
Additional prognostic value of second-trimester biomarker measurement for predicting preeclampsia before 37 weeks in a Russian cohort
Ivshin A.A., Boldina Yu.S., Malyshev N.A.
Objective: To assess the additional prognostic value of second-trimester biomarker measurements (MAP, UtAPI, PlGF) for predicting preeclampsia before 37 weeks (pPE) and to compare the discrimination, calibration, and clinical utility of a machine learning (ML) logistic regression model and the Fetal Medicine Foundation (FMF) Bayesian algorithm.
Materials and methods: A multicenter retrospective cohort study was conducted using the MARS register of pregnant women (development cohort: 7,101 singleton pregnancies, 133 pPE cases; external validation: 1,325 pregnancies, 24 pPE cases). First-trimester (M2:15 maternal factors + 3 biomarkers) and combined first- and second-trimester (M4: M2 + 3 second-trimester biomarkers) ML models were developed and compared with FMF algorithms (T1, T2). The AUC, calibration (O:E ratio), NRI, IDI, decision curve analysis, and reclassification safety were evaluated.
Results: Second-trimester biomarkers significantly improved discrimination: ΔAUC +0.025 (p=0.001) for ML and +0.031 (p<0.001) for FMF. ML M4 and FMF T2 showed equivalent discrimination (AUC 0.927 vs. 0.935; p=0.91), but ML M4 demonstrated superior calibration (O:E 1.00 vs. 0.81). The detection rates at the 1:100 threshold were 89.5% (ML M4) and 88.0% (FMF T2). Over 99% of the risk downgrades were correct. External validation: AUC of 0.897 (ML M4) and 0.905 (FMF T2).
Conclusion: Additional second-trimester biomarker measurements significantly improved pPE prediction. ML and FMF achieved equivalent discrimination, but ML provided superior calibration in a Russian cohort, supporting the prospective evaluation of a two-stage prenatal pPE screening protocol.
Authors' contributions: Ivshin A.A. – conception and supervision of the study, expert analysis of results, editing of the manuscript; Boldina Yu.S. – drafting of the manuscript; Malyshev N.A. – data analysis and mathematical modeling.
Conflicts of interest: The authors have no conflicts of interest to declare.
Funding: The study was financially supported by the Russian Science Foundation No 24-25-00429,
https://rscf.ru/project/24-25-00429/
Ethical Approval: The study was reviewed and approved by the Research Ethics Committee of the Petrozavodsk State University (Ref. No: 18 of 20.03.2024).
Acknowledgements: The authors express their gratitude to Professor Zulfiya S. Khodjaeva, MD, PhD, Deputy Director for Research at the Institute of Obstetrics, V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Moscow, Russia, for her foundational research on the heterogeneity of preeclampsia, which shaped the theoretical framework of the present study, and for her pioneering work on the validation of preeclampsia prediction algorithms in the Russian population, which served as the starting point and methodological reference for this research.
AI disclosure: The Claude 3.5 Sonnet model (Anthropic) was used to reduce the length of this article through editorial and stylistic editing. The resulting content was then reviewed, edited and approved by the authors. The authors bear full responsibility for the accuracy of the publication's content.
Authors' Data Sharing Statement: De-identified data used in this study are available upon reasonable request, in accordance with the requirements of Federal Law No. 152-FZ 'On Personal Data'. Requests should be directed to the corresponding author (scipeople@mail.ru).
For citation: Ivshin A.A., Boldina Yu.S., Malyshev N.A. Additional prognostic value of second-trimester biomarker measurement for predicting preeclampsia before 37 weeks in a Russian cohort.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (4): 96-104 (in Russian)
https://dx.doi.org/10.18565/aig.2026.51
Keywords
preeclampsia
prediction
machine learning
Fetal Medicine Foundation
placental growth factor
uterine artery pulsatility index
calibration
prenatal screening
Preeclampsia (PE) is a multisystem complication of pregnancy that affects 2–8% of pregnant women and remains one of the leading causes of maternal and perinatal mortality [1]. Of particular clinical importance is PE that manifests before 37 weeks of gestation (preterm preeclampsia [pPE] ), which accounts for the majority of severe adverse outcomes [2–4]. This term corresponds to the criteria used in the Fetal Medicine Foundation (FMF) algorithm and the ASPRE study and is fundamentally distinct from the concept of “early-onset PE” (onset <34 weeks), as defined by the Russian clinical guidelines [3]. Evidence supporting the effectiveness of prophylactic acetylsalicylic acid administration before 16 weeks [5, 6] has established the importance of early screening for pPE.
