
Diagnostic and predictive significance of standardized placental weight and birth weight percentiles for gestational age
Rodionov V.E., Zarubin E.A., Nichiporov A.I., Tiumeneva E.A., Chernov I.A., Kirillov Yu.A.
Objective. To develop gender-specific distribution of placental weight percentiles based on newborn’s birth weight and gestational age, perform preliminary analysis of influencing factors and assess the possibility of using these percentiles as regional standards.
Materials and methods. A retrospective analysis of 2039 cases of singleton pregnancy was performed. The following parameters were analyzed: newborn’s weight and height, placental weight, newborn’s gender, gestational age, maternal age and weight, parity. The Kolmogorov–Smirnov test was used to check the quantitative variables for normal distribution. The Mann–Whitney U test was used to compare independent groups. Spearman’s rank correlation coefficient was used to assess the strength of relationship between two ranked variables. The main product of the study consists of percentile standards, which were calculated using statistical modeling.
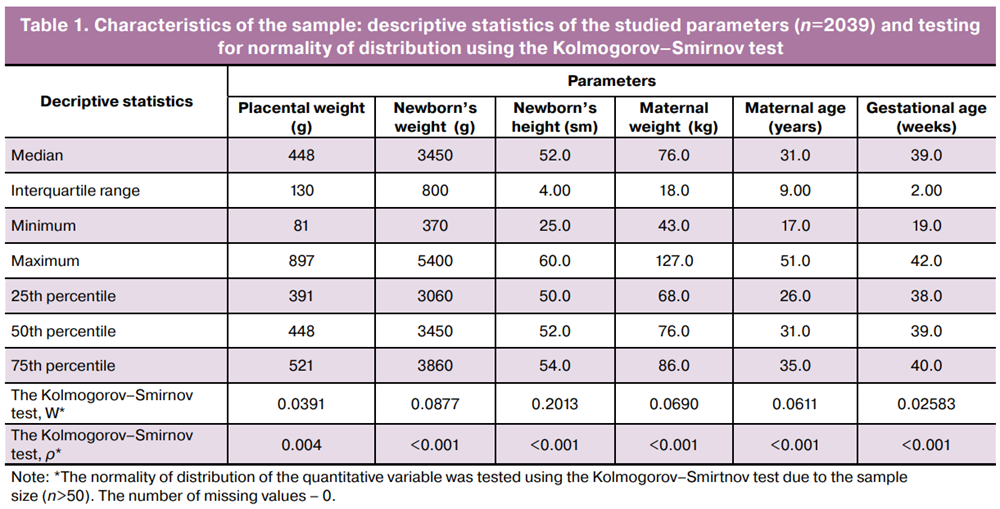
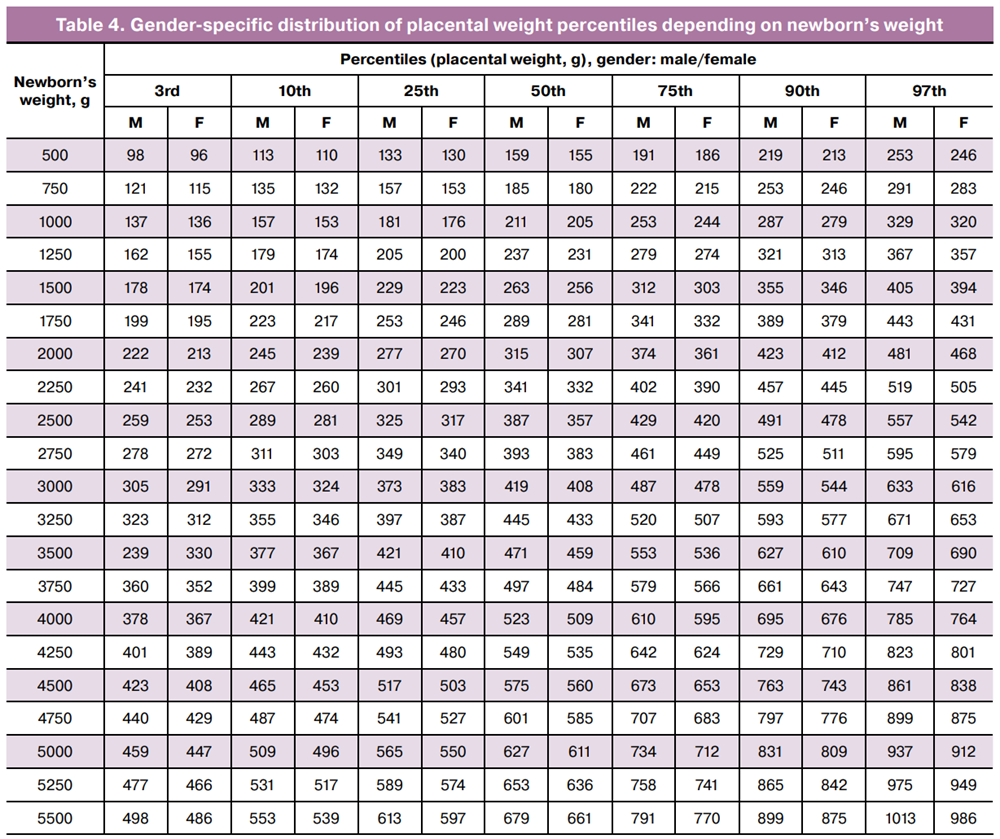
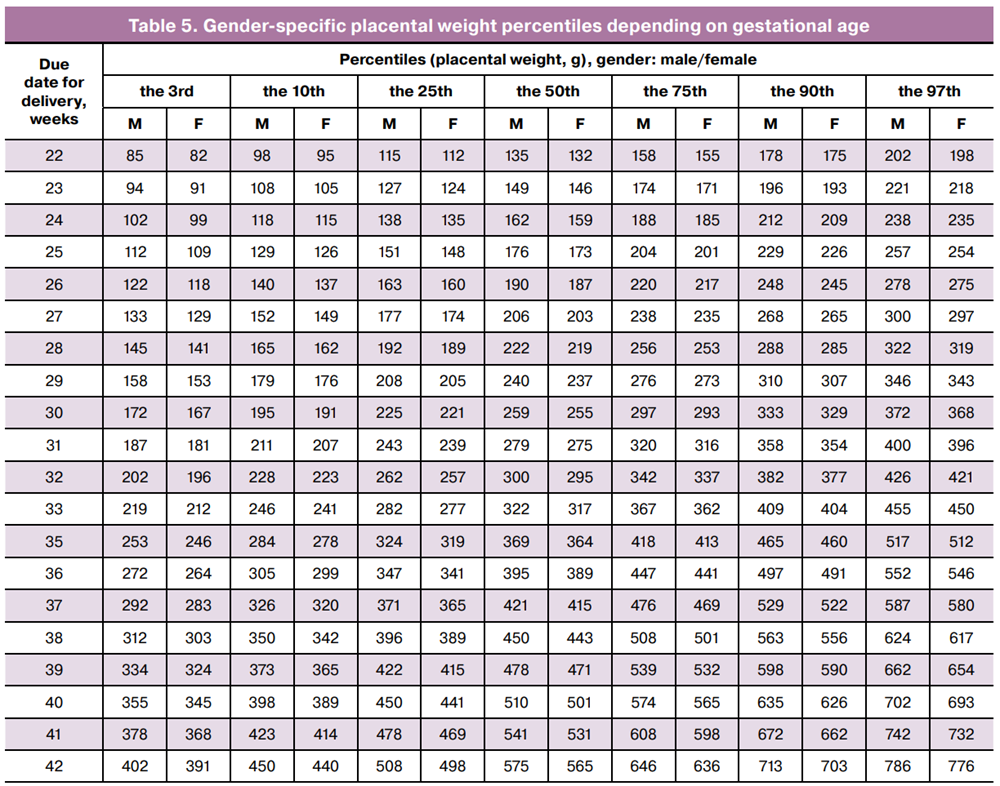
Results. The median weight of newborns was 3450 g (interquartile range (IQR) 3060–3860 g). The median gestational age was 39 weeks (IQR 38–40 weeks). Correlation analysis confirmed strong relationship between newborn’s weight and height (ρ=0.901; p<0.001), as well as between newborn’s weight and placental weight (ρ=0.716; p<0.001). As a result of statistical modeling, the tables of percentiles were created (the 3rd, 10th, 50th, 90 and 97th percentiles) reflecting distribution of placental weight based on newborn’s weight and gestational age.
