
Fetal adaptation to cardiotocography as a criterion of fetal condition
Aim. To investigate fetal adaptation profile during antenatal cardiotocography (CTG) with subsequent analysis of neonatal outcomes.Loginov V.V., Davydov D.G., Prikhod'ko A.M., Baev O.R., Degtyarev D.N.
Materials and methods. The retrospective study included 1927 observations at 33 to 40 weeks of gestation. Consecutive RR intervals were recorded using a UNICOS fetal computerized cardiac monitor. Heart rate variability (HRV) was assessed during the first 30 measurements. Based on cluster analysis, observations were divided into two groups categorized by fetal adaptation profiles as 1 [habituation, n=1702 (88.3%)] and 2 [dishabituation, n=225 (11.7%)]. The relationship between adaptation profiles and data on the early neonatal complications was analyzed.
Results. Fetal HRV analysis showed that in most cases, fetuses quickly adapted to the CTG and maintained parameters throughout the procedure. In the first group, the profile showed a decrease in RR interval variance with relatively low basal heart rate and fetal condition indicator (FCI). In the second group (newborns with complicated neonatal course), the profile was characterized by a high basal heart rate, high RR interval variance, and higher mean FCI. HRV changes during adaptation to the CTG were associated with complications identified in newborns.
Conclusion. Fetal HRV assessment during adaptation to CTG is essential for assessing the fetal condition and predicting the complicated neonatal course.
Keywords
habituations
cardiotocography
heart rate variability
The use of antenatal cardiotocography (CTG) to determine the fetal condition has significantly expanded the opportunities to diagnose intrauterine disorders. Non-invasive fetal cardiac activity monitoring allows identification of women with high risk pregnancies and, thereby, reduces perinatal morbidity and mortality rates [1]. At the same time, there are concerns regarding the interpretation of CTG results, particularly the overdiagnosis of fetal distress [2].
A fetal heartbeat may first be detected as early as 5 to 6 weeks after gestation. By this time, the myocardium contains a sufficient number of specialized pacemaker cells initiating and controlling cardiac contractions. Vagal parasympathetic and sympathetic fibers begin to penetrate the myocardium by 18 and 27 weeks of gestational age, respectively. The cardiac conduction system development completes by 32–33 weeks of gestation [3, 4]. The study of the fetus's cardiovascular system reflects not only its intrauterine oxygenation but also provides essential information about autonomic regulation of the cardiovascular system and the body as a whole.
Heart rate variability (HRV) is the variation in the time interval between heartbeats. A sequential series of cardio intervals (RR) has a complex structure reflecting various humoral factors' regulatory effect on the sinoatrial node [5]. As a result of fetal exposure to an external stimulus, the heart rate changes and stabilizes over some time due to habituation. Assessment of changes in HRV during this period is becoming increasingly important in the diagnosis of the fetal condition [6].
The present study aimed to investigate fetal adaptation profile during antenatal cardiotocography with subsequent analysis of neonatal outcomes.
Materials and methods
The study was conducted at the V.I. Kulakov NMRC for OG&P, Ministry of Health of Russia, affiliated to the Department of Obstetrics, Gynecology, Perinatology, and Reproductology, I.M. Sechenov First MSMU, Ministry of Health of Russia (Sechenov University). This retrospective study analyzed 1927 CTGs that were antenatally recorded using a UNICOS fetal computerized cardiac monitor in 2018–2019. Of them, 1195 (62%) were recorded in patients who gave birth at the Center. Among infants born to them, 42 (3.5%) newborns had neonatal period complications. The study inclusion criteria were singleton pregnancy at 33–40 weeks, no clinical or laboratory signs of fetal distress, and fetal condition index (FCI) ≤1.05. Study exclusion criteria were fetal disorders, FCI> 1.05. The baseline data consisted of successive measurements of 2500–6600 RR intervals (16–60 minutes). During CTG registration, the pregnant woman was placed on a couch, and the sensors were fixed at the points of the best signal during heart rate tracing. The signal was first monitored, and then recording was started, which lasted from 10 minutes to 1 hour and 20 minutes. The RR intervals variability was calculated as the standard deviation for each of 10 consecutive RR intervals, with a shift by one (from 1st to 10th, from 2nd to 11th, etc.). HRV was assessed during the first 30 measurements since later on it ceases to reflect the fetal response to external stimuli. Observations were divided into two groups categorized by fetal adaptation profiles as 1 [habituation, n=1753 (88.32%)] and 2 [dishabituation, n=232 (11.68%)] and neonatal disorders and neurosonographic findings were analyzed after birth.
