive age with the diagnosis of infertility, the use of IVF as a method of ART for infertility treatment. Exclusion criteria were contraindications to IVF (according to the Order No. 803n of the Ministry of Health of Russia of July 31, 2020) [13], the use of other ART techniques. The groups were formed based on failed IVF attempts in history (the group with the first IVF protocol and without previous IVF attempts, the group with the repeated IVF protocol and with previous IVF attempts.
The study was conducted in the following institutions in Novokuznetsk: Novokuznetsk State Institute of Postgraduate Medical Education – a branch of the Russian Medical Academy of Continuous Professional Education of the Ministry of Health of Russia, the Department of Obstetrics and Gynecology; Family Clinic “Expert” and Kuzbass Humanitarian and Pedagogical Institute of Kemerovo State University, the Department of Psychology and General Pedagogics.
The study sample comprised of 58 female patients, who were the residents of Kemerovo region – Kuzbass for more than 3 years. The mean age of women was 34.2±4.64 years. The voluntary informed consent to participate in the study was obtained from each woman.
At the first stage, treatment characteristics for patients undergoing IVF were specified: the first cycle (no patient experience in IVF treatment) or the repeated cycles (failed IVF attempts). According to the obtained results, the entire sample was divided into 2 groups. The number of women the undergoing IVF treatment program for the first time was 35. The mean age was 33.2±4.65 years, the average number of IVF cycles was 0. The group with repeated IVF treatment consisted of 23 women. The mean age was 35.82±4.25 years, the average number of IVF cycles was 2.48. The groups were comparable in age; no statistically significant differences were found between the groups.
At the second stage, neurophysiological tests with the use of EEG were performed for the objective diagnosis of psycho-emotional states. Automated test equipment produced by ATES MEDICA Device (Italy) was used in accordance with the International 10–20 system for EEG electrode placement (the monopolar montage, reference electrode Cz). The background EEG recording was taken (3 minutes, eyes closed), consisting of eyes open, photic stimulation, and hyperventilation stages. EEG analysis included evaluation of the frequency and amplitude characteristics, detection of paroxysmal activity and assessment of EEG symmetry. The frequency ranges of EEG signals were the following: alpha rhythm (8–13 Hz, up to 100 μV), beta rhythm (14–30 Hz, 5–30 μV), theta rhythm (4–16 Hz) and delta rhythm (0.5–3 Hz) [14]. Low amplitude and desynchronization of beta activity and smooth topographical differences, which were interpreted as a neurotic pattern of tension [15], were considered by us as an indicator of stress, reflecting predominance of ascending activation over inhibitory effects.
At the third stage, the diagnosis of neurotic conditions was made using psychodiagnostic methods – Psychological Stress Measure (РSМ-25) questionnaire (R. Tessier, L. Lemyre, L. Fillion, adapted by N.E. Vodopyanova) with the subsequent interpretation of the common indicator of psychological stress, and abridged version of the Clinical Questionnaire for Identification and Assessment of Neurotic Disorders (K.K. Yakhin, D.M. Mendelevich), known as Anxiety and Depression Questionnaire (ADQ), which had only two measurement scales, and the scores were interpreted in accordance with normal health parameters.
Statistical analysis
Statistical data processing included the following steps and methods. The Kolmogorov–Smirnov test was used to test for normality of distribution of the quantitative data. When the normal distribution was detected, the data were described as mean values (M) and standard deviation (SD), and otherwise were described as median (Me) and interquartile range (Q1; Q3). Absolute and relative (%) frequencies were calculated for qualitative data. The quantitative variables of independent samples were compared using the Student t-test (for normal distribution) or the Mann–Whitney U-test (for non-normal distribution). Fisher’s exact test or Pearson’s chi-squared (χ2) test was used for qualitative nominal variables. To estimate the influence of multiple factors, two types of regression analysis – multiple linear regression (for metric dependent variables) and logistic regression (for categorical (binary) dependent variables) were used. The differences and results of regression analysis were considered statistically significant at p<0.05.