Conclusion. The developed gender-specific standardized placental weight percentiles represent an instrument for standardized placental assessment. Implementation of standardized placental weight percentiles into clinical practice will contribute to more objective diagnostics, improve early detection of risks associated with placental dysfunction, and provide improved personalized approach to management of pregnancy.
Authors' contributions. Rodionov V.E., Kirillov Yu.A., Chernov I.A. – the study concept and design; Rodionov V.E., Zarubin E.A., Nichiporov A.I., Tiumeneva E.A. – material collection and processing; Rodionov V.E. – statistical data processing; Rodionov V.E., Kirillov Yu.A. – manuscript writing; Zarubin E.A., Kirillov Yu.A., Chernov I.A. – manuscript editing.
Conflicts of interest. The authors have no conflicts of interest to declare that are related to publication of this article.
Funding. The study was carried out without any sponsorship.
Ethical Approval. The study was approved by the local Ethics Committee of Moscow Multidisciplinary Clinical Center “Kommunarka” of Moscow Healthcare Department (protocol No. 6 of August 08, 2023).
Authors' Data Sharing Statement. The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Rodionov V.E., Zarubin E.A., Nichiporov A.I., Tiumeneva E.A., Chernov I.A., Kirillov Yu.A. Diagnostic and predictive significance of standardized placental weight and birth weight percentiles for gestational age.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (5): 71-77 (in Russian)
https://dx.doi.org/10.18565/aig.2026.32
Keywords
placental weight
fetal weight
newborn’s weight
fetal length
newborn’s height
standardized percentiles
placental morphometry
prenatal diagnosis
placenta
The placenta is a transient organ acting as a functional and physiological interface between the fetus and mother. This multifunctional biological module provides ideal conditions for the development of new organism and performs a broad range of functions including trophic, gas exchange, endocrine, immune and adaptive functions [1]. Placental weight is one of the integral indicators reflecting the effectiveness of function of the placenta and the mother-placenta-fetus system [2, 3]. In clinical practice morphometric assessment of the placenta including placental weight remains the most available and informative diagnostic method, both in postnatal and intranatal pathological evaluation.
Due to the diagnostic significance, the development and application in clinical practice of accurate reference values for placental weight and correlation with other morphometric parameters of the fetus, newborn and mother is of particular importance. [4]. Significant deviations from normal placental weight may indicate serious pathologies, such as preeclampsia and uteroplacental insufficiency in case of placental hypoplasia (placental weight below the 10th percentile), or gestational diabetes mellitus in case of placental hyperplasia (placental weight greater than the 90th percentile) [5]. According to the theory of fetal programming (D.J.P. Barker), abnormal placental weight can have long-term consequences: low birth weight is associated with placental hypoplasia and increases the risk of developing hypertension and metabolic syndrome in adulthood; the development of obesity and cognitive impairment in the child are associated with placental hyperplasia [6].
Analysis of global experience in using percentile curves showed multiple limiting factors for their use in specific regions. Key problematic issues include significant ethnic differences (placental weight in the Asian population is on average significantly lower than in the North America population) [7]), social and economic factors influencing placental mass (availability of food, quality of healthcare, development of modern technologies), and time factors (the use of old reference values, which were actual 20–30 years ago, without taking into account the influence of modern trends, such as increasing obesity in specific regions, the development and prevalence of in vitro fertilization techniques) [8].
In modern obstetric and anatomic pathology practice, the fetal/placental ratio (FPR) remains widely used to assess the morphofunctional state of the placenta. However, the use of FPR has several limitations, one of which is absence of personalized approach that does not take into account the individual morphometric parameters of the newborn and placenta (for example, FPR for newborn’s low birth weight and low placental weight will be within the normal range masking potential problems) [9].
