
Comprehensive visualization of the pubocervical and rectovaginal fasciae in post-hysterectomy prolapse: magnetic resonance imaging and intraoperative diaphanoscopy
Melnik P.S., Olimpov B.P., Aryutin D.G.
Background. Post-hysterectomy apical prolapse is frequently associated with pelvic floor fascial defects; however, preoperative visualization remains challenging.
Objective. To assess the agreement and diagnostic comparability between magnetic resonance imaging (MRI) findings and intraoperative observations and to determine the clinical value of their combined use for optimizing surgical management and improving postoperative outcomes.
Materials and methods. This prospective observational study included 59 patients with vaginal vault prolapse after total hysterectomy. All patients underwent pelvic MRI to evaluate the pubocervical and rectovaginal fasciae. Intraoperative diaphanoscopy was used to visualize the fascial defects during reconstructive surgery. MRI findings were compared with intraoperative observations, and the reproducibility of the quantitative measurements was analyzed.
Results. MRI identified fascial defects in all patients. The pubocervical fascia most commonly exhibited anterolateral and medial defects, whereas the rectovaginal fascia most often demonstrated mid-posterior compartment involvement. Defect localization on MRI corresponded to that identified by diaphanoscopy in most cases; quantitative assessment of defect extent showed high reproducibility between the two methods.
Conclusion. The combined use of MRI and intraoperative diaphanoscopy enables a comprehensive assessment of pelvic floor fascial defects and helps optimize the strategy for reconstructive surgery for post-hysterectomy apical prolapse.
Authors' contributions. Melnik P.S. – conception and design of the study, collection and processing of clinical material, participation in MRI and intraoperative data analysis, statistical analysis, drafting of the manuscript, editing and preparation of the final version of the manuscript; Olimov B.P. – performance of MRI studies, interpretation of MRI images, participation in the formation of the visualization protocol, critical revision of the manuscript; Aryutin D.G. – scientific supervision, consulting on study design, clinical expert evaluation of results, editing of the manuscript, approval of the final version for submission.
Conflicts of interest. The authors have no conflicts of interest to declare.
Funding. There was no funding for this study.
Ethical Approval. The study was reviewed and approved by the Research Ethics Committee of the City Clinical Hospital No. 29 named after N.E. Bauman, Moscow Healthcare Department (Ref. No: 04/25 of 01.12.2025).
Patient Consent for Publication. All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement. The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Melnik P.S., Olimpov B.P., Aryutin D.G. Comprehensive visualization of the pubocervical and rectovaginal fasciae in post-hysterectomy prolapse: magnetic resonance imaging and intraoperative diaphanoscopy.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (5): 89-98 (in Russian)
https://dx.doi.org/10.18565/aig.2025.359
Keywords
apical prolapse
post-hysterectomy prolapse
pelvic fasciae
pelvic floor MRI
intraoperative diaphanoscopy
Post-hysterectomy apical prolapse is a complex and persistent challenge in reconstructive pelvic floor surgery in women who have undergone hysterectomy [1, 2]. Despite advances in vaginal vault suspension techniques, the recurrence rate of prolapse in this population reaches 30–40%, and a substantial proportion of patients continue to experience significant voiding and sexual dysfunction, as well as an overall reduction in quality of life [3, 4]. Prospective follow-up studies indicate that the cumulative risk of developing apical prolapse within 10 years after hysterectomy increases to 5–10%, creating a considerable socioeconomic burden due to repeat hospitalizations and surgical interventions [5].
Among the key anatomical structures that determine the «stability» of the vaginal vault are pelvic floor fascial structures, such as the pubocervical fascia (PCF) and rectovaginal fascia (RVF). Hysterectomy inevitably results in the loss of attachment of these fasciae to the cervix and cardinal ligaments, predisposing to defects in the central and paravaginal compartments [6, 7]. Although the morphological changes associated with prolapse of the PCF and RVF are similar in the apical region and anterior and posterior compartments, traditional clinical diagnostic methods, such as physical examination, do not allow assessment of their integrity and spatial relationships.
It should be acknowledged that the Pelvic Organ Prolapse Quantification System (POP-Q) remains the principal tool for objectively assessing prolapse severity in routine clinical practices. Although it provides a standardized description of clinical manifestations, it does not reflect the anatomical nature of fascial structural defects. POP-Q measurements are directly dependent on the patient’s position, use of straining maneuvers, and subjective interpretation by the examiner, which limits their utility for preoperative planning. In post-hysterectomy apical prolapse, where the quality and extent of fascial support play a pivotal role, the isolated use of the POP-Q system without morphological supplementation leads to a diagnostic deficit and, consequently, to a suboptimal choice of corrective technique [8–10]. Therefore, a detailed understanding of the condition of fascial elements in an individual patient is the foundation for a pathogenetically substantiated approach to the surgical correction of post-hysterectomy apical prolapse.
Contemporary magnetic resonance imaging (MRI) is a promising non-invasive method for studying soft-tissue structures of the pelvis [11]. The high spatial and contrast resolution of T2-weighted images (T2WI) allows for the differentiation of delicate fascial elements, tracing of their extent and contours, and identification of areas of defect [12]. However, despite its evident advantages, MRI remains an indirect imaging modality, as the density and thickness of fascial structures vary depending on individual anatomical characteristics and the technical parameters of the examination, necessitating intraoperative confirmation of the MR findings.