Statistical analysis
Statistical analysis and plotting were performed using IBM SPSS 25 statistical software. The grouping of observations according to their similarity was carried out by cluster analysis using K-means based on the Euclidean distance. The number of clusters was determined using the Silhouette Index. The normality of the distribution was tested by the Kolmogorov–Smirnov test. Student’s t-test was used to test quantitative parameters between 2 independent groups with the normal distribution. Quantitative variables showing normal distribution were expressed as means and standard deviation, qualitative data as counts and percentages. Differences were considered statistically significant at p<0.05. The study was approved by the V.I. Kulakov NMRC for OG&P Research Ethics Committee.
Results
The patients' age and gestational age ranged from 17 to 51 years (31.5) and 33 to 40 weeks (37.2), respectively. HRV analysis showed that at the beginning of CTG recording, the rate of RR intervals increased (during the first 30 intervals or 18 seconds), followed by a transition to the basal level, which does not change further during the subsequent recording (Fig. 1). Considering this observation, it was decided to analyze further even shorter CTG fragments (the first 30 measurements).
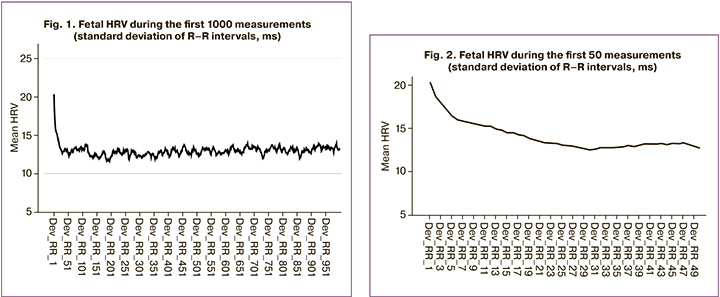
Figure 2 shows a fragment of the first 50 intervals, reflecting an increased HRV as a response of the fetus to external stimuli, followed by a decrease in the habituation type.
These findings convincingly show that in most cases, fetuses quickly adapt to the CTG and maintain parameters throughout the entire habituation.
At the next stage, all data were grouped using cluster analysis by the k-means method, which allowed optimal selection of two groups (Fig. 3). The determination of the number of clusters was carried out using the Silhouette Index, which exceeds 0.65, which is considered the right solution in terms of quality.
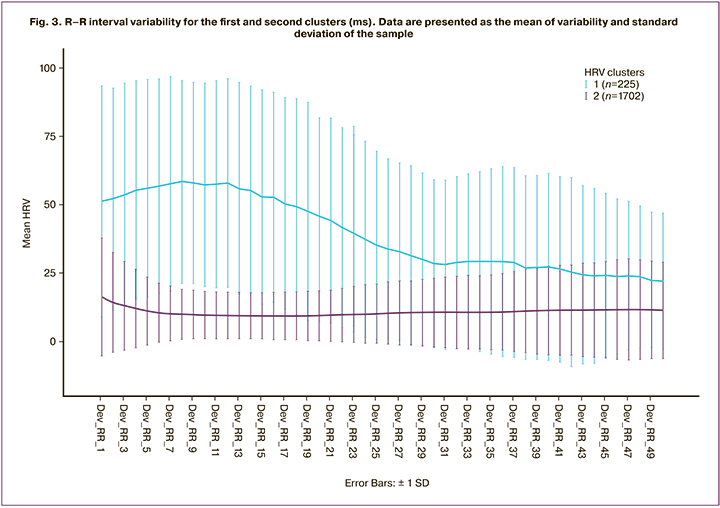
The first group included 1702 (88.3%) observations. It is characterized by an increased HRV at the beginning of the examination and a non-linear decrease during the first 20 intervals. The second group included 225 (11.7%) observations with a high HRV followed by an increase (up to 60 ms) and then a decrease by the 30th interval. Differences in HRV between clusters are significant in all the first 30 intervals (Student's t – 8.3 to 44.0, p≤0.001). At the same time, the total variability of the heart rate of the second group up to the 30th interval is almost three times higher than in the first group.