The purpose of the study was to develop gender-specific distribution of placental weight percentiles based on newborn’s birth weight and gestational age, perform preliminary analysis of influencing factors, and assess the possibility of using placental weigh percentiles as regional standards.
Materials and methods
A descriptive study was conducted based on retrospectively collected data from medical records containing information about 2039 cases of singleton pregnancies for the period from 01.01.2024 to 01.09.2025 at Perinatal Center of Moscow Multidisciplinary Clinical Center «Kommunarka» of Moscow Healthcare Department. The sample size (n=2039) provided sufficient statistical power to identify apriori specified clinically significant effects, as well as to apply statistical smoothing and modeling methods and create stable percentile tables. The database included the following parameters: placental weight (g), newborn’s weight (g), height (cm) and gender, maternal weight (kg) and age (years), due date for delivery (weeks), and parity.
Inclusion criteria included singleton pregnancy, gestational age from 22 to 42 weeks, the availability of complete anthropometric, morphometric and clinical data.
Exclusion criteria included multiple pregnancy fetal or neonatal death, absence of data about placental or newborn’s weight.
The protocol of the study was considered and approved by the local Ethics Committee of Moscow Multidisciplinary Clinical Center «Kommunarka» of Moscow Healthcare Department (protocol No. 6 of August 08, 2023).
Statistical analysis
Statistical data analysis was performed using Jamovi 2.6.26 open and free statistical software (the Jamovi Project (2024). The primary data analysis included descriptive statistics, testing for normality of data distribution using the Kolmogorov–Smirnov test, correlation analysis using Spearman’s rank correlation coefficient for non-normal distribution, and comparison of independent groups using the nonparametric Mann–Whitney U test. For comparative analysis, the following groups were formed: gender-based groups included male group and female group of newborns; maternal parity groups included the groups of primiparous women and multiparous women, as well as the subgroups depending on birth order (first, second, third, etc.).
A combined approach was used to create the tables of percentiles. Calculation of the 3rd, 10th, 25th, 50th, 75th, 90th, 97th percentiles for gestational age and weight categories with a sufficient number of observations (n≥10) was based on empirical data. Statistical smoothing methods were used for categories with a small number of observations (n<10) and included cubic spline interpolation to obtain smooth percentile curves; second-order polynomial regression to model non-linear growth of placental weight depending on the newborn’s weight and gestational age; the weighted moving average with assigning different weights proportional to the sample size in each category; linear extrapolation based on regression coefficients for extremely low gestational age and weight of the newborn. Regression modeling was performed separately for male and female newborns.
Results
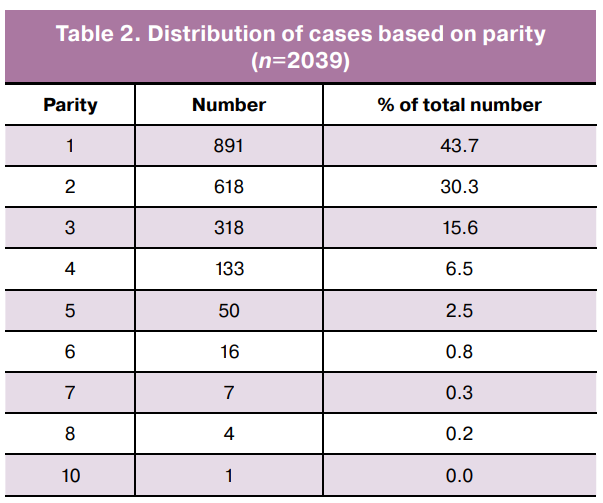
Descriptive statistics was used summarize the characteristics of the sample (Tables 1, 2). Testing for normality of data distribution using the Kolmogorov–Smirnov test showed non-normal distribution for all parameters. For this reason, the quantitative variables were presented as the median and interquartile range. The qualitative variables were presented as absolute numbers and percentages.