Results
The data of 58 patients enrolled in the study were analyzed in accordance with the general inclusion/exclusion criteria. The group of women with the first IVF cycle (n=35) was characterized by the absence of previous IVF attempts; the presence of the following concomitant diseases: chronic adnexitis (28/35 (62%)), endometritis (28/35 (62%)), polycystic ovary syndrome (10/35 (29%)), uterine fibroids (9/35 (24%)) and ectopic pregnancy in history (7/35 (20%)); absence of mental or behavioral disorders. The group of women with the repeated IVF cycle (n 23) was characterized as follows: the average number of previous IVF attempts – 2.48±1.9; the presence of the following concomitant diseases, such as chronic adnexitis (13/23 (56%)), endometritis (13/23 (56%)), multiple IVF failures (8/23 (38%), polycystic ovary syndrome (5/23 (22%)) and ectopic pregnancy in history (4/23 (17%)); absence of mental or behavioral disorders (Table 1).
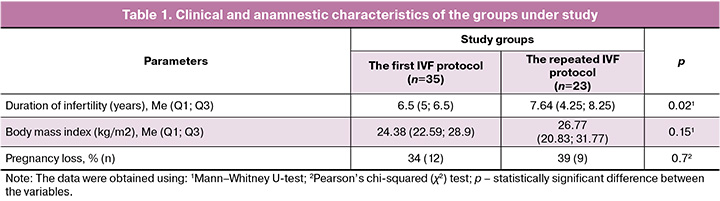
Statistical data analysis found no significant differences between the groups in the incidence of concomitant diseases: chronic adnexitis (p=0.05) and endometritis (p=0.05), polycystic ovary syndrome (p=0.56), ectopic pregnancy (p=0.8) and pregnancy loss (p=0.7) in history. The group with the first IVF attempt was characterized by higher incidence of uterine fibroids (p=0.02) compared with the group with repeated IVF. Body mass index in both groups conformed to the borderline level between normal and overweight (pre-obesity). There were no significant differences in BMI between the groups. Statistically significant differences were found in duration of infertility. It was greater in women with the repeated IVF protocol (p=0.02). EEG analysis found that modulated alpha rhythm dominated in the occipital areas, and there was no paroxysmal activity in women undergoing IVF treatment (the first and repeated cycles). There were no significant differences in EEG amplitude characteristics found between the groups. However, statistically significant differences were found in the frequency of alpha rhythm and severity of irritative changes (diffuse asynchronous beta activity), that is represented in Table 2.

The parameters of the brain’s bioelectrical activity in both groups conformed to age norms and did not reflect pathological manifestations. However, higher frequency of alpha rhythm and severity of the disorganized basic EEG rhythm (diffuse asynchronous beta activity) was observed in the group with the repeated IVF protocol compared with the group with the first IVF protocol. High frequency of irritative changes in the group with the first IVF cycle (28/35 (81%)) and in the group with the repeated IVF cycle (23/23 (100%)) indicate a common EEG neurotic pattern of overwrought type specific for the patients undergoing ART.
Although the frequency of alpha rhythm remained within the age norm, the obtained data may indicate a tendency for replacement of alpha activity by faster beta activity associated with stress [10]. Potential confounding factors that could explain the observed differences were controlled by comparisons between the groups, such as no statistically significant differences in age, comorbidities (in manifestation of endocrine and metabolic disorders, absence of mental disorders, behavioral disorders and their pharmacological treatment), body mass index (indirectly affecting the hormonal background), the time of performing EEG (before starting IVF cycle and in the morning). At the same time, we did not control the phase of the menstrual cycle at the time of performing EEG, that could also affect the frequency and amplitude of alpha rhythm and explain the observed differences.