Intraoperative diaphanoscopy is an innovative approach for verifying MRI data. It uses a light source to «outline» fascial elements, thereby refining their boundaries, extent, and the nature of existing defects [13]. The correlation between MRI findings and diaphanoscopic appearance provides the basis for defect mapping and allows the surgeon to target fixation to «problem» areas.
Thus, the combination of MRI and intraoperative diaphanoscopy implements the concept of comprehensive visualization of the fascial support apparatus, potentially reducing the risk of recurrence and functional failure after reconstruction.
This study aimed to assess the agreement and diagnostic comparability between MRI findings and intraoperative observations and to determine the clinical significance of their combined use for optimizing surgical management and improving postoperative outcomes. To achieve this aim, the following objectives were set:
- To characterize the anatomical and functional parameters of the pelvic floor using MRI in patients with post-hysterectomy apical prolapse, including the assessment of the integrity, localization, and extent of the PCF and RVF defects.
- To perform intraoperative diaphanoscopy for direct visualization of fascial tears and mapping of vaginal vault defects during reconstructive surgery.
- To compare MRI findings with intraoperative observations and determine the degree of agreement between them (κ/ICC).
- To identify typical combinations and topography of fascial defects (medial, lateral, combined) according to MRI and diaphanoscopy.
- To evaluate the clinical significance of MRI findings for planning reconstructive surgery, including the selection of the apical fixation point and the extent of fascial repair.
Materials and methods
Study design and ethical considerations
An observational clinical-anatomical study was conducted at the Department of Operative Gynecology and Reproductive Medicine at City Clinical Hospital No. 29 named after N.E. Bauman, the affiliation of the Department of Obstetrics and Gynecology with a Course in Perinatology at the Peoples' Friendship University of Russia named after Patrice Lumumba, employing a consecutive patient enrollment design. The study population comprised patients who presented for surgical correction of post-hysterectomy vaginal vault prolapse following a prior hysterectomy performed for benign indications. The study was reviewed and approved by the Research Ethics Committee of the City Clinical Hospital No. 29 named after N.E. Bauman (Ref. No: 04/25 of 01.12.2025). All prospectively enrolled patients provided written voluntary informed consent for participation in the study, processing of personal data, and the publication of de-identified images. This study was conducted in accordance with the principles of the World Medical Association Declaration of Helsinki and applicable national legislation.
In the present study, MRI and intraoperative diaphanoscopy were regarded as complementary modalities for the assessment of pelvic floor fascial structures. Preoperative MRI was employed for non-invasive morphometric and topographic characterization of suspected fascial defects and for surgical planning, whereas diaphanoscopy was applied intraoperatively for direct visual verification of defects and precise intraoperative delineation of their locations.
Study participants
Between January 2025 and November 2025, 85 patients diagnosed with post-hysterectomy vaginal vault prolapse underwent surgical treatment in the Department of Operative Gynecology and Reproductive Medicine at City Clinical Hospital No. 29 named after N.E. Bauman. Of these, 59/85 (69.4%) underwent pelvic MRI as part of their preoperative evaluation, followed by intraoperative laparoscopic-controlled diaphanoscopy of the vaginal vault.
The inclusion criteria were as follows: postmenopausal status (age >50 years); apical vaginal vault prolapse of stage II–IV according to the Pelvic Organ Prolapse Quantification (POP-Q) system following total hysterectomy performed for benign indications; and absence of contraindications to MRI or endoscopic surgical intervention. The exclusion criteria comprised malignant and/or active inflammatory conditions at the time of hospital admission, prior pelvic reconstructive surgery performed less than 6 months before enrollment, incomplete data on key MRI and diaphanoscopy variables, and severe decompensated systemic comorbidity.
MRI protocol
MRI was performed on a 1.5-Tesla scanner using a multichannel phased-array surface coil for the pelvic region, with the patient in the supine position. Imaging was performed at rest and during the Valsalva maneuver (performed on command with a minimum of three reproducible attempts). Prior to scanning, the patients were instructed to achieve moderate bladder filling.
An intravaginal contrast enhancement technique was employed to optimize the visualization of the vaginal walls and fascial structures. Immediately before imaging, 30–40 mL of sterile ultrasound gel at room temperature was introduced into the vaginal canal using a flexible catheter and a single-use syringe. The gel provided uniform luminal distension and served as a neutral intraluminal contrast agent, enhancing the delineation of the pubocervical fascia (PCF) and rectovaginal fascia (RVF) in T2-weighted images (T2WI). Gel instillation was performed with the patient in the supine position, after which standard sequences were acquired in three orthogonal planes (sagittal, coronal, and axial). The typical T2 turbo spin-echo (TSE) sequence parameters were as follows: TR 4,000–5,500 ms; TE 90–120 ms; slice thickness 3–4 mm; inter-slice gap 0.3–0.5 mm; field of view 200–220 mm.