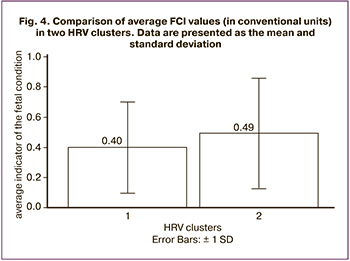 Comparison of the selected groups by the mean FCI value also showed that, although both groups meet the norm criterion (FCI 1.0), the second group has a higher FCI (t=4.125 p <0.05; Fig. 4).
Comparison of the selected groups by the mean FCI value also showed that, although both groups meet the norm criterion (FCI 1.0), the second group has a higher FCI (t=4.125 p <0.05; Fig. 4).
The analysis of 1927 observations showed two fetal profiles during the beginning of CTG registration. In the first group (habituation), the profile showed a regular decrease in the RR interval variance with a relatively low basal heart rate and a low average FCI. In the second group (dishabituation), the profile was characterized by a high level of basal heart rate and high RR interval variance, and increased mean FCI.
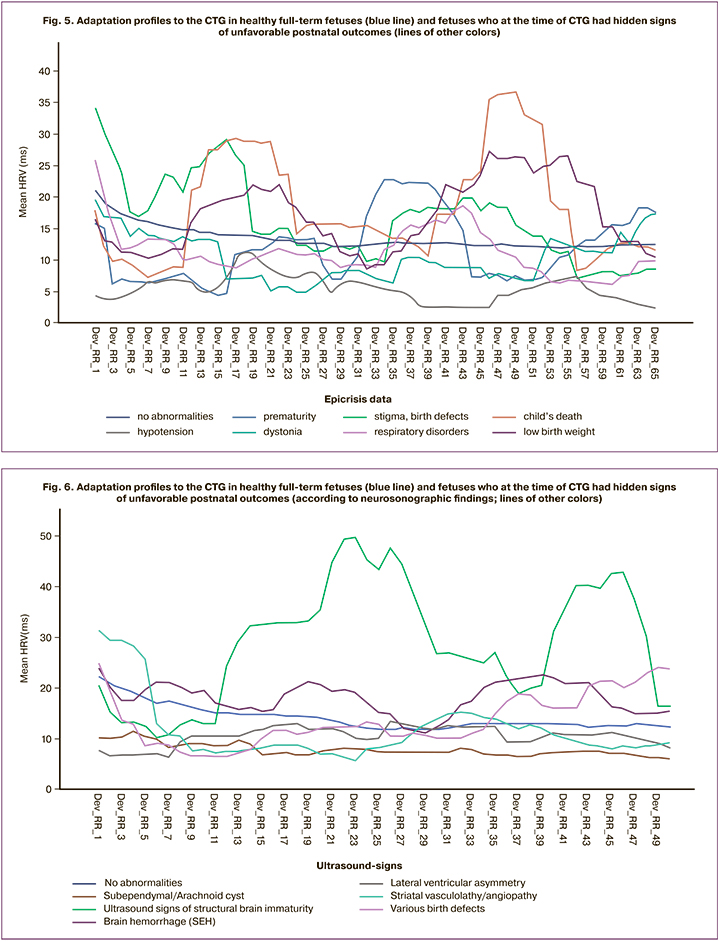
To assess the practical significance of the findings, the outcomes of labor in these patients were analyzed. The analysis included 1195 (62%) observations. Only 42 (3.5%) newborns had neonatal pathologies and/or developmental abnormalities. Figure 5 shows the HRV of fetuses that did not have developmental abnormalities after birth and preterm fetuses born with malformations, antenatal death, and those with a complicated early neonatal course. It was also noted that the HRV profile of fetuses who had normal postnatal neurosonographic findings differed from that in fetuses who postnatally were found to have changes in brain structures, including structural immaturity, hemorrhages, lateral ventricles asymmetry, subependymal or arachnoid cysts, and others (Fig. 6 ). It should be assumed that the difference from the adaptation profile to the CTG of healthy full-term fetuses may suggest the likelihood of an unfavorable postnatal outcome.
Therefore, characteristics of HRV at the beginning of antenatal CTG can be used to predict early neonatal complications. Although the number of observations in the group of unfavorable outcomes (n=42) is non-representative, these findings lead to a preliminary conclusion that dishabituation is associated with fetal development abnormalities.
