
Comparative analysis of clinical characteristics in Syrian women with uterine fibroids stratified by body mass index
Alali O.M., Khaddam W.M., Churnosov M.I.
Objective. To compare the clinical characteristics of Syrian women with uterine fibroid (UF) stratified by body mass index (BMI).
Materials and methods. 500 Syrian women with UF, ages 22–83, were included. They were split into three groups according to their BMI: 174 patients had BMI<25 kg/m2, 166 patients had BMI 25–29.99 kg/m2, and 160 patients had BMI≥30 kg/m2. A questionnaire of 65 items was used to gather data on the clinical characteristics and risk factors for the onset of UF. To analyze data was used SPSS version 30.
Results. Indicated that the rise in BMI of the participants was accompanied by a statistically significant increase in each of the age due to an increase in the proportion of women over 50 years of age, the elapsed time from the last birth, the number of births, the summary number of children, the usage an intrauterine device as a contraceptive method, and the incidence of hypertension, diabetes, and endometrial hyperplasia, moreover undergoing myomectomy and hysterectomy. While a statistically significant decrease was observed for the age at the first birth and age at first menstruation with a rise in BMI of these participants. The characteristics of fibromatous nodes in women with BMI 25–29.99 kg/m2 are their predominantly intramural location and large size, whereas in women with BMI<25 kg/m2 and BMI≥30 kg/m2, the nodes were mostly located subserosally and had smaller sizes. Similarly, women with BMI<25 kg/m2 often have pedunculated nodes and a combination of subserosal and intramural nodes, and women with BMI≥30 kg/m2 have submucosal nodes.
Conclusion. This study showed that Syrian women with different BMIs have distinct clinical characteristics of UFs. That will provide further insight into how they are affected by variations in BMI, and consequently, how these variations influence the risk and prevalence of UFs, which is helpful in their diagnosis, prevention, and symptom relief.
Authors' contributions. Alali O.M., Khaddam W.M., Churnosov M.I. – conception and design of the study; Alali O.M. – data collection and analysis, manuscript drafting; Churnosov M.I. – manuscript editing.
Conflicts of interest. The authors have no conflicts of interest to declare.
Funding. There was no funding for this study.
Ethical Approval. The study was reviewed and approved by the Research Ethics Committee of the Belgorod State National Research University.
Patient Consent for Publication. All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement. The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Alali O.M., Khaddam W.M., Churnosov M.I. Comparative analysis of
clinical characteristics in Syrian women with uterine fibroids stratified by body mass index.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (5): 121-132 (in Russian)
https://dx.doi.org/10.18565/aig.2025.335
Keywords
uterine fibroid
leiomyoma
body mass index
obesity
overweight
risk factor
The most common tumors in women are uterine fibroids (UF), also known as leiomyomas, which are benign tumors that grow from the uterine smooth muscle layer (myometrium) and are reliant on sex steroid hormones [1]. They affect 20–40% of women in their reproductive years [2], and have a lifetime frequency of 30–70% [3]. In the United States, UF is the leading cause of hysterectomy, accounting for billions of dollars in annual healthcare costs [4].
Obesity and overweight are significant variables influencing women's reproductive health [5, 6], and are regarded as the most prevalent disease predisposing factors [5–7]. Previous studies have shown that obesity increases the likelihood of endometrial polyps and symptomatic UFs in women's reproductive systems [8], and is a risk factor for the development of UF through a variety of molecular mechanisms [5–7].
There are several mechanisms that impact the link between obesity and the female reproductive system. One describes the endocrine reaction that happens when obesity increases the conversion of circulating androgens to estrogens, resulting in excess adipose tissue. Another mechanism, Obesity may elevate peripheral unbound estrogen levels by reducing the liver's production of sex hormone binding globulin (SHBG) [4, 5].