The most extensively validated first-trimester screening tool is the FMF Bayesian algorithm [7–9], which has been recommended by the FIGO [10]. However, external validation of this algorithm in non-Western European populations has revealed substantial calibration issues, that is, discrepancies between the predicted probabilities and observed outcome frequencies [11]. In a cohort of Russian women, the validation results for the FMF algorithm in first-trimester screening were more encouraging [12]; however, calibration when second-trimester data are incorporated remains unexplored.
Machine learning (ML) methods have been proposed as an alternative, with the potential to provide automatic calibration to the local population [13]. We previously developed ML models for predicting pPE with discrimination comparable to that of the FMF algorithm [14, 15]. However, a direct comparison between ML and FMF using second-trimester data and external validation has not yet been conducted.
The addition of second-trimester biomarker measurements (19–24 weeks) is biologically justified by the completion of spiral artery remodeling by this stage [16] and has been shown to increase the detection rate of pPE from 75% to 85% at a 10% false-positive rate [17], although these data were obtained from Western European cohorts.
This study aimed to assess the incremental predictive value of second-trimester biomarker measurements for predicting PE requiring delivery before 37 weeks and to compare the performance of ML models with the FMF algorithm using both internal and external validation.
Materials and methods
Study design
A retrospective multicenter cohort study was conducted to develop and externally validate prognostic models for pPE. The reporting structure complies with the TRIPOD recommendations (type 2b) [18]. The study was approved by the local ethics committee (Petrozavodsk State University; Protocol No. 18, dated March 20, 2024). Owing to the retrospective design and use of de-identified data, informed consent was not required for this study.
Cohorts
The development cohort was derived from the multicenter scientific pregnancy registry MARS (Modeling Obstetric Risk and Stratification), which integrates retrospective data from medical institutions in five regions of the Russian Federation (Kirov, Omsk, and Chelyabinsk regions; the Republic of Bashkortostan; and the Yamalo-Nenets Autonomous Okrug). Cases were enrolled consecutively from 2011 to 2025. Of the 24,247 records, 7,101 observations were selected after applying the inclusion and exclusion criteria (Appendix, Section P1), including 133 cases of pPE (1.87%).
The external validation cohort was formed from data obtained from medical institutions in the Republic of Karelia that were not involved in the creation of the MARS Registry. Of the 3,668 records, 1,325 observations were included using analogous criteria, including 24 cases of pPE (1.81%).
The inclusion criteria were as follows: singleton pregnancy; maternal age ≥18 years; registration for antenatal care and completion of first-trimester screening (11+0 to 13+6 weeks of gestation); availability of data on first- and second-trimester biophysical and biochemical markers (MAP, UtAPI, and PlGF); and delivery at an institution participating in the registry.
The exclusion criteria were as follows: multiple pregnancies; delivery before 22+0 weeks of gestation (nonviable fetus); missing >50% of biomarker data in either the first or second trimester; and absence of information on gestational age at delivery or discharge diagnosis.
Outcome
The primary outcome was pPE, defined as the development of PE according to the ISSHP 2018 criteria [1], followed by delivery before 37 weeks of gestation.
Predictors
The analysis included 15 maternal factors (demographic, anthropometric, and anamnestic variables), as well as biomarkers measured in the first trimester (11⁺⁰–13⁺⁶ weeks) and second trimester (19⁺⁰–23⁺⁶ weeks): mean arterial pressure (MAP), uterine artery pulsatility index (UtAPI), and placental growth factor (PlGF). Biomarker values were converted into multiples of the median (MoM) with covariate adjustment using FMF equations [8, 19] and then log₁₀-transformed. A full list of the predictors, measurement methods, and conversion procedures is provided in the Appendix (Section P2).
Prognostic models
Four models were developed: ML M2 (logistic regression; 15 maternal factors + 3 first-trimester biomarkers), ML M4 (ML M2 + 3 second-trimester biomarkers), FMF T1, and FMF T2 (Bayesian competing-risks algorithm [7] using published parameters [17, 19] without recalibration).
The biomarker sets were identical for the ML and FMF approaches in each trimester.
The choice of logistic regression was motivated by the requirements for calibrated probabilities, interpretability and reproducibility. The number of events per predictor (EPV) was 7.4 for M2 and 6.3 for M4; with adequate validation, an EPV ≥5–8 is considered acceptable for logistic regression [20]. The AUC optimism for model M4 was 0.030, and the calibration slope was 0.973, indicating no evidence of substantial overfitting in the model.