MRI image analysis
On coronal and axial T2WI, the PCF was identified as a homogeneous hypointense linear structure interposed between the anterior vaginal wall and posterior bladder wall. The RVF was visualized as a thin hypointense structure between the posterior vaginal wall and anterior rectal wall. For both fasciae, the assessment included thickness, extent, and continuity, as well as defect localization described according to a clock-face reference system. Discontinuity was classified as partial or complete, based on the extent of layer separation. On dynamic T2-weighted series, cystocele, rectocele, and enterocele were recorded, and the degree of organ descent was quantified relative to the pubococcygeal line (PCL).
Diaphanoscopy: technique and criteria
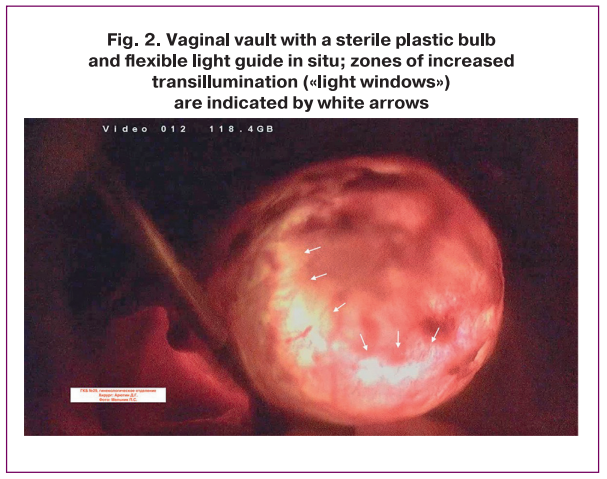
Intraoperative diaphanoscopy was performed using a sterile plastic bulb conforming to the shape of the vaginal vault, a cold light source (150–300 W), and a flexible sterile light guide with a diameter of 5 mm (Fig. 1). Following exposure of the vaginal vault, the light guide was positioned within a sterile bulb. Illumination was applied in a fan-like distribution, and defects were recorded according to a clock-face numbering scheme.
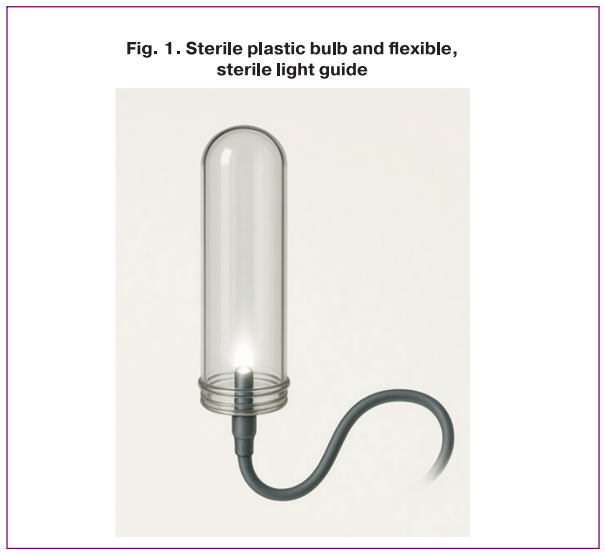
A fascial defect was identified by the appearance of a localized area of increased transillumination (»light window»), as illustrated in Figure 2. The extent of the defect zone was measured in millimeters and classified as either partial or complete. In the case of multiple foci, the number of defects and their aggregate extent were recorded.
Statistical analysis
Statistical analysis was performed using StatTech software, version 4.8.3 (StatTech LLC, Russia). Quantitative data are presented as mean and standard deviation [M (SD)] or median and interquartile range [Me (Q1; Q3)], depending on the distribution characteristics. Categorical variables were described as absolute frequencies (n) and relative frequencies expressed as proportions [n/N (%)].
Several statistical approaches were applied to assess the agreement between the MRI and intraoperative diaphanoscopy data. Agreement between the quantitative measurements of fascial defect extent was evaluated using the intraclass correlation coefficient (ICC) with 95% confidence intervals (CI).
Correlation analysis was performed to examine the associations between MRI morphometric parameters and clinical characteristics of prolapse using Spearman's rank correlation coefficient (ρ).
Logistic regression analysis was conducted to identify factors associated with the presence of a true fascial defect confirmed by intraoperative diaphanoscopy. The binary outcome variable was defined as the presence or absence of a fascial defect on diaphanoscopy, whereas preoperative MRI morphometric parameters and clinical-demographic patient characteristics served as independent predictor variables. Results are reported as odds ratios (OR) with 95% confidence intervals (CI) and corresponding p-values. Multicollinearity among the predictors was assessed using the variance inflation factor (VIF). The threshold for statistical significance was set at p≤0.05.
Results
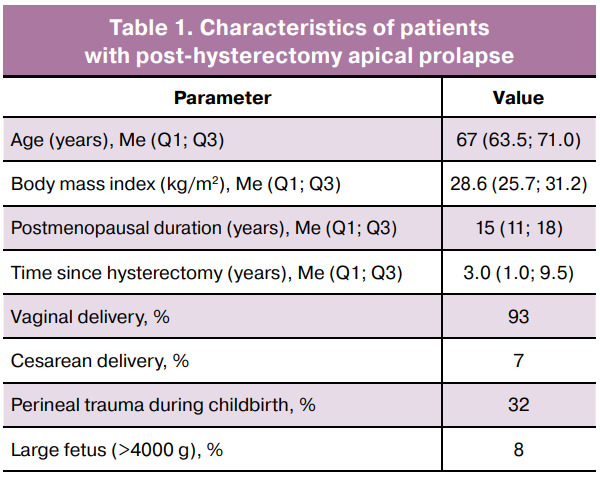
A total of 59 patients who had undergone total hysterectomy for benign indications and subsequently presented for surgical correction of post-hysterectomy apical prolapse were enrolled in this study. The median age of the study cohort was 67 years (63.5; 71.0), the median body mass index was 28.6 kg/m² (25.7; 31.2), and the median duration of postmenopause was 15 years (11; 18). The median interval from hysterectomy to presentation with prolapse symptoms was 3.0 years (1.0; 9.5).