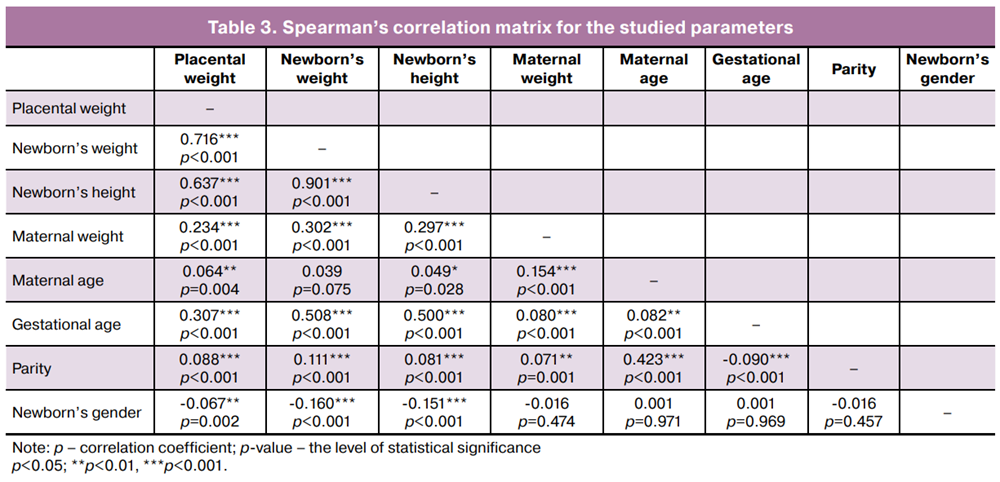
Correlation analysis was performed to assess the relationship between the studied quantitative parameters (placental weight, newborn’s weight and height, maternal weight and age, gestational age, and parity) and the binary variable (newborn’s gender). Since the data distribution was non-normal, the non-parametric Spearman rank correlation coefficient was used (Table 3).
Comparison of newborn’s weight depending on gender was performed using the non-parametric Mann–Whitney U test. Analysis showed statistically significant differences between the groups (U=421 707, p<0.001): male newborns weighed significantly greater compared with female newborns.
Based on data analysis, gender-specific percentile tables of placental weight depending on newborn’s weight (Table 4) and gestational age (Table 5) were created. The percentile curves (3rd, 10th, 25th, 50th, 75th, 90th, 97th) were built separately for male and female newborns.
Discussion
The characteristics of the study sample corresponded to the typical population parameters for full-term and early-term pregnancies in the developed countries (the median birth weight 3450 g, the median gestational age 39.0 weeks). It should be noted that a significant variation of the parameters, especially birth weight from 370 g to 5400 g and gestational age from 19 to 42 weeks indicated that cases with severe fetal growth restriction and extreme prematurity, as well as cases of macrosomia and postmaturity have been included in analysis [10].
The predominance of primiparous women (891/2039 (43.7%)) in the structure of parity reflected the general demographic trend. However, a significant percentage of multiparous women, who gave birth the second and third time – 936/2039 (45.9%) made it possible to appropriately assess the influence of this factor on the studied parameters of the fetoplacental system. A small proportion of women with high parity (≥4) was consistent with the general epidemiological trend. Careful interpretation of the statistics is required for these groups due to a small subsample size [11].
The results of correlation analysis confirmed the key physiological relationship between the parameters of fetoplacental system. A very strong correlation between the newborn's weight and height (ρ=0.901) indicated their synchronous development. The high correlation between placental weight and the newborn's weight and height (ρ=0.716 and ρ=0.637, respectively) emphasized the principal function of the placenta to supply the fetus with nutrients and to sustain the growth of the fetus, that is consistent with the concept of the fetoplacental unit [2, 3]. The absence of direct significant correlation between maternal age and newborn’s weight (p=0.075) could indicate a nonlinear or indirect relationship [12]. The validity of the developed gender-specific tables of percentiles for placental weight depending on neonatal weight and gestational age was ensured by table construction method that combined direct empirical calculation of the percentiles for the categories with sufficient volume of data and statistical modeling for rare categories. This approach allowed to eliminate random fluctuations inherent in empirical data, ensure smoothness and biological plausibility of the standards, as well as extrapolate the percentile values to the zones with insufficient data coverage (the 3rd, 97th percentiles, extremely low and high weight of newborns, extremely preterm birth), that is consistent with the modern standards for constructing normative curves, and increases the clinical applicability of these tables of percentiles [13, 14].