Validation
The ML models were internally validated using stratified 10-fold cross-validation. External validation was conducted by training on the full development cohort and applying the models to the validation cohort without any parameter modification. FMF models were applied to both cohorts using published parameters.
Statistical analysis
Discrimination was assessed using the area under the curve (AUC) with 95% confidence intervals (CI) (DeLong method), and paired comparisons were performed using the DeLong test for correlated curves. Calibration was evaluated comprehensively using the O:E ratio, calibration slope and intercept, Brier score, and calibration curves (LOESS) [21]. Reclassification was assessed using continuous NRI and IDI [22]. The clinical utility was evaluated using decision curve analysis (DCA) [23]. The high-risk threshold was defined as ≥1:100 (FIGO) [10]. The 95% confidence intervals (CIs) were calculated using bootstrap resampling (2,000 replicates). The significance level was set at p<0.05; in sensitivity analyses with Bonferroni correction (α=0.0125), all major conclusions remained the same. Equivalence in discrimination between ML M4 and FMF T2 was confirmed using the two one-sided tests (TOST) procedure (±0.03 AUC; both p<0.01). Missing values were imputed using the Hot-Deck Nearest Neighbor method. The details of the statistical procedures are provided in the Appendix (Section P3).
FMF risk calculations were performed using the “Preeclampsia batch risk assessment” tool (fetalmedicine.org). The analysis was conducted using R 4.3 (packages: pROC, rms, dcurves, nricens) and Python 3.11 (scikit-learn, statsmodels).
Results
Cohort characteristics
The clinicodemographic characteristics of the cohorts are presented in Supplementary Table S1 (Appendix). The incidence of preterm preeclampsia (pPE) was 1.87% (internal cohort) and 1.81% (external cohort), and the difference was not statistically significant (p=0.88). Pregnant women with pPE were characterized by a higher body mass index, greater prevalence of chronic arterial hypertension, and a history of preeclampsia (all p<0.001). Biomarkers from both trimesters differed significantly between the groups, with differences increasing from the first to the second trimester, reflecting the progressive nature of placental dysfunction.
Discriminative performance
The discrimination results are presented in Table 1 and Figure 1.
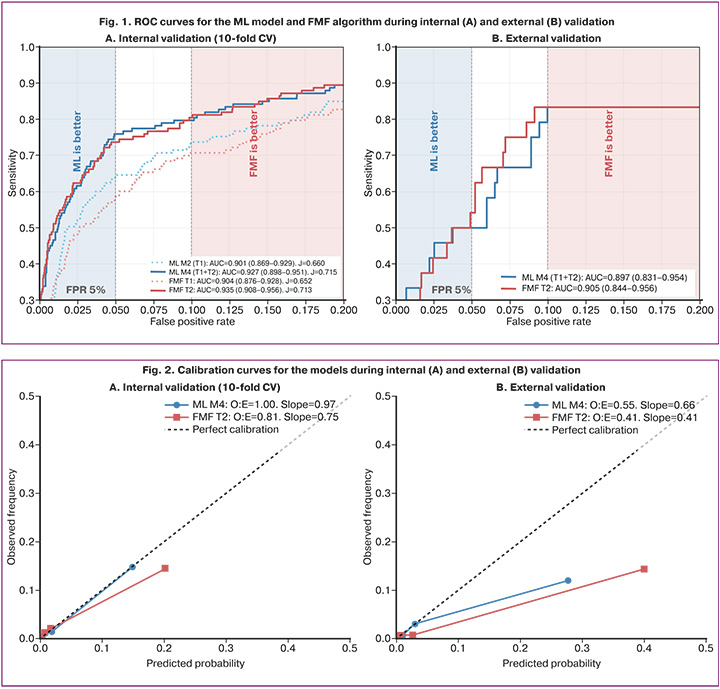
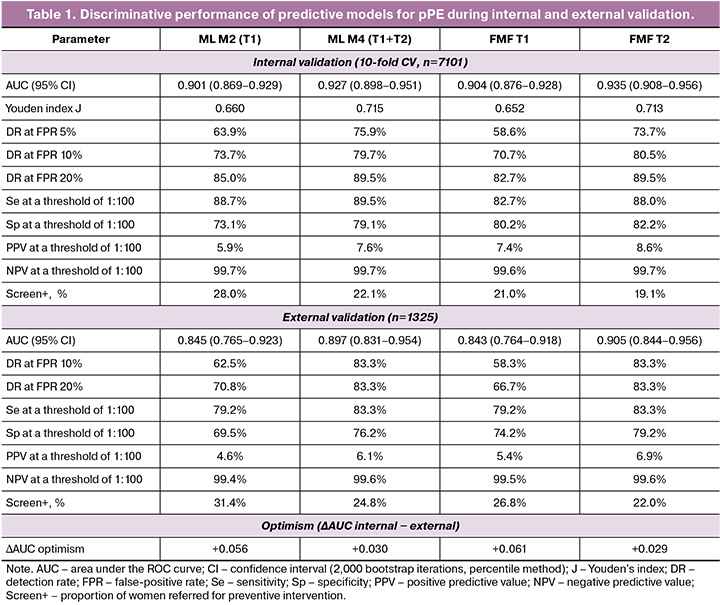