Stress in patients undergoing IVF was detected using psychophysiological diagnostics, and can be both as a result of unsuccessful IVF treatment for infertility and preceding factors that had negative effect on reproductive health [16]. Regression analysis was used to assess multiple factors (duration of infertility, the number of failed IVF, pregnancy losses in history) influencing psycho-emotional state of patients, which was assessed using psychophysiological methods, and the difference in their psycho-emotional state. Statistically insignificant results were obtained using multiple regression model (p=0.89) and logistic regression model (p=0.08). It is likely that the detected psycho-emotional states are caused by other factors, which are not directly related to reproductive function and require further research, in particular, the assumption that women may initially be more prone to neurotic behavior, and IVF failures and the problems associated with infertility may only aggravate the existing state.
Evaluation of the levels of psychological stress and neurotic states in the groups of women under study showed no significant differences both in women with the first IVF attempt and in women with repeated IVF cycles. The results are represented in Table 3.
The common indicator of mental stress in both groups conformed to psychological adaptation. The average score of anxiety and neurotic depression in both groups conformed to the level of health. Regardless of the number of IVF attempts, stress severity did not change. The obtained data can be associated with social support, financial situation, thereby the overall well-being is assessed as high, allowing to feel protected from social stressors [17]. Given the above represented data, which were obtained during the psychophysiological assessment, we cannot exclude that the explanation for the obtained results could be psychological defense mechanisms (repression, denial, etc.) and avoidance coping strategies, when women avoid stressful experience by conscious suppression of unwanted thoughts, as well as specific properties of self-report questionnaires, consisting of subjective assessment and depending on the ability for self-observation and reflection, and disposition to social desirability distortion.
Regression analysis for assessment of multiple factors – the number of failed IVF, pregnancy losses, duration of infertility influencing psycho-emotional state of women that was assessed using psychophysiological methods, showed insignificant results when estimating multiple regression models for the parameters “Stress” (p=0.08) and “Neurotic depression” (p=0.25), and significant results when estimating regression model for the parameter “Anxiety” (p=0.02). The factors that were used in the model contributed to 11% of the variance in anxiety. At the same time, IVF failures (p=0.94) and duration of infertility (p=0.17) had no statistically significant effect on anxiety. Pregnancy loss in history had statistically significant effect on anxiety (p=0.008). With an increase in the number of pregnancy losses by 1 loss, the anxiety score increases by 0.55 points, provided that all other variables remain constant. It is quite probable that the emotional experience associated with pregnancy loss may be more intense due to experiencing pregnancy loss. Therefore, it is taken into account in woman’s subjective assessment of her condition, while the experience of disappointment and frustration caused by unmet expectations due to failed IVF and long-term infertility can be subjectively assessed as an insignificant change, and therefore is not reflected when filling out questionnaires.
Discussion
Our study detected the signs of stress state according to the results of psychophysiological diagnostics in patients in both groups. These signs manifest themselves more often in the group with the repeated IVF cycle. However, subjective assessment of the psycho-emotional state using psychodiagnostic methods found no the signs of stress, anxiety or depression even with failed IVF in history and the need for repeated treatment.
EEG results (irritative changes and a tendency toward increased frequency of alpha rhythm in women with repeated IVF cycles) are consistent with the data on psychophysiological characteristics of patients undergoing IVF treatment. Previously it has been shown that in women planning to go through IVF for infertility, there is a tendency toward replacement of alpha activity by faster beta activity, that is interpreted as emotional stress [18].
Based on the data, which were obtained from one sample, the use of psychophysiological methods and the psychodiagnostic tools for assessment of psycho-emotional state in our study made it possible to detect inconsistency not with other studies, but with the results obtained from the respondents, and to interpret them. It is likely that the use of self-report questionnaires suggesting a subjective assessment of individuals’ condition can be influenced by social desirability in their answers, and is associated with insufficient skills of introspection and reflection, as well as the effect of psychological defense mechanisms and avoidance coping strategies. This is consistent with the findings of a systematic review reporting that distress associated with the use ART is associated with avoidance coping strategies [19].