Conclusion
Thus, introduction of gender-specific standardized placental weight percentiles into clinical practice will contribute to standardization of placental assessment, improve early detection of risks associated with placental dysfunction, and ultimately, promote improved personalized management of pregnancy. The standardized placental weight percentiles will make it possible to switch from assessment of absolute placental weight to analysis of its conformity with the individual characteristics of the given pregnancy, that will improve the accuracy in diagnosing uteroplacental insufficiency or placentomegaly.
References
- Burton G.J., Fowden A.L. The placenta: a multifaceted, transient organ. Phil. Trans. R. Soc. B. 2015; 370(1663): 20140066. https://dx.doi.org/10.1098/rstb.2014.0066
- Щеголев А.И., Серов В.Н. Клиническая значимость поражений плаценты. Акушерство и гинекология. 2019; 3: 54-62. [Shchegolev A.I., Serov V.N. Clinical significance of placental lesions. Obstetrics and Gynecology. 2019; (3): 54-62 (in Russian)]. https://dx.doi.org/10.18565/aig.2019.3.54-62
- Колобов А.В. Методические особенности морфологического исследования плаценты, внеплацентарных оболочек и пуповины при инфекционной патологии. Архив патологии. 2024; 86(5): 53-9. [Kolobov A.V. Methodological approaches to the morphological study of placenta, extraplacental membranes and umbilical cord in infectious pathology. Russian Journal of Archive of Pathology. 2024; 86(5): 53-9 (in Russian)]. https://dx.doi.org/10.17116/patol20248605153
- Nicholls V., Nye E.B. The influence of maternal factors on placental weight. N. Z. Med. J. 1980; 91(661): 426-30.
- Baptiste-Roberts K., Salafia C.M., Nicholson W.K., Duggan A., Wang N.Y., Brancati F.L. Maternal risk factors for abnormal placental growth: The national collaborative perinatal project. BMC Pregnancy Childbirth. 2008; 8(1): 44. https://dx.doi.org/10.1186/1471-2393-8-44
- Barker D.J.P. The fetal and infant origins of disease. Eur. J. Clin. Invest. 1995; 25(7): 457-63. https://dx.doi.org/10.1111/j.1365-2362.1995.tb01730.x
- Rutherford J.N., deMartelly V., Ragsdale H.B., Avila J.L., Lee N.R., Kuzawa C.W. Global population variation in placental size and structure: Evidence from Cebu, Philippines. Placenta. 2019; 85: 40-8. https://dx.doi.org/10.1016/j.placenta.2019.08.076
- Papageorghiou A.T., Kennedy S.H., Salomon L.J., Altman D.G., Ohuma E.O., Stones W. et al. The INTERGROWTH-21st fetal growth standards: toward the global integration of pregnancy and pediatric care. Am. J. Obstet. Gynecol. 2018; 218(2S): S630-40. https://dx.doi.org/10.1016/j.ajog.2018.01.011
- Hayward C.E., Lean S., Sibley C.P., Jones R.L., Wareing M., Greenwood S.L. et al. Placental adaptation: what can we learn from birthweight: placental weight ratio? Front. Physiol. 2016; 7: 28. https://dx.doi.org/10.3389/fphys.2016.00028
- Kiserud T., Benachi A., Hecher K., Perez R.G., Carvalho J., Piaggio G. et al. The World Health Organization fetal growth charts: concept, findings, interpretation, and application. Am. J. Obstet. Gynecol. 2018; 218(2S): S619-29. https://dx.doi.org/10.1016/j.ajog.2017.12.010
- Vollset S.E., Goren E., Yuan C.W., Cao J., Smith A.E., Hsiao T. et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020; 396(10258): 1285-306. https://dx.doi.org/10.1016/s0140-6736(20)30677-2