First-trimester models demonstrated comparable discrimination: AUC ML M2 = 0.901 (95% CI 0.869–0.929) and FMF T1 = 0.904 (0.876–0.928); p=0.62. The addition of second-trimester data significantly improved discrimination: ΔAUC = +0.025 (p=0.001) for the ML model and +0.031 (p<0.001) for the FMF algorithm. Second-trimester models were equivalent with respect to discrimination: AUC ML M4 = 0.927 and FMF T2 = 0.935 (ΔAUC = -0.008; p=0.91; two one-sided tests [TOST], p<0.01). At a risk threshold of 1:100, the detection rates (DR) were 89.5% (ML M4) and 88.0% (FMF T2), with screen-positive rates of 22.1% and 19.1%, respectively.
Calibration
The calibration metrics are presented in Table 2 and Figure 2.
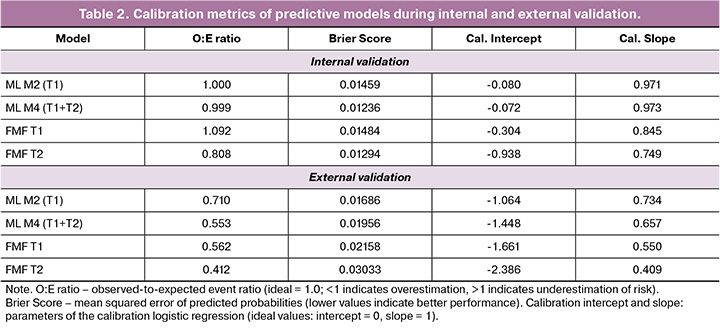
During internal validation, the ML models demonstrated near-ideal calibration (O:E ratio ML M4 = 0.999; calibration slope = 0.973). The FMF T2 algorithm systematically overestimated risk: O:E = 0.808 (slope = 0.749), indicating that the predicted probabilities exceeded the observed event rates by a mean of 24%. Calibration curves corroborated this pattern: for ML M4, the LOESS curve coincided with the diagonal reference line, whereas for FMF T2, it deviated below the diagonal, most notably within the clinically relevant probability range of 1–5% (Fig. 2).
Reclassification and clinical utility
The categorical net reclassification improvement (NRI) at a threshold of 1:100 was +0.068 (ML) and +0.072 (FMF), and the integrated discrimination improvement (IDI) was +0.115 and +0.214, respectively, confirming the additional prognostic value conferred by the second-trimester data. Reclassification was safe, with a proportion of correct downward risk reclassifications of 99.7% and 99.4% for the transition from first-to second-trimester models for (ML) and 99.4% (FMF). Concurrently, second-trimester data enabled the additional identification of three (ML) and ten (FMF) pPE cases that were previously classified as low-risk. A detailed reclassification analysis is provided in the Appendix (Supplementary Tables S4–S5).
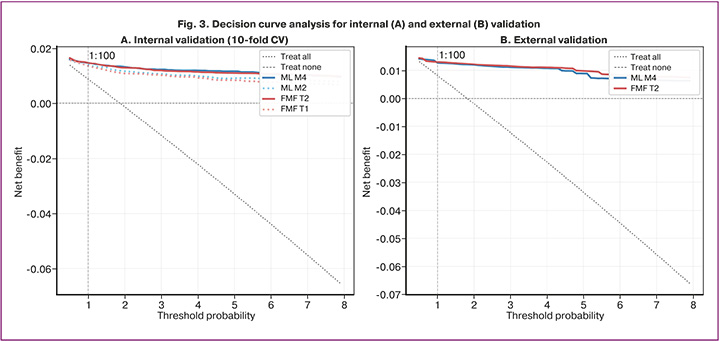
Decision curve analysis (Fig. 3) demonstrated that all models outperformed both the "treat all" and "treat none" strategies across the threshold range of 0.5–5%. The net benefit of ML M4 and FMF T2 at a threshold of 1:100 was nearly identical (0.01469 and 0.01471, respectively), which, assuming timely initiation of acetylsalicylic acid therapy, translates to the identification of approximately six additional pPE cases per 1,000 women screened compared with a strategy of universal aspirin administration.