Subjectively, the women with EEG neurotic pattern of overwrought type may perceive the signs of psycho-emotional stress (excitability, emotional dysregulation, irritability, sleep disturbance) as normal and not requiring correction. Moreover, lack of subjective awareness of stress at the somatic, emotional and behavioral levels can be due to individual properties of the emotion regulation. This neurotic pattern, among other things, is characterized by an imbalance in favor of activating influence, which is subjectively experienced as psycho-emotional tension without the severity of anxiety symptoms [16]. Thus, the state of anxiety can be less inherent in this sample.
The data obtained in both groups of women indicate that lack of subjective experience of psycho-emotional states, such as stress, anxiety, depression, and detection of the signs of these states based on the results of a psychophysiological assessment, are inherent in respondents in this sample, regardless of the number of IVF attempts. This, in turn, can influence the course of treatment. Due to increased excitability and subconscious psycho-emotional stress, medical procedures can be perceived with impatience, that increases the risk of impulsive behavior, while the degree of adherence to treatment after failed IVF attempts or when facing problems during IVF treatment can be reduced. Also, suppression of the signs of stress at a conscious level can cause difficulties for women to seeking timely help from relatives and close people, and professional medical help, that can worsen their psycho-emotional state.
Conclusion
This article represents the results of the study of the psycho-emotional states of women undergoing the first and repeated cycles of IVF treatment. The signs of psycho-emotional stress recorded by EEG, which occur more often in the group of patients with failed IVF attempts, are inherent in both groups. At the same time, the results of psychophysiological diagnostics did not reflect the patients’ subjective assessment of their psycho-emotional state when using psychodiagnostic methods. The findings in the study cannot be explained exclusively by the factors directly related to reproductive function, and require additional research on the initial tendency of patients toward neurotic and stress reactions, and strategies for perception and stress management.
References
- Adamsom G.D., de Mouzon J., Chambers G.M., Zegers-Hochschild F. International Committee for Monitoring Assisted Reproductive Technology: world report on assisted reproductive technology, 2011. Fertil. Steril. 2018; 110(6): 1067-80. https://dx.doi.org/10.1016/j.fertnstert.2018.06.039.
- Бирюкова А.М., Мартиросян Я.О., Ковальчик А.И., Хубаева Д.Г. Диагностика и лечение бесплодия. Клиническая лекция. Медицинский оппонент. 2021; 2(14): 41-5. [Birukova A.M., Martirosyan Ya.O., Kovalchuk A.I., Khubaeva D.G. Infertility diagnosis and treatment. Clinical lecture. Medical Opponent. 2021; 2(14): 41-5. (in Russian)].
- Паскарь С.С., Калугина А.С., Ткачук А.Г. Оценка удовлетворенности качеством лечения пациенток с бесплодием с помощью вспомогательных репродуктивных технологий. Российский вестник акушера-гинеколога. 2019; 19(5): 77-82. [Paskar S.S., Kalugina A.S., Tkachuk A.G. Evaluating patient satisfaction regarding assisted reproductive technologies. Russian Bulletin of Obstetrician-Gynecologist. 2019; 19(5): 77 82. (in Russian)]. https://dx.doi.org/10.17116/rosakush20191905177.
- Purewal S., Chapman S.C.E., van den Akker O.B.A. A systematic review and meta‐analysis of psychological predictors of successful assisted reproductive technologies. BMC Res. Notes. 2017; 10(1): 711. https://dx.doi.org/10.1186/s13104-017- 3049-z.
- Purewal S., Chapman S.C.E, van den Akker O.B.A. Depression, anxiety and lifestyle factors and outcomes from IVF. Reproductive Biomed. Online. 2018; 36(6): 646-57. https://dx.doi.org/10.1016/j.rbmo.2018.03.010.
- Maroufizadeh S., Navid B., Omani-Samani R., Amini P. The effects of depression, anxiety and stress symptoms on the clinical pregnancy rate in women undergoing IVF treatment. BMC Res. Notes. 2019; 12(1): 256. https://dx.doi.org/10.1186/s13104-019-4294-0.