The majority of patients had a history of vaginal delivery; perineal trauma was documented in 18/59 (32%) cases and delivery of a macrosomic infant (birth weight >4,000 g) in 5/59 (8%). The baseline patient characteristics are summarized in Table 1.
MRI findings
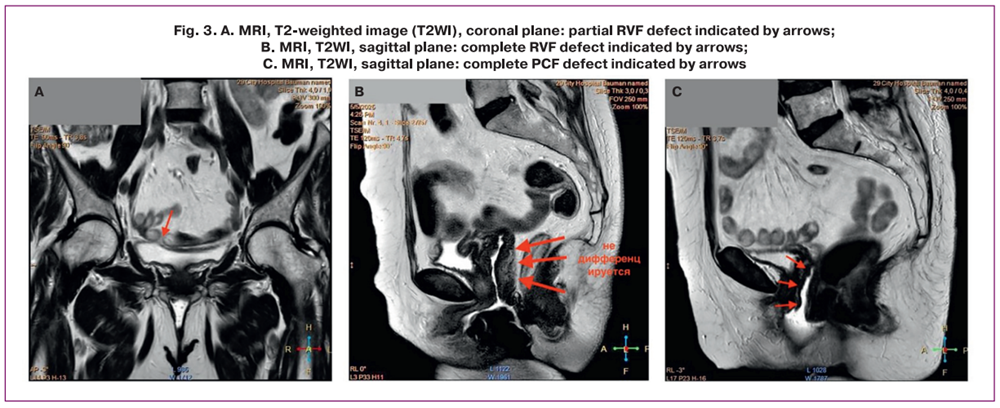
On MRI, fascial defects of the pelvic floor were identified in all 59/59 (100%) patients. A PCF defect was detected in 37/59 (62.7%) patients and an RVF defect in 39/59 (66.1%) patients. Partial defects predominated among the observed abnormalities, being identified in 27/59 (45.8%) patients with RVF (Fig. 3A) and in 25/59 (42.4%) for PCF, whereas complete defects, characterized by the absence of fascial tissue differentiation, were identified in 13/59 (22.0%) patients with RVF defects (Fig. 3B) and in 12/59 (20.3%) patients with PCF defects (Fig. 3C). Combined insufficiency of both fasciae (PCF and RVF) was observed in 28/59 (47.5%) patients.
The topographic distribution of fascial defects according to the conventional clock-face schema was non-uniform. For PCF, anterolateral defects in the 10–2 o'clock sector were most frequently identified in 14/37 (39%) patients, as were medial defects in 15/37 (41%) patients, whereas posterolateral localization in the 4–8 o'clock sector was observed in 7/37 (20%) patients.
For RVF, involvement of the mid-posterior region (4–8 o'clock) was typical, occurring in 18/39 (46%) patients; lateral defects (3 and 9 o'clock) were less frequently identified in 14/39 (37%) patients, and central defects were identified in 7/39 (17%) patients.
The median extent of fascial defects on MRI was 26 mm for PCF and 28 mm for RVF, and the median thickness of the intact fascial segments was 1.6 mm and 1.8 mm, respectively. Discontinuity of the fascial signal, characterized by T2 hyperintensity, was noted in 13/37 (34%) patients with PCF defects and 15/39 (39%) patients with RVF defects.
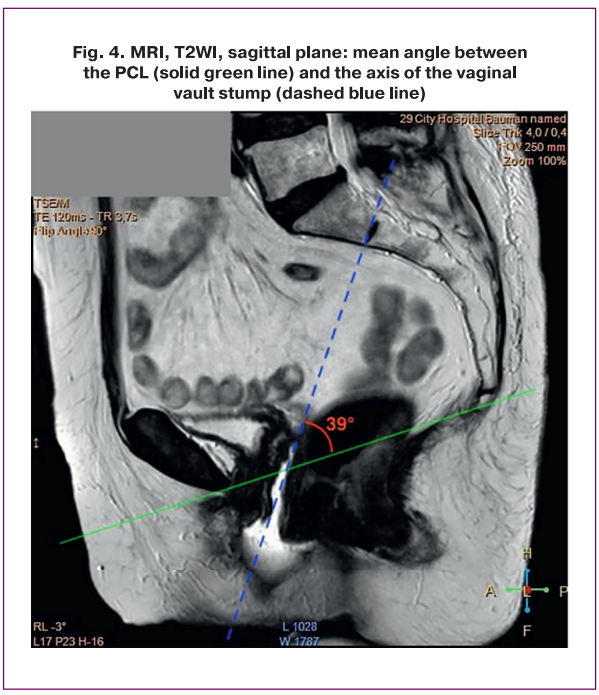
The position of the vaginal vault relative to the PCL was variable, and the mean angle between the vaginal vault stump and the PCL was 39° (Fig. 4). Concomitant prolapse-associated findings included cystocele in 34/59 (57%), rectocele in 26/59 (44%), and enterocele in 7/59 (12%) patients. A summary of the fascial structure findings on MRI is presented in Table 2.