External validation
Discrimination was maintained at an acceptable level: AUC ML M4 = 0.897 (0.831–0.954) and FMF T2 = 0.905 (0.844–0.956); optimism was +0.030 and +0.029, respectively. The added prognostic value of the second-trimester data was reproduced: the DR at a 10% FPR increased from 62.5% and 58.3% (first-trimester models) to 83.3% for both second-trimester models. The calibration hierarchy was preserved: ML models were better calibrated than the FMF algorithm (O:E ML M4 = 0.553 vs. FMF T2 = 0.412). The expected degradation in calibration observed in the external cohort is an anticipated phenomenon when a model is applied to an independent population [11, 13].
Discussion
The central finding of the present study is the FMF calibration paradox: an algorithm that was acceptably calibrated for first-trimester screening in a cohort of Russian women systematically overestimated risk when second-trimester data were added, whereas the ML model retained near-perfect calibration. Simultaneously, both strategies are equivalent in terms of discrimination and clinical utility, and reclassification within a two-stage screening framework is safe.
The gain in discrimination achieved by adding second-trimester data is consistent with the findings of the FMF group (detection rate increased from 75% to 85% at a 10% false-positive rate) [17] and the PRESIDE study (detection rate 88%) [24]. The somewhat smaller absolute effect observed in our cohort (detection rate up to 80.5%) may be explained by differences in the population structure. The biological rationale lies in the fact that second-trimester biomarkers reflect established placental dysfunction after the completion of spiral artery remodeling [16, 25]. Notably, when transitioning from model M2 to M4, the predictive contribution of first-trimester PlGF and UtAPI was almost completely replaced by their second-trimester counterparts (Appendix, Table P2), suggesting not an additive accumulation of information but rather the replacement of a less mature signal with a more mature one.
Given equivalent discrimination, the choice between the two approaches was determined by calibration. The nonlinear calibration dynamics of the FMF algorithm –acceptable for T1 (O:E = 1.09) but impaired for T2 (O:E = 0.81) – constitute one of the most important observations of this study. The underlying mechanism is likely related to the multiplicative amplification of systematic error during the sequential application of likelihood ratios; if the MoM distributions in the study cohort deviate from the reference distributions, repeated application cumulatively increases the mismatch. Clinically, this means that the use of uncorrected FMF T2 risk for individual counseling would lead to a systematic overestimation of risk. In contrast, ML models trained on local data are not subject to this limitation and can be updated as new observations accumulate [26, 27]. In addition, the asymmetry of reclassification is noteworthy: ML is more effective in appropriately downgrading false-positive cases, whereas FMF is more effective in identifying additional pPE cases, a difference attributable to the calibration properties of the models.
Limitations. The retrospective design and analysis of complete cases constitute the principal limitations of this study; the proportion of excluded observations was 30.5% in the internal cohort. The number of events in the external cohort (n=24) limits the power of the calibration assessment, for which the recommended minimum is ≥100 events [20]. The absence of systematic data on the prescription of acetylsalicylic acid is another important limitation. The available information (approximately 40% of observations) suggests an increase in aspirin prescriptions after 2018, which may have affected the calibration without altering the comparative conclusions. The degradation of calibration across all models during external validation (O:E 0.41–0.71) underscores the need for recalibration when transferring models to a new population. The use of cross-validation rather than temporal splitting represents an additional limitation, given the 14-year recruitment period. The set of maternal factors included in the ML models did not fully match the expanded FMF feature set (in particular, smoking data were unavailable), which formally placed ML at a disadvantage; the achievement of equivalent discrimination despite this indirectly supports the compensatory role of local calibration.
These findings support the need for prospective validation of a two-stage screening protocol, including an assessment of its impact on clinical outcomes, the development of recalibration equations for FMF T2, and an evaluation of cost-effectiveness. The logistic regression model represents a fixed formula that can be implemented in a medical information system or a web-based calculator. The MARS registry may serve as a platform to accomplish these objectives.