Other studies suggest that increasing weight after the age of 18 enhances the risk of having UF. However, one study found that women who are very overweight have a decreased chance of having UF [9]. Women who had their fibroids surgically removed had a higher waist-to-hip ratio (WHR) and body mass index (BMI), noticed to have a high frequency of several and larger UFs [10], and maintaining a healthy weight can help avoid UF [7, 11]. According to WHR, the obese body type had a higher frequency of irregular vaginal bleeding, multiple tumors, tumor degeneration, and lesion sizes of 40 mm than the normal body type group. The findings revealed that, independent of the type of obesity, an increase in peripheral adipose tissue is associated with a greater risk of UF [11]. BMI has been found to have a significant influence on fibroids growth. Women weighing 70 kg are three times more likely to have fibroids than those weighing 50 kg [12]. Moreover, a previous study found that visceral obesity increases the incidence of fibroids by promoting the creation of inflammatory mediators such as tumor necrosis factor-α (TNF-α) [6].
Several epidemiological studies have been undertaken to evaluate the association between obesity and the incidence of UF in premenopausal women, with inconsistent results [13–15]. Some studies identified a link between obesity and an increased incidence of UF [5, 15, 16]. While others found no significant correlation [13, 14].
Not all ethnic groups have a favorable link between a greater BMI and an increased risk of having fibroids [9, 17]. Case-control studies in China, Korea, and Japan found that greater BMI levels were associated with an increased risk of UF. One Japanese case-control research, however, revealed that greater odds of UF risk were associated with body fat percentage rather than BMI [13].
The characteristics of Asian women who may be more likely to develop UF are little known. There was just one study on Saudi women that found that obesity is a risk factor for Saudi women because it promotes the growth of UF [16]. Furthermore, the impact of obesity on the beginning and progression of UF is still largely unclear. Thus, in this study, we aimed to compare the clinical characteristics of Syrian women with UF stratified by BMI.
Materials and methods
A study was conducted in Syria between June 2023 and August 2024 in public and private hospitals in cities like Damascus, Hama, Tartus, Latakia, and Homs. These include Al-Ahli Private Hospital, Homs University Hospital, Latakia University Hospital, Tartus Maternity and Children's Hospital, and Latakia Maternity and Children's Hospital.
500 Syrian women with UFs, ages 22–83, were included in the study. They were split into three groups according to their body mass index (BMI): 174 patients had a BMI<25 kg/m2 (normal weight), 166 patients had a BMI 25–29.99 kg/m2 (overweight), and 160 patients had a BMI≥30 kg/m2 (obesity). Those born outside of Syria, women under the age of 20, and those of non-Syrian heritage were all excluded. After being informed of the purpose of the study, participants provided their informed consent. For the convenience of the participants, a 65-question questionnaire with yes/no categorical categories and multiple-choice questions (MCQ) translated into Arabic was developed to evaluate clinical characteristics and risk factors. The questionnaire's design was altered based on previously published studies.
Statistical analysis
Based on the BMI, we determined that a sample size of 500 patients was split into three groups: 174 patients had a BMI<25 kg/m2 (normal weight), 166 patients had a BMI 25–29.99 kg/m2 (overweight), and 160 patients had a BMI≥30 kg/m2 (obesity). Statistical analyses were achieved using jamovi 2.6.22 Debug. Continuous variables were checked out for normality using the Shapiro–Wilk test. Since all continuous variables demonstrated non-normal distributions (p<0.05), non-parametric tests were used throughout. Data are shown as median and interquartile range [Me (Q1; Q3)].
Comparisons among the three groups were conducted using the Kruskal–Wallis test for continuous and ordinal variables, and Chi-square test for categorical variables. As variables which significantly differences (p<0.05), we performed post-hoc pairwise comparisons between groups. For this pairwise comparison, we used chi-square test for binary categorical variables and Mann–Whitney test for continuous variables and variables with three or more categories.
When assessing the statistical significance of these differences, in order to reduce false positive results, we additionally introduced a Bonferroni correction accounting the number of pairwise compared groups (N=3) and a statistically significant level based on it was p<0.05/3≈0.017. The data were displayed as numbers or percentages of each participant for every qualitative attribute.