- Kozuki N., Lee A.C., Silveira M.F., Sania A., Vogel J.P., Adair L. et al. The associations of parity and maternal age with small-for-gestational-age, preterm, and neonatal and infant mortality: a meta-analysis. BMC Public Health. 2013; 13(S3): S2. https://dx.doi.org/10.1186/1471-2458-13-s3-s2
- Cole T.J., Green P.J. Smoothing reference centile curves: the LMS method and penalized likelihood. Statistics in Medicine. 1992; 11(10): 1305-19. https://dx.doi.org/10.1002/sim.4780111005
- Rigby R.A., Stasinopoulos D.M. Generalized additive models for location, scale and shape. Journal of the Royal Statistical Society Series C. 2005; 54(3): 507-54. https://dx.doi.org/10.1111/j.1467-9876.2005.00510.x
Received 02.02.2026
Accepted 09.04.2026
About the Authors
Vladimir E. Rodionov, Pathologist, Moscow Multidisciplinary Clinical Center «Kommunarka», Moscow City Healthcare Department, 108814, Russia, Moscow,Sosenskoye village, Kommunarka village, Sosensky Stan str., 8, build. 3, TiNAO; Lecturer at the Department of Pathological Anatomy and Forensic Medicine, Tyumen State Medical University, Ministry of Health of Russia, 625023, Russia, Tyumen, Odesskaya str., 54, +7(916)323-88-24, rodionov.ve@mail.ru, https://orcid.org/0000-0003-0842-4169
Egor A. Zarubin, PhD, Pathologist, Moscow Multidisciplinary Clinical Center «Kommunarka», Moscow City Healthcare Department, 108814, Russia, Moscow,
Sosenskoye village, Kommunarka village, Sosensky Stan str., 8, build. 3, TiNAO, +7(916)019-00-30, zarubean@gmail.com, https://orcid.org/0000-0002-2548-9506
Andrey I. Nichiporov, Laboratory Research Assistant, Moscow Multidisciplinary Clinical Center «Kommunarka», Moscow City Healthcare Department, 108814, Russia, Moscow, Sosenskoye village, Kommunarka village, Sosensky Stan str., 8, build. 3, TiNAO, andrei.ni4iporov@yandex.ru, https://orcid.org/0009-0006-6895-5278
Evgeniia A. Tiumeneva, Pathologist, Moscow Multidisciplinary Clinical Center «Kommunarka», Moscow City Healthcare Department, 108814, Russia, Moscow,
Sosenskoye village, Kommunarka village, Sosensky Stan str., 8, build. 3, TiNAO, +7(916)232-22-60, eugenie.tyumenev@yandex.ru, https://orcid.org/0009-0001-0338-7453
Igor A. Chernov, PhD, Associate Professor, Head of the Department of Pathological Anatomy and Forensic Medicine, Tyumen State Medical University, Ministry of Health of the Russia, 625023, Russia, Tyumen, Odesskaya str., 54, Chernov@tyumsmu.ru, https://orcid.org/0000-0002-6475-5731
Yuri A. Kirillov, Dr. Med. Sci., Professor, Pathologist, Moscow Multidisciplinary Clinical Center «Kommunarka», Moscow City Healthcare Department, 108814, Russia, Moscow, Sosenskoye village, Kommunarka village, Sosensky Stan str., 8, build. 3, TiNAO; Professor, Department of Pathological Anatomy and Forensic Medicine, Tyumen State Medical University, Ministry of Health of Russia, 625023, Russia, Tyumen, Odesskaya str., 54; Leading Researcher at the Clinical Morphology Laboratory, Research Institute of Human Morphology, 117418, Russia, Moscow, Tsyurupy str., 3, youri_kirillov@mail.ru, https://orcid.org/0000-0003-3555-0902
Corresponding author: Vladimir E. Rodionov, rodionov.ve@mail.ru
Similar Articles