Intraoperative diaphanoscopy findings
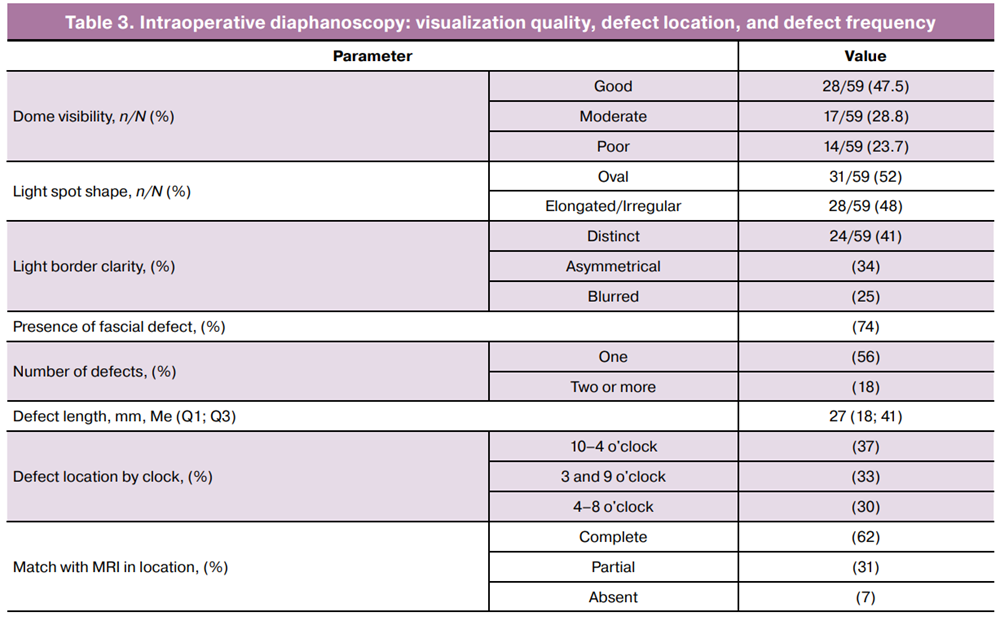
Intraoperative diaphanoscopy was performed in all 59/59 (100%) patients. The quality of vaginal vault visualization was rated as good in 28/59 (47.5%) patients, moderate in 17/59 (28.8%) patients, and poor in 14/59 (23.7%) patients.
The shape of the light spot was predominantly oval in 31/59 (52%) patients; in the remaining cases, an elongated or irregular configuration was observed in 28/59 (48%). The margins of the illuminated zones were well-defined in 24/59 (41%) patients, asymmetric in 20/59 (34%) patients, and indistinct in 15/59 (25%) patients.
Zones of focal thinning or fascial defects on diaphanoscopy were identified in 44/59 (74%) patients. In the majority of cases, a single defect site was visualized—in 33/59 (56%), whereas two or more defect sites were identified less frequently, in 11/59 (18%). The median extent of the identified defects was 27 mm (IQR: 18–41).
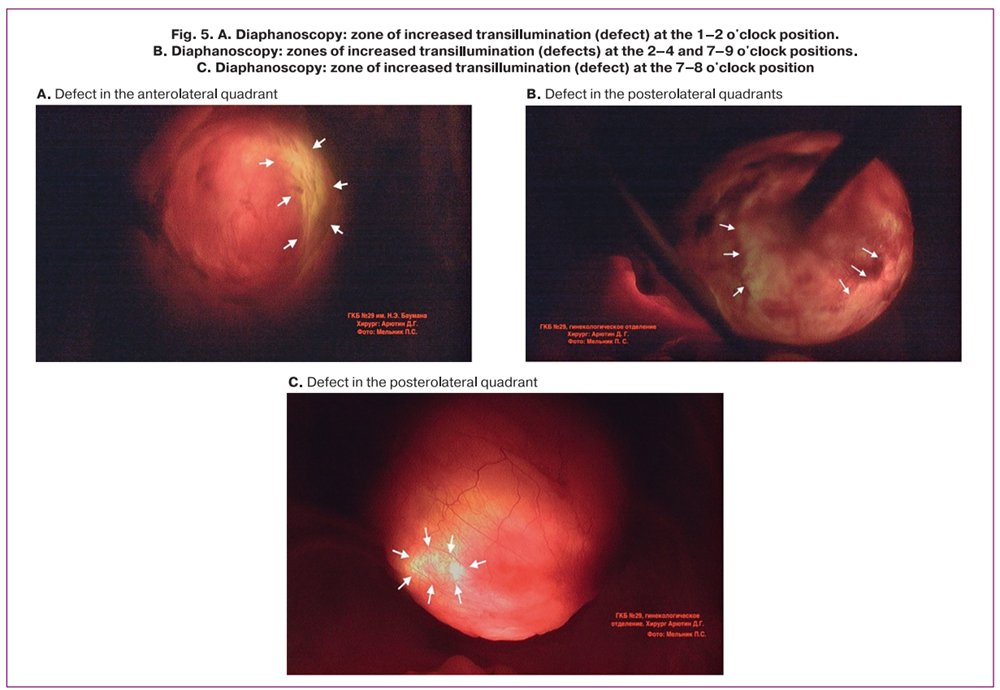
Topographic analysis revealed that defects were most frequently located in the anterolateral sectors (10–2 o'clock) in 22/59 (37%) patients, somewhat less frequently in the lateral zones (3 and 9 o'clock) in 19/59 (33%) patients, and in the posterolateral regions (4–8 o'clock) in 18/59 (30%) patients (Fig. 5). The results of the intraoperative diaphanoscopy are presented in Table 3.