Results
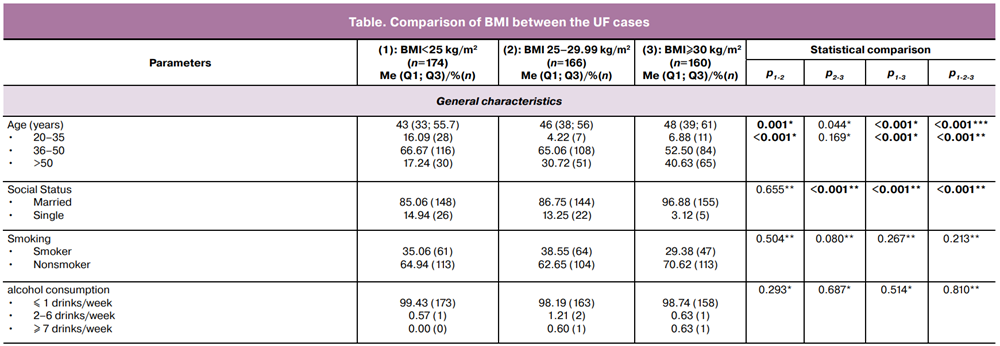
The study was performed on 500 Syrian women with UF, who ranged in age from 22 to 83, with the majority in the 36–50 age group, and were split into three groups according to their BMI: the first whose BMI<25 kg/m2 (174 patients), the second whose BMI 25–29.99 kg/m2 (166 patients), and the third whose BMI≥30 kg/m2 (160 patients).
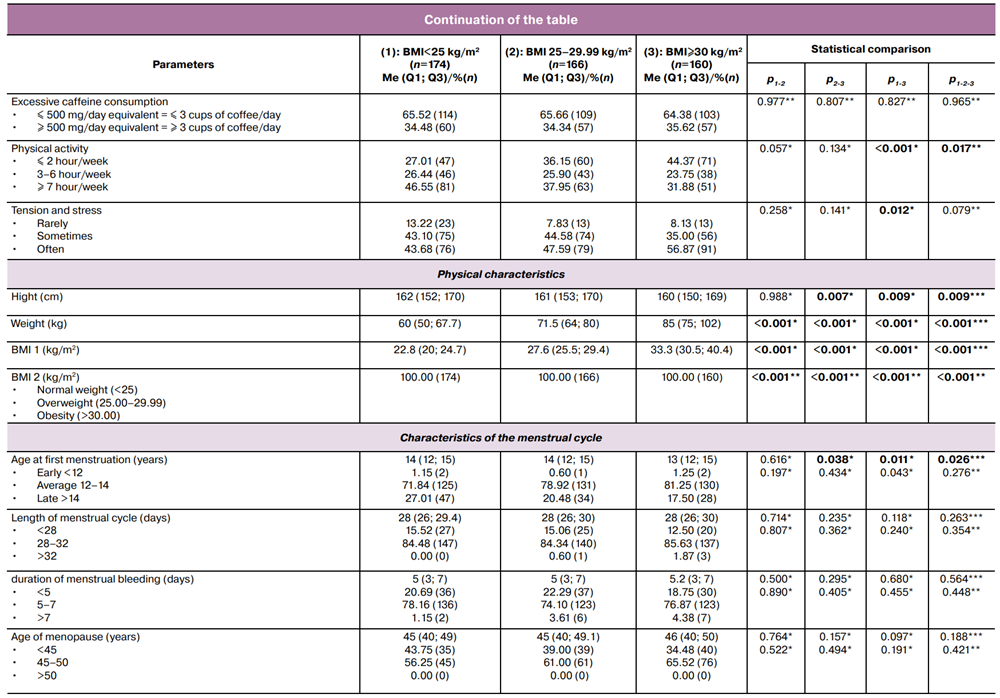
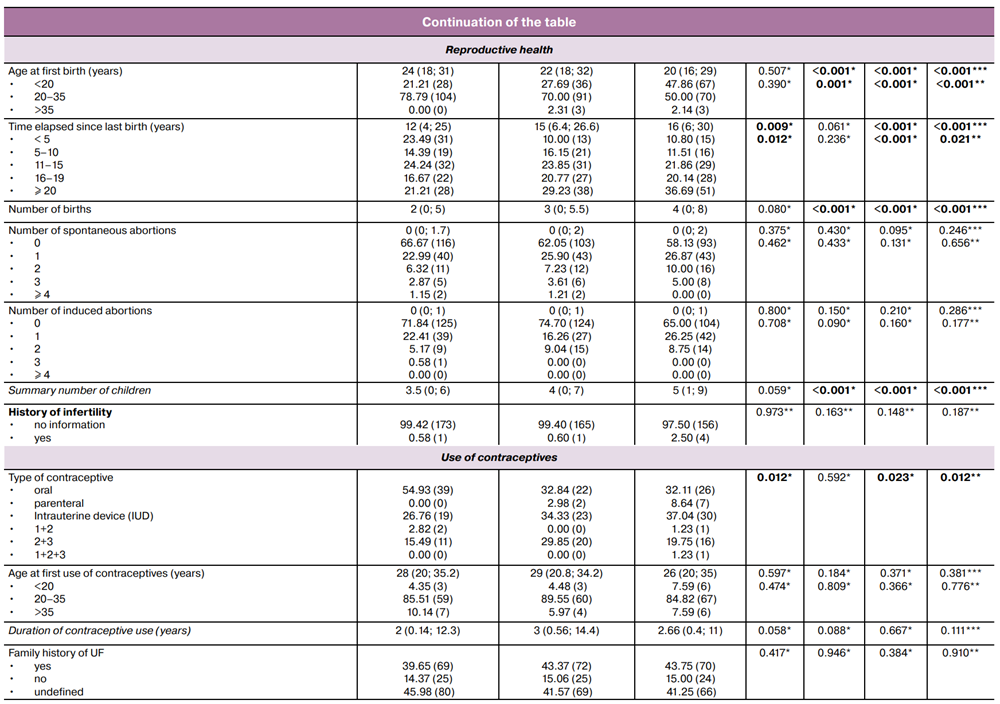
In patients with UF, with an increase in BMI, a higher average age was observed (43 (33; 55.7) years in patients with BMI<25 kg/m2, 46 (38; 56) years in patients with BMI 25–29.99 kg/m2, and 48 (39; 61) years in patients with BMI≥30 kg/m2, p<0.001), due to an increase in the proportion of women over 50 years of age (from 17.24% in patients with BMI<25 kg/m2 to 30.72% in patients with BMI 25–29.99 kg/m2 and 40.63% in patients with BMI ≥30 25 kg/m2, p<0.001), a lower average age at first menstruation (14 (12; 15) years in patients with BMI<25 kg/m2, 14 (12; 15) years in patients with BMI 25–29.99 kg/m2, and 13 (12; 15) years in patients with BMI ≥30 kg/m2, p=0.026), a lower average age at first birth (24 (18; 31) years in patients with BMI<25 kg/m2, 22 (18; 32) years in patients with BMI 25–29.99 kg/m2, and 20 (16; 29) years in patients with BMI≥30 kg/m2, p<0.001), due to the