Conclusion
The measurement of second-trimester biomarkers (MAP, UtAPI, and PlGF) provides a statistically significant improvement in the prediction of PE requiring delivery before 37 weeks in a cohort of Russian women. A logistic regression–based ML model and the FMF algorithm, when using data from both trimesters, achieved equivalent discrimination (AUC>0.92) and clinical utility; however, the ML model demonstrated substantially superior calibration, which is critical for individualized counseling. Risk reclassification within a two-stage screening strategy is safe (>99% correct downgrades). These findings provide a rationale for the prospective evaluation of a two-stage pPE screening protocol using locally trained models.
Appendices
The supplementary materials (Tables P1–P7, Figures P1–P6 and the statistical analysis details) are available online at: https://doi.org/10.5281/zenodo.19223173
References
- Brown M.A., Magee L.A., Kenny L.C., Karumanchi S.A., McCarthy F.P., Saito S. et al. The hypertensive disorders of pregnancy: ISSHP classification, diagnosis & management recommendations for international practice. Pregnancy Hypertens. 2018; 13: 291-310. https://dx.doi.org/10.1016/j.preghy.2018.05.004
- Ходжаева З.С., Холин А.М., Вихляева Е.М. Ранняя и поздняя преэклампсия: парадигмы патобиологии и клиническая практика. Акушерство и гинекология. 2013; 10: 4-11. [Khodzhaeva Z.S., Kholin A.M., Vikhlyaeva E.M. Early and late preeclampsia: paradigms of pathobiology and clinical practice. Obstetrics and Gynecology. 2013; (10): 4-11 (in Russian)].
- Министерство здравоохранения Российской Федерации. Клинические рекомендации. Преэклампсия. Эклампсия. Отеки, протеинурия и гипертензивные расстройства во время беременности, в родах и послеродовом периоде. 2024. [Ministry of Health of the Russian Federation. Clinical guidelines. Preeclampsia. Eclampsia. Edema, proteinuria and hypertensive disorders during pregnancy, labor and the postpartum period. 2024 (in Russian)].
- Кан Н.Е., Беднягин Л.А., Долгушина Н.В., Тютюнник В.Л., Ховхаева П.А., Сергунина О.А., Тютюнник Н.В., Амирасланов Э.Ю. Клинико-анамнестические факторы риска развития преэклампсии у беременных. Акушерство и гинекология. 2016; 6: 39-44. [Kan N.E., Bednyagin L.A., Dolgushina N.V., Tyutyunnik V.L., Khovkhaeva P.A., Sergunina O.A., Tyutyunnik N.V., Amiraslanov E.Yu. Clinical and anamnestic risk factors for preeclampsia in pregnant women. Obstetrics and Gynecology. 2016; (6): 39-44. (in Russian)]. https://dx.doi.org/10.18565/aig.2016.6.39-44
- Rolnik D.L., Wright D., Poon L.C., O'Gorman N., Syngelaki A., de Paco Matallana C. et al. Aspirin versus placebo in pregnancies at high risk for preterm preeclampsia. N. Engl. J. Med. 2017; 377(7): 613-22. https://dx.doi.org/10.1056/NEJMoa1704559
- Roberge S., Nicolaides K., Demers S., Hyett J., Chaillet N., Bujold E. The role of aspirin dose on the prevention of preeclampsia and fetal growth restriction: systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2017; 216(2): 110-20.e6. https://dx.doi.org/10.1016/j.ajog.2016.09.076
- Wright D., Akolekar R., Syngelaki A., Poon L.C., Nicolaides K.H. A competing risks model in early screening for preeclampsia. Fetal Diagn. Ther. 2012; 32(3): 171-8. https://dx.doi.org/10.1159/000338470