- Филиппова Г.Г. Психологические аспекты вспомогательных репродуктивных технологий: обзор зарубежных и Российских исследований. Современная зарубежная психология. 2022; 11(1): 26-38. [Filippova G.G. Psychological aspects of assisted reproductive technologies: a review of foreign and Russian studies. Modern Foreign Psychology. 2022; 11(1): 26-38. (in Russian)]. https://dx.doi.org/10.17759/jmfp.2022110103.
- Tuncay G., Yıldız S., Karaer A., Reyhani I., Özgöcer T., Ucar C. et al. Stress in couples undergoing assisted reproductive technology. Arch. Gynecol. Obstet. 2020; 301(6):1561-7. https://dx.doi.org/10.1007/s00404-020-05549-8.
- Rooney K., Domar A. The relationship between stress and infertility. Dialogues Clin. Neurosci. 2018; 20(1): 41-7. https://dx.doi.org/10.31887/DCNS.2018.20.1/klrooney.
- Гаврилова Е.А. Стресс и патология сердца. М.: ГЭОТАР-Медиа; 2024. 237 с. [Gavrilova E.A. Stress and heart pathology. Moscow: GEOTAR-Media; 2024. 237 p. (in Russian)].
- Vanhollebeke G., De Smet S., De Raedt R., Baeken C., van Mierlo P., Vanderhasselt M.A. The neural correlates of psychosocial stress: A systematic review and meta-analysis of spectral analysis EEG studies. Neurobiol. Stress. 2022; 18: 100452. https://dx.doi.org/10.1016/j.ynstr.2022.100452.
- Ясная Д.В., Проскурякова Л.А., Мартынов И.Д., Лихачева В.В. Электроэнцефалографические показатели переживания стресса у женщин, проходящих подготовку к процедуре экстракорпорального оплодотворения. Современные вопросы биомедицины. 2024; 8(3): 18. [Yasnaya D.V., Proskuryakova L.A., Martynov I.D., Likhachyova V.V. Electroencephalographic indicators of stress of women in preparation for in vitro fertilization procedure. Modern Issues of Biomedicine. 2024; 8(3): 18. (in Russian)]. https://dx.doi.org/10.24412/2588-0500-2024_08_03_18.
- Приказ Минздрава РФ от 31.07.2020 № 803Н «О порядке использования вспомогательных репродуктивных технологий, противопоказаниях и ограничениях к их применению». Доступно по: https://normativ.kontur.ru/document?moduleId=1&documentId=373901 [Order of the Ministry of Health of the Russian Federation No. 803N dated 07/31/2020 «On the procedure for using assisted reproductive technologies, contraindications and restrictions on their use. Available at: https://normativ.kontur.ru/document?moduleId=1&documentId=373901 (in Russian)].
- Мартынов И.Д., Ямщикова А.В., Флейшман А.Н., Петровский С.А. Эффективность транскраниальной магнитной стимуляции в лечении профессиональной полинейропатии. Гигиена и санитария. 2023; 102(4): 351-5. [Martynov I.D., Yamshchikova A.V., Fleishman A.N., Petrovskiy S.A. Efficiency of the transcranial magnetic stimulation in the treatment of occupational polyneuropathy. Hygiene and Sanitation. 2023; 102(4): 351-5. (in Russian)]. https://dx.doi.org/10.47470/0016-9900-2023-102-4-351-355.
- Александров М.В., ред. Электроэнцефалография: руководство. 3-е изд. Санкт-Петербург: СпецЛит; 2019. 200 с. [Alexandrov M.V., ed. Electroencephalography: a guide. 3 ed. St. Petersburg: SpetsLit; 2019. 200 p. (in Russian)].
- Simionescu G., Doroftei B., Maftei R., Obreja B.E., Anton E., Grab D. et al. The complex relationship between infertility and psychological distress (review). Exp. Ther. Med. 2021; 21(4): 306. https://dx.doi.org/10.3892/etm.2021.9737.