Discussion
The CTG remains one of the objective methods of antenatal assessment of fetal wellbeing and early prediction of postnatal development disorders. In this study, 3.5% of newborns with normal CTG findings had postnatal disorders. The study demonstrated a steady increase in HRV at the initial stage of fetal adaptation to the CTG with its subsequent decrease. No interpretation of the functional significance of this phenomenon was found in the relevant literature. In our opinion, during the period of fetal adaptation to the CTG, the regulatory systems reorganize in the direction of basal heart rate stabilization according to the habituation type. Currently, this phenomenon is not considered when interpreting the test result. However, it may provide useful information about the fetal state [7–9].
Research into fetal habituation date back to the International Conference on Prenatal Psychology, held in Vienna in 1971, and is one of the recognized approaches to the study of perinatal development [10– 13]. Almost 50 years of research into fetal habituation to assess central nervous system functional state using vibroacoustic stimulation can become a standard procedure [6, 14]. At the same time, it is impossible to unambiguously separate the cognitive response during vibroacoustic stimulation (frequent blinking, turning the head towards the stimulus, opening the mouth, putting out the tongue, moving the cheeks, moving the arms to the head, and stretching the legs) from the stress response in the fetus. Differences between stress and cognitive responses have been clearly shown in the study of anencephaly. In such fetuses, the typical motor activity could be observed. Still, there was an almost complete absence of habituation, which is important for the formation of learning and memorizing mechanisms [15]. Further study of habituation showed a very high sensitivity of this phenomenon not only to morphological abnormalities of the fetal central nervous system but also to gestational age, mode of conception (natural or IVF), and partial oxygen pressure [6].
Our study used no vibroacoustic stimulation. However, a habituation-type response was observed in fetuses in natural conditions and in a familiar environment, which indicates regular changes in heart rate in the process of fetal adaptation to the CTG [15]. This study suggests that the habituation-type response to the stimulus can be realized under strict observance of two primary conditions, including the optimal basal fetal heart rate and neurophysiological maturity of the mechanisms related to homeostasis constancy.
Conclusion
The present study's findings showed that fetal HRV assessment during adaptation to CTG is essential for assessing the fetal condition and predicting the complicated neonatal course.
References
- Приходько А.М., Романов А.Ю., Евграфова А.В., Шуклина Д.А. Определение уровня pH и лактата крови из предлежащей части плода для оценки его состояния в родах. Вопросы гинекологии, акушерства и перинатологии. 2017; 16(6): 96-9. [Prikhodko А.М., Romanov A.Yu., Evgrafova A.V., Shuklina D.A. Detection of pH and blood lactate levels in the presenting part of the foetusfor evaluation of its status during labour. Questions of gynecology, obstetrics and perinatology. 2017; 16(6): 96-9. (in Russian)]. https://dx.doi.org/10.20953/1726-1678-2017-6-96-99.
- Еремина О.В., Баев О.Р., Приходько А.М., Шифман Е.М. Использование комбинации кардиотокографии и автоматического анализа сегмента ST электрокардиограммы плода для мониторинга его состояния в родах. Акушерство и гинекология. 2014; 11: 49-56. [Eremina O.V., Bayev O.R., Prikhodko A.M., Shifman E.M. Cardiotocography used in combination with automatic ST segment analysis of the electrocardiogram of a fetus for its status monitoring during labor and delivery. Akusherstvo i ginekologiya/ Obstetrics and Gynecology. 2014; 11: 49-56. (in Russian)].
- Christoffels V.M., Moorman A.F.M. Development of the сardiac сonduction system. Circ. Arrhythmia Electrophysiol. 2009; 2: 195-207. https://dx.doi.org/10.1161/CIRCEP.108.829341.
- Renou P., Newman W., Wood C. Autonomic control of fetal heart rate. Am. J. Obstet. Gynecol. 1969; 105(6): 949-53. https://dx.doi.org/10.1016/0002-9378(69)90103-3.
- Баевский Р.М., Берсенева А.П. Введение в донозологическую диагностику. М.: Слово; 2008. 174 с. [Baevskij R.M., Berseneva A.P. Introduction to prenosological diagnostics. M.: Slovo, 2008. 174 p. (in Russian)].
- Leader L.R. The potential value of habituation in the fetus. In: Reissland N., Kisilevsky B.S., eds. Fetal development: research on brain and behavior, environmental influences, and emerging technologies. Springer Int. Publ.; 2016: 189-209. https://dx.doi.org/10.1007/978-3-319-22023-9_11.