- O'Gorman N., Wright D., Syngelaki A., Akolekar R., Wright A., Poon L.C. et al. Competing risks model in screening for preeclampsia by maternal factors and biomarkers at 11–13 weeks gestation. Am. J. Obstet. Gynecol. 2016; 214(1):103.e1-e12. https://dx.doi.org/10.1016/j.ajog.2015.08.034
- Wright D., Tan M.Y., O'Gorman N., Poon L.C., Syngelaki A., Wright A. et al. Predictive performance of the competing risk model in screening for preeclampsia. Am. J. Obstet. Gynecol. 2019; 220(2): 199.e1-e13. https://doi.org/10.1016/j.ajog.2018.11.1087
- Poon L.C., Shennan A., Hyett J.A., Kapur A., Hadar E., Divakar H. et al. The International federation of gynecology and obstetrics (FIGO) initiative on pre-eclampsia: a pragmatic guide for first-trimester screening and prevention. Int. J. Gynaecol. Obstet. 2019; 145(Suppl. 1): 1-33. https://dx.doi.org/10.1002/ijgo.12802
- Tiruneh S.A., Vu T.T.T., Moran L.J., Callander E.J., Allotey J., Thangaratinam S. et al. Externally validated prediction models for pre-eclampsia: systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2024; 63(5): 592-604. https://dx.doi.org/10.1002/uog.27490
- Холин А.М., Муминова К.Т., Балашов И.С., Ходжаева З.С., Боровиков П.И., Иванец Т.Ю., Гус А.И. Прогнозирование преэклампсии в первом триместре беременности: валидация алгоритмов скрининга на российской популяции. Акушерство и гинекология. 2017; 8: 74-84. [Kholin A.M., Muminova K.T., Balashov I.S., Khodzhaeva Z.S., Borovikov P.I., Ivanets T.Yu., Gus A.I. First-trimester prediction of preeclampsia: Validation of screening algorithms in a Russian population. Obstetrics and Gynecology. 2017; (8): 74-84 (in Russian)]. https://dx.doi.org/10.18565/aig.2017.8.74-84
- Ranjbar A., Montazeri F., Ghamsari S.R., Mehrnoush V., Roozbeh N. Machine learning models for predicting preeclampsia: a systematic review. BMC Pregnancy Childbirth. 2024; 24(1): 6. https://dx.doi.org/10.1186/s12884-023-06220-1
- Андрейченко А.Е., Лучинин А.С., Ившин А.А., Ермак А.Д., Новицкий Р.Э., Гусев А.В. Разработка и валидация моделей прогнозирования общего риска преэклампсии и риска ранней преэклампсии с использованием алгоритмов машинного обучения в первом триместре беременности. Акушерство и гинекология. 2023; 10: 94-107. [Andreychenko A.E., Luchinin A.S., Ivshin A.A., Ermak A.D., Novitskiy R.E., Gusev A.V. Development and validation of models to predict total and early-onset preeclampsia in the first trimester of pregnancy using machine learning algorithms. Obstetrics and Gynecology. 2023; (10): 94-107 (in Russian)]. https://dx.doi.org/10.18565/aig.2023.101
- Ившин А.А., Малышев Н.А. Ранняя стратификация риска преэклампсии на основе мультипараметрической модели машинного обучения и рутинных клинических данных. Акушерство, гинекология и репродукция. 2026; 20(1): 111-29. [Ivshin A.A., Malyshev N.A. Early preeclampsia risk stratification based on a multiparametric machine learning model and routine clinical data. Obstetrics, Gynecology and Reproduction. 2026; 20(1): 111-29 (in Russian)]. https://dx.doi.org/10.17749/2313-7347/ob.gyn.rep.2025.706
- Ходжаева З.С., Коган Е.А., Клименченко Н.И., Акатьева А.С., Сафонова А.Д., Холин А.М., Вавина О.В., Сухих Г.Т. Клинико-патогенетические особенности ранней и поздней преэклампсии. Акушерство и гинекология. 2015; 1: 12-7. [Khodzhaeva Z.S., Kogan E.A., Klimenchenko N.I., Akatyeva A.S., Kholin A.M., Vavina O.V., Sukhikh G.T. Clinical and pathogenetic features of early and late preeclampsia. Obstetrics and Gynecology. 2015; (1): 12-7 (in Russian)].