- Воронина И.Д., Бохан Т.Г., Терехина О.В., Малых С.Б., Ковас Ю.В. Демографические показатели, образ жизни и здоровье в семьях с естественной и индуцированной беременностью в России и Великобритании. Теоретическая и экспериментальная психология. 2017; 9(4): 63-76. [Voronina I.D., Bohan T.G., Terekhina O.V., Malykh S.B., Kovas Yu.V. Demographic indicators, lifestyle, and health in families with natural and induced pregnancies in Russia and Great Britain. Theoretical and Experimental Psychology. 2017; 9(4): 63-76. (in Russian)].
- Гончаров Г.В., Ильина О.В., Труфанова Н.Г., Воликова Г.А. Ритмическая организация ЭЭГ-коррелятов устойчивости к эмоциональному стрессу у женщин фертильного возраста. Вестник Волгоградского государственного медицинского университета. 2010; 7(4): 79-82. [Goncharov G.V., Il'ina O.V., Trufanova N.G., Volikova G.A. Rhythmic organization of EEG-correlates of stability to emotional stress at reproductive age in women. Journal of Volgograd State Medical University. 2010; 7(4): 79-82. (in Russian)].
- Rockliff H., Lightman S., Rhidian E., Buchanan H., Gordon U., Vedhara K. A systematic review of psychosocial factors associated with emotional adjustment in in vitro fertilization patients. Hum. Reprod. Update. 2014; 20(4): 594-613. https://dx.doi.org/10.1093/humupd/dmu010.
Received 05.12.2024
Accepted 13.03.2025
About the Authors
Darya V. Yasnaya, Senior Lecturer at the Department of Psychology and General Pedagogy, Kuzbass Humanitarian and Pedagogical Institute, Kemerovo State University, 654041, Russia, Kemerovo Oblast – Kuzbass, Novokuznetsk, Tsiolkovsky str., 23, st1daria@ya.ru, https://orcid.org/0009-0004-0659-7183Viktoria V. Likhacheva, Dr. Med. Sci., Professor, Department of Obstetrics and Gynecology, Novokuznetsk State Institute for Further Training of Physicians – Branch Campus of the Russian Medical Academy of Continuous Professional Education, Ministry of Health of Russia, 654005, Russia, Kemerovo Oblast – Kuzbass, Novokuznetsk,
Stroiteley Ave., 5, Higher Category Obstetrician-Gynecologist, viroli@mail.ru, https://orcid.org/0000-0002-5637-7590
Larisa A. Proskuryakova, Dr. Bio. Sci., Professor, Department of Psychology and General Pedagogy, Kuzbass Humanitarian and Pedagogical Institute, Kemerovo State University, 654041, Russia, Kemerovo Oblast – Kuzbass, Novokuznetsk, Tsiolkovsky str., 23; Associate Professor, Department of Hygiene, Epidemiology and Healthy Living, Novokuznetsk State Institute for Further Training of Physicians – Branch Campus of the Russian Medical Academy of Continuous Professional Education, Ministry of Health of Russia, 654005, Russia, Kemerovo Oblast – Kuzbass, Novokuznetsk, Stroiteley Ave., 5, lora-al@yandex.ru, Researcher ID: AAE-5730-2022, SPIN: 5636-0613,
Scopus Author ID: 57200689936, https://orcid.org/0000-0002-9583-9161
Valeriya V. Alontseva, 6th year student, Medical Faculty, Pavlov First Saint Petersburg State Medical University, Ministry of Health of Russia, 197022, Russia, Saint Petersburg, Leo Tolstoy str., 6-8, leral2612@mail.ru
Olga V. Azarova, Obstetrician-Gynecologist, Reproductive Specialist, Head of the ART Department, Expert LLC, 654041, Russia, Kemerovo Oblast – Kuzbass, Novokuznetsk, Kutuzov str., 17a, az.o@mail.ru, https://orcid.org/0000-0002-2954-7494
Corresponding author: Larisa A. Proskuryakova, lora-al@yandex.ru
Similar Articles