- Kuhlman K.A., Depp. R. Acoustic stimulation testing. Obstet. Gynecol. Clin. North Am. 1988; 15(1): 303-19.
- Westgren M., Almstrom H., Nymon M., Ulmsten U. Maternal perception of sound‐provoked fetal movements as a measure of fetal well‐being. Br. J. Obstet. Gynaecol. 1987; 94(6): 523-7. https://dx.doi.org/10.1111/j.1471-0528.1987.tb03144.x.
- Kuhlman K.A., Burns K.A., Depp R., Sabbagha R.E. Ultrasonic imaging of normal fetal response to external vibratory acoustic stimulation. Am. J. Obstet. Gynecol. 1988; 158(1): 47-51. https://dx.doi.org/10.1016/0002-9378(88)90773-9.
- Кочубей Б.И. В защиту эмпиризма. Вопросы психологии. 1989; 2: 68-72. [Kochubej B.I. In defense of empiricism. Questions of psychology. 1989; 2: 68-72. (in Russian)].
- Латаш Л.П. Гипоталамус, приспособительная активность и электроэнцефалограмма. М.; 1968. 294с. [Latash L.P. The hypothalamus, an adaptive activity and electroencephalogram. M.: 1968. 294p. (in Russian)].
- Соколов Е.Н. Очерки по психофизиологии сознания. М.: МГУ; 2010. 255с. [Sokolov E.N. Essays on the psychophysiology of consciousness. M.: 2010. 255p. (in Russian)].
- James D.K. Fetal learning: a critical review. Infant Child Dev. 2010. 19: 45-54. https://dx.doi.org/10.1002/icd.653.
- Ohel G., Birkenfeld A., Rabinowitz R., Sadovsky E. Fetal response to vibratory acoustic stimulation in periods of low heart rate reactivity and low activity. Am. J. Obstet. Gynecol.1986; 154(3): 619-21. https://dx.doi.org/10.1016/0002-9378(86)90612-5.
Received 08.10.2020
Accepted 19.10.2020
About the Authors
Viktor V. Loginov, Ph.D. (bio.sci.), Head of the Laboratory of Neurophysiology, V.I. Kulakov NMRC for OG&P, Ministry of Health Russia. Tel.: +7(495)316-13-75.E-mail: v_loginov@oparina4.ru. 117997, Russia, Moscow, Ac. Oparina str., 4.
Denis G. Davydov, Ph.D. (psychol.sci.), Associate professor, Open University of Economics, Management and Law. Tel.: +7(926)120-85-22. E-mail: dgdavydov19@gmail.com.
109029, Russia, Moscow, Nizhegorodskaya str., 32-4.
Andrey M. Prikhod'ko, Ph.D., Physician at the 1st Maternity Department, Teaching Assistant at the Department of Obstetrics and Gynecology, Researcher at the Department of Innovative Technologies, Institute of Obstetrics, V.I. Kulakov NMRC for OG&P, Ministry of Health Russia. Tel.: +7(495)438-30-47. E-mail: a_prikhodko@oparina4.ru.
4 Oparina str., Moscow, 117997, Russian Federation.
Oleg R. Baev, Dr. Med. Sci., Head of the Maternity Department, V.I. Kulakov NMRC for OG&P, Ministry of Health Russia; Professor at the Department of Obstetrics, Gynecology, Perinatology, and Reproductology, I.M. Sechenov First MSMU, Ministry of Health of Russia (Sechenov University). Tel.: +7(495)438-11-88.
E-mail: o_baev@oparina4.ru. 117997, Russia, Moscow, Ac. Oparina str., 4.
Dmitry N. Degtyarev, Dr. Med. Sci., Professor, Head of the Department of Neonatology, I.M. Sechenov First MSMU, Ministry of Health Russia (Sechenov University); Deputy Director, V.I. Kulakov NMRC for OG&P, Ministry of Health Russia. E-mail: glav_neolog@yahoo.com, d_degtiarev@oparina4.ru. 117997, Russia, Moscow, Ac. Oparina str., 4.
For citation: Loginov V.V., Davydov D.G., Prikhod'ko A.M., Baev O.R., Degtyarev D.N. Fetal adaptation to cardiotocography as a criterion of fetal condition.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2021; 3: 138-144 (in Russian)
https://dx.doi.org/10.18565/aig.2021.3.138-144
Similar Articles