- Gallo D.M., Wright D., Casanova C., Campanero M., Nicolaides K.H. Competing risks model in screening for preeclampsia by maternal factors and biomarkers at 19–24 weeks' gestation. Am. J. Obstet. Gynecol. 2016; 214(5): 619.e1-e17. https://dx.doi.org/10.1016/j.ajog.2015.11.016
- Collins G.S., Reitsma J.B., Altman D.G., Moons K.G. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): the TRIPOD statement Ann. Intern. Med. 2015; 162(1): 55-63. https://dx.doi.org/10.7326/M14-0697
- Wright D., Syngelaki A., Akolekar R., Poon L.C., Nicolaides K.H. Competing risks model in screening for preeclampsia by maternal characteristics and medical history. Am. J. Obstet. Gynecol. 2015; 213(1): 62.e1-e10. https://dx.doi.org/10.1016/j.ajog.2015.02.018
- Riley R.D., Ensor J., Snell K.I.E., Harrell F.E., Martin G.P., Reitsma J.B. et al. Calculating the sample size required for developing a clinical prediction model. BMJ. 2020; 368: m441. https://dx.doi.org/10.1136/bmj.m441
- Van Calster B., McLernon D.J., van Smeden M., Bottolo L., Timmerman D., Steyerberg E.W. Calibration: the Achilles heel of predictive analytics. BMC Med. 2019; 17(1): 230. https://dx.doi.org/10.1186/s12916-019-1466-7
- Pencina M.J., D'Agostino R.B. Sr., D'Agostino R.B. Jr., Vasan R.S. Evaluating the added predictive ability of a new marker: from area under the ROC curve to reclassification and beyond. Stat. Med. 2008; 27(2): 157-72. https://dx.doi.org/10.1002/sim.2929
- Vickers A.J., Elkin E.B. Decision curve analysis: a novel method for evaluating prediction models. Med. Decis. Making. 2006; 26(6): 565-74. https://dx.doi.org/10.1177/0272989X06295361
- Riishede L., Wright A., Wright D., Petersen O.B., Nicolaides K.H. Evaluation of second-trimester screening for preterm pre-eclampsia by maternal factors and biomarkers in a Danish population: the PRESIDE study. Ultrasound Obstet. Gynecol. 2023; 62(5): 651-8. https://dx.doi.org/10.1002/uog.26274
- Холин А.М., Ходжаева З.С., Гус А.И. Патологическая плацентация и прогнозирование преэклампсии и задержки роста плода в первом триместре. Акушерство и гинекология. 2018; 5: 12-9. [Kholin A.M., Khodzhaeva Z.S., Gus A.I. Pathological placentation and prediction of preeclampsia and intrauterine growth restriction in the first trimester. Obstetrics and Gynecology. 2018; (5): 12-9 (in Russian)]. https://dx.doi.org/10.18565/aig.2018.5.12-19
- Ившин А.А., Багаудин Т.З., Гусев А.В. Прогнозирование преэклампсии с использованием технологий искусственного интеллекта. Акушерство, гинекология и репродукция. 2021; 15(5): 576-85. [Ivshin A.A., Bagaudin T.Z., Gusev A.V. Prediction of preeclampsia using artificial intelligence technologies. Obstetrics, Gynecology and Reproduction. 2021; 15(5): 576-85 (in Russian)]. https://dx.doi.org/10.17749/2313-7347/ob.gyn.rep.2021.229
- Ivshin A.A., Boldina Yu.S., Gusev A.V., Shtykov A.S., Vasilev A.S. Artificial intelligence on guard of reproductive health. Ad Alta, Journal of Interdisciplinary Research. 2022; 12(02): 325-9. https://dx.doi.org/10.33543/1202
Received 03.02.2026
Accepted 31.03.2026
About the Authors
Aleksandr A. Ivshin, PhD, Associate Professor, Head of the Department of Obstetrics and Gynecology, Dermatovenerology of the Medical Institute, Petrozavodsk State University, 31, Krasnoarmeyskaya str., Petrozavodsk, Republic of Karelia, 185035, Russia, +7(909)567-12-51, scipeople@mail.ru, https://orcid.org/0000-0001-7834-096XYuliya S. Boldina, Senior Lecturer at the Department of Obstetrics, Gynecology, Dermatovenereology of the Medical Institute, Petrozavodsk State University, 31, Krasnoarmeyskaya str., Petrozavodsk, Republic of Karelia, 185035, Russia; Obstetrician-Gynecologist, Republican Perinatal Center named after K.A. Gutkin, Petrozavodsk, +7(981)405-85-24, ulia.isakova94@gmail.com, https://orcid.org/0000-0002-1450-650X
Nikita A. Malyshev, PhD Student in the scientific specialty «Information-Measuring and Control Systems», Lecturer, Department of Family Medicine, Public Health, Healthcare Management, Life Safety, Disaster Medicine, Petrozavodsk State University, 31, Krasnoarmeyskaya str., Petrozavodsk, Republic of Karelia, 185035, Russia, +7(921)461-38-60, malyshev.nikita.2016@gmail.com, https://orcid.org/0009-0005-2722-5976
Corresponding author: Alexander A. Ivshin, scipeople@mail.ru
Similar Articles