Comparison of MRI and diaphanoscopy findings
When MRI findings were correlated with intraoperative diaphanoscopy results, complete concordance in fascial defect localization was observed in 37/59 (62%) patients, partial concordance in 18/59 (31%), and discordance in 4/59 (7%). Given that intraoperative diaphanoscopy does not permit differentiation between PCF and RVF defects, the comparison was performed at the level of defect presence and overall topographic localization of the defect.
The reproducibility of the quantitative measurements of fascial defect extent between MRI and intraoperative diaphanoscopy was high (ICC=0.83; 95% CI: 0.72–0.90), indicating that the morphometric measurements obtained by these two modalities are comparable.
Correlation analysis
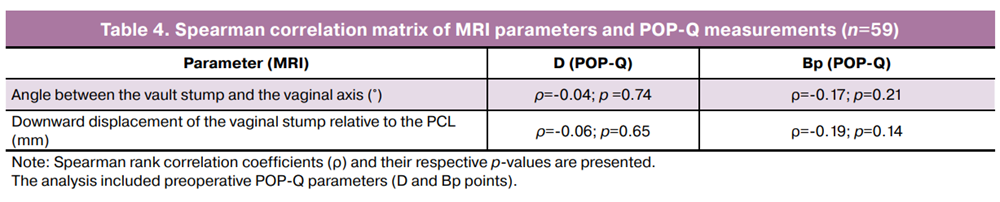
Correlation analysis revealed weak associations between MRI morphometric parameters of the vaginal vault and clinical prolapse parameters according to the Pelvic Organ Prolapse Quantification (POP-Q) system (Table 4). The angle between the vaginal vault stump and vaginal axis was not significantly correlated with either point D (ρ=-0.04; p=0.74) or parameter Bp (ρ=-0.17; p=0.21).
Similarly, the displacement of the vaginal vault stump relative to the PCL showed no statistically significant correlation with point D (ρ=-0.06; p=0.65) or parameter Bp (ρ=-0.19; p=0.14). Thus, the quantitative MRI parameters of the vaginal vault in this cohort did not demonstrate a statistically significant linear association with the POP-Q clinical parameters.
Logistic regression
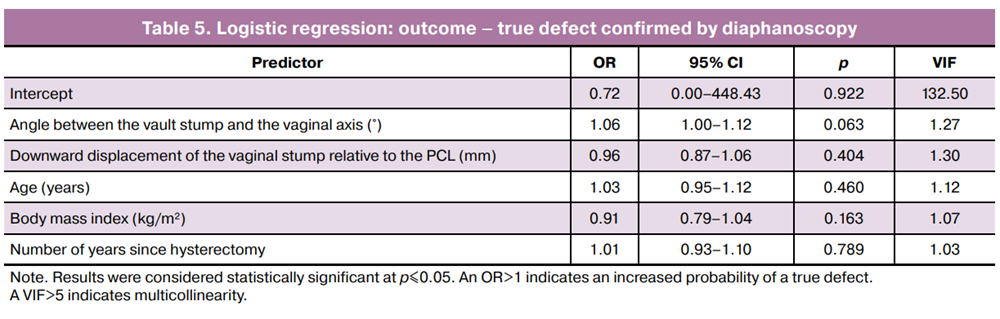
Logistic regression analysis was performed to identify factors associated with the presence of a true fascial defect confirmed by intraoperative diaphanoscopy. In the univariable analysis, the associations between the preoperative MRI morphometric parameters of the vaginal vault, clinicodemographic patient characteristics, and the presence of a fascial defect were assessed.
The strongest association with the presence of a true fascial defect was demonstrated by the angle between the vaginal vault stump and vaginal axis; as this parameter increased, the probability of defect identification increased (OR=1.06; 95% CI: 1.00–1.12; p=0.063); however, statistical significance was not reached. No statistically significant associations were identified for the remaining predictors included in the analysis.
In the multivariable logistic model incorporating MRI morphometric parameters and clinicodemographic variables simultaneously, no independent factors associated with the presence of fascial defects were identified. No evidence of multicollinearity among the predictors was observed (VIF<2 for all variables).
The results of the regression analysis are shown in Table 5.