increase in the percentage of women under 20 years old at the time of their first birth (from 21.21% in patients with BMI<25 kg/m2 to 27.69% in patients with BMI 25–29.99 kg/m2 and 47.86% in patients with BMI≥30 kg/m2, p<0.001), a higher average time elapsed since the last birth (12 (4; 25) years in patients with BMI<25 kg/m2, 15 (6.4; 26.6) years in patients with BMI 25–29.99 kg/m2, and 16 (6; 30) years in patients with BMI≥30 kg/m2, p<0.001), due to the increase in the percentage of women who have had their last birth for ≥ 20 years (from 21.21% in patients with BMI<25 kg/m2 to 29.23% in patients with BMI 25–29.99 kg/m2 and 36.69% in patients with BMI≥30 kg/m2, p=0.021), a higher average number of births (2 (0; 5) years in patients with BMI<25 kg/m2, 3 (0; 5.5) years in patients with BMI 25–29.99 kg/m2, and 4 (0; 8) years in patients with BMI≥30 kg/m2, p<0.001), and thus a higher average summary number of children (3.5 (0; 6) years in patients with BMI<25 kg/m2, 4 (0; 7) years in patients with BMI 25–29.99 kg/m2, and 5 (1; 9) years in patients with BMI≥30 kg/m2, p<0.001). It was also noticed that a higher percentage of women who used intrauterine devices (IUDs) as a method of contraception (from 26.76% in patients with BMI<25 kg/m2 to 34.33% in patients with BMI 25–29.99 kg/m2 and 37.04% in patients with BMI≥30 kg/m2, p=0.012).