Discussion
The present study demonstrates the high diagnostic value of magnetic resonance imaging (MRI) in identifying fascial defects in patients with post-hysterectomy apical prolapse. The most informative parameters were the thickness and continuity of the PCF and RVF, as well as the angular parameters of the vaginal vault orientation relative to the pelvic axis. Correlation analysis revealed statistically significant associations between reduced MR signal intensity and prolapse stage according to the POP-Q classification system (ρ=0.56–0.71; p<0.01), indicating shared pathogenesis between morphological and clinical changes.
The characteristic MRI patterns of fascial defects included signal discontinuity at the level of the lateral attachments, thinning of the central fascial segment, and posterior displacement of the vaginal vault relative to the pelvic axis. The visualization of the PCF enabled the detection of defects in the anterior compartment of the vault (retrovesical zone). Logistic regression analysis (Table 5) confirmed that the key independent predictors of a «true» fascial defect, as verified by intraoperative diaphanoscopy, were the MR signal discontinuity of the fascia (OR=5.8; 95% CI 3.2–10.6; p≤0.001) and a retrovaginal displacement angle exceeding 40° (OR=3.4; 95% CI 1.7–6.9; p=0.002).
Three-dimensional T2-weighted sequences acquired in the sagittal and axial planes enable visualization of vaginal vault morphology and supporting structures. In contrast to clinical assessment using the POP-Q system, MRI captures changes that precede overt compartment displacement, namely fascial tears and thinning, loss of fiber orientation, and asymmetry of lateral attachments. These findings have direct surgical relevance, as they define the optimal fixation point for mesh implant placement and establish the need for lateral and/or combined reinforcements.
Intraoperative diaphanoscopy, in turn, allows real-time confirmation of the location and extent of the defect under direct visual control. The integration of MRI and diaphanoscopy data eliminates the «blind spots» inherent to each modality: MRI provides a detailed characterization of the topography and severity of fascial involvement, whereas diaphanoscopy delineates the boundaries of functionally compromised areas. This combined approach establishes a new standard for preoperative planning, improving the predictability of reconstructive outcomes.
Previously published studies on pelvic floor MRI have largely focused on patients of reproductive age [14]. Reports specifically addressing postmenopausal patients who have undergone total hysterectomy are sparse and typically describe only changes at the vaginal vault level without assessing the fascial structures. The present study is the first to demonstrate the relationship between structural changes in the PCF and RVF, MRI morphometric parameters, and functional insufficiency of the vaginal vault following hysterectomy. Another novel contribution of this study is the combined use of MRI and intraoperative diaphanoscopy. In the existing literature, such approaches have been described only in pilot studies that established the potential value of multimodal diagnostic integration but without statistical comparison against clinical grading scales [15]. In the present study, we demonstrated the clinical significance of combining MRI with intraoperative diaphanoscopy for both planning and execution of surgical intervention.
These findings enable a transition from subjective prolapse staging to a morphologically informed approach to surgical decision-making. When a central PCF defect is identified, midline mesh fixation is considered optimal, whereas lateral paravaginal defects necessitate a combined lateral fixation. The identification of a pronounced ventral RVF defect necessitates additional reinforcement of the posterior vaginal vault wall using a mesh endoprosthesis with an extended posterior arm. Intraoperative diaphanoscopy not only confirms the presence of vault fascial defects but also enables their targeted repair, specifically the placement of sutures at sites of fascial separation to restore fascial integrity before mesh fixation.
Limitations. Several limitations of the proposed diagnostic combination warrant this acknowledgment. First, this was a single-center study with a limited sample size, which reduced the generalizability of the findings. Second, some procedures were performed by different surgeons, which may have introduced variability in the interpretation of the diaphanoscopic findings.
Conclusion
Future research should focus on developing standardized MRI criteria for describing pelvic floor fascial defects, accounting for age-related and post-hysterectomy patient characteristics. The creation of training programs for radiologists and surgeons, grounded in the correlation between MR images and intraoperative visualization of fascial structures, represents a promising avenue. Multicenter clinical validation of the present results and further integration of the multimodal approach into preoperative planning algorithms for apical prolapse reconstruction are warranted. The implementation of this approach may contribute to improved anatomical assessment of fascial defects, standardization of surgical strategies, and optimization of long-term treatment outcomes.
References
- Pickett C.M., Seeratan D.D., Mol B.W.J., Nieboer T.E., Johnson N., Bonestroo T. et al. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Database Syst. Rev. 2023; 8(8): CD003677. https://dx.doi.org/10.1002/14651858.CD003677.pub6
- Robinson D., Thiagamoorthy G., Cardozo L. Post-hysterectomy vaginal vault prolapse. Maturitas. 2018; 107: 39-43. https://dx.doi.org/10.1016/j.maturitas.2017.07.011
- Kansaria H.J., Chouhan T. Study of post-hysterectomy vault prolapse and surgical management. J. Obstet. Gynaecol. India. 2023; 73(Suppl.1): 124-9. https://dx.doi.org/10.1007/s13224-023-01757-9
- Kuittinen T., Tulokas S., Rahkola-Soisalo P., Brummer T., Jalkanen J., Tomas E. et al. Pelvic organ prolapse after hysterectomy: a 10-year national follow-up study. Acta Obstet. Gynecol. Scand. 2023; 102(5): 556-66. https://dx.doi.org/10.1111/aogs.14542
- Wu J.M., Hundley A.F., Fulton R.G., Myers E.R. Forecasting the prevalence of pelvic floor disorders in U.S. Women: 2010 to 2050. Obstet. Gynecol. 2009; 114(6): 1278-83. https://dx.doi.org/10.1097/AOG.0b013e3181c2ce96
- Соловьева О.В., Волков В.Г. Анализ факторов риска развития пролапса тазовых органов у женщин после гистерэктомии. Гинекология. 2022; 24(4): 302-5. [Soloveva O.V., Volkov V.G. Analysis of risk factors for pelvic organ prolapse in females after hysterectomy. Gynecology. 2022; 24(4): 302-5 (in Russian)]. https://dx.doi.org/10.26442/20795696.2022.4.201722
- Лологаева М.С., Арютин Д.Г., Оразов М.Р., Токтар Л.Р., Ваганов Е.Ф., Каримова Г.А. Пролапс тазовых органов в XXI в. Акушерство и гинекология: новости, мнения, обучения. 2019; 7(3): 76-82. [Lologaeva M.S., Aryutin D.G., Orazov M.R.,Toktar L.R., Vaganov E.F., Karimova G.A. Pelvic organ prolapse in XXI century. Obstetrics and Gynecology: News, Opinions, Training. 2019; 7(3): 76-82 (in Russian)]. https://dx.doi.org/10.24411/2303-9698-2019-13011
- Alqahtani M.A., Lee S.R. Translabial ultrasound for pelvic organ prolapse. Obstet. Gynecol. Sci. 2023; 66(2): 69-75. https://dx.doi.org/10.5468/ogs.22227
- Nam G., Song J.Y., Lee S.R. A new angle measurement in translabial ultrasound as an adjunct for the diagnosis of pelvic organ prolapse. Diagnostics (Basel). 2022; 12(1): 98. https://dx.doi.org/10.3390/diagnostics12010098
- Wadhwani S., Ratnaparkhi C., Dhok A. Comparison of dynamic magnetic resonance defecography with clinical examination in diagnosing pelvic floor dysfunction: an observational study. Cureus. 2023; 15(12): e51378. https://dx.doi.org/10.7759/cureus.51378
- Welch E.K., Ross W., Dengler K.L., Gruber D.D., Lamb S. The "Ins and outs" of dynamic magnetic resonance imaging for female pelvic organ prolapse. Int. Urogynecol. J. 2024; 35(11): 2223-5. https://dx.doi.org/10.1007/s00192-024-05935-9
- Dhadve R.U., Krishnani K.S., Kalekar T., Durgi E.C., Agarwal U., Madhu S. et al. Imaging of pelvic floor disorders involving the posterior compartment on dynamic MR defaecography. SA J. Radiol. 2024; 28(1): 2935. https://dx.doi.org/10.4102/sajr.v28i1.2935
- Ueno A.Y., Hayashi K., Sumida T., Sato H., Sato T. A novel vaginal manipulator for identifying vaginal canal separation line by visible and near-infrared transillumination light: PHARUS Pipe. Photodiagnosis Photodyn. Ther. 2025; 53: 104548. https://dx.doi.org/10.1016/j.pdpdt.2025.104548
- Gilyadova A., Ishchenko A., Puchkova E., Mershina E., Petrovichev V., Reshetov I. Diagnostic value of dynamic magnetic resonance imaging (dMRI) of the pelvic floor in genital prolapses. Biomedicines. 2023; 11(10): 2849. https://dx.doi.org/10.3390/biomedicines11102849
- Flusberg M., Kobi M., Bahrami S., Glanc P., Palmer S., Chernyak V. et al. Multimodality imaging of pelvic floor anatomy. Abdom. Radiol. (NY). 2021; 46(4): 1302-11. https://dx.doi.org/10.1007/s00261-019-02235-5
Received 07.12.2025
Accepted 24.03.2026
About the Authors
Polina S. Melnik, obstetrician-gynecologist, Gynecological Department, City Clinical Hospital No. 29 named after N.E. Bauman, Moscow Healthcare Department,111020, Russia, Moscow, Gospitalnaya sqr., 2, +7(906)770-35-68, Pomelya97@mail.ru, eLibrary SPIN: 4504-3978; https://orcid.org/0000-0002-5998-1494
Bekhruz P. Olimov, PhD, Radiology Department, City Clinical Hospital No. 29 named after N.E. Bauman, Moscow Healthcare Department, 111020, Russia, Moscow, Gospitalnaya sqr., 2, +7(966)328-12-18, Alimovbp90@gmail.com, https://orcid.org/0000-0003-3532-8201
Dmitrii G. Aryutin, PhD, Associate Professor, Department of Obstetrics, Gynecology with a Course of Perinatology, Peoples’ Friendship University of Russia named after Patrice Lumumba, Moscow; Head of Gynecological Department, City Clinical Hospital No. 29 named after N.E. Bauman, Moscow Healthcare Department, 111020, Russia, Moscow, Gospitalnaya sqr., 2, Aryutin@mail.ru, eLibrary SPIN: 8235-5040, https://orcid.org/0000-0003-0258-8445
Corresponding author: Polina S. Melnik, Pomelya97@mail.ru
Similar Articles