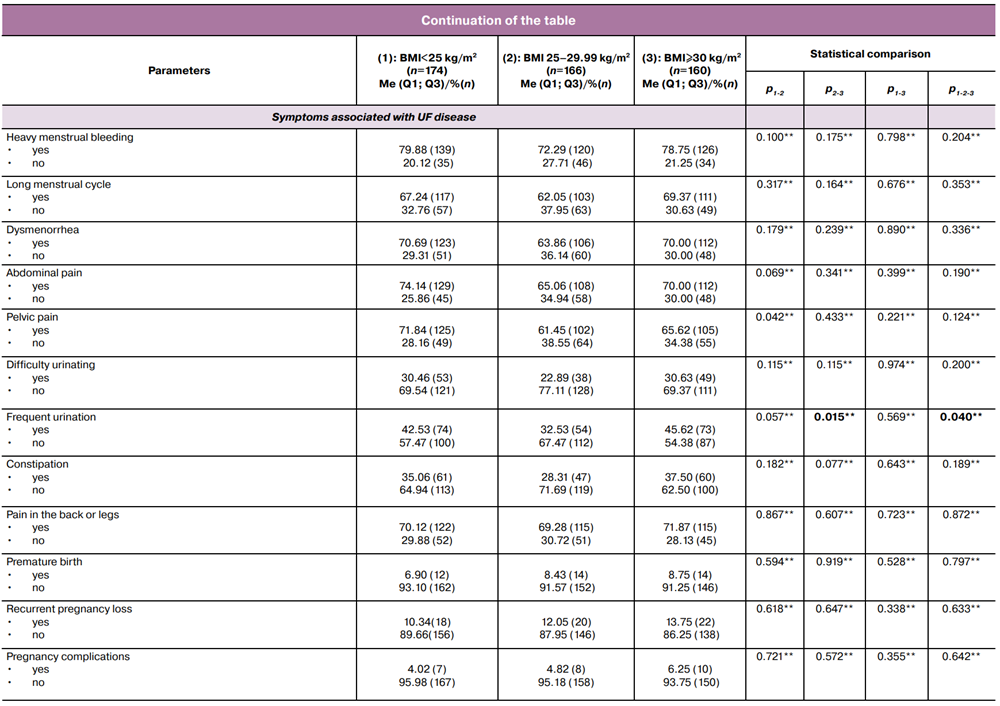
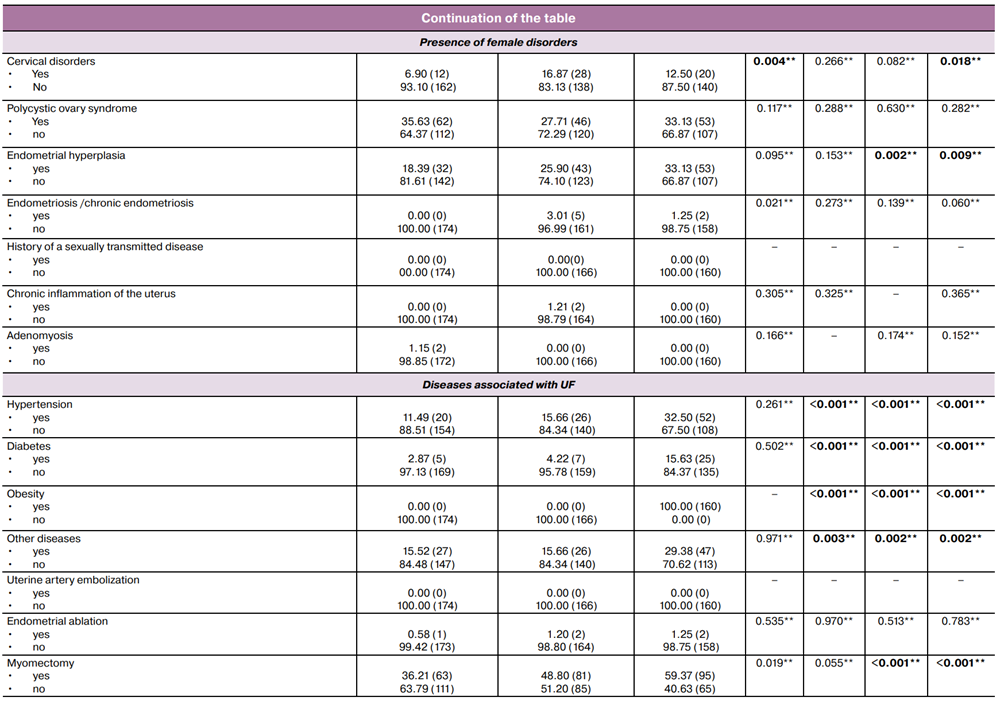
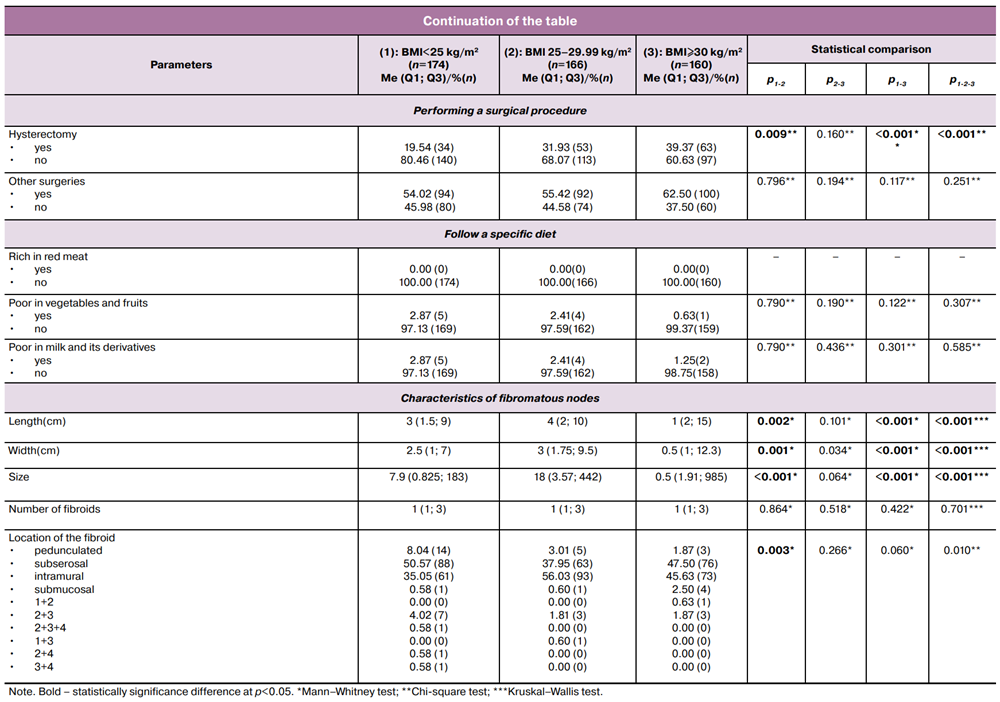
Furthermore, there has been an increase in the percentage of women suffering from hypertension (from 11.49% in patients with BMI<25 kg/m2 to 15.66% in patients with BMI 25–29.99 kg/m2 and 32.50% in patients with BMI≥30 kg/m2, p<0.001), diabetes (from 2.87% in patients with BMI<25 kg/m2 to 4.22% in patients with BMI 25–29.99 kg/m2 and 15.63% in patients with BMI≥30 kg/m2, p<0.001), and endometrial hyperplasia (EH) (from 18.39% in patients with BMI<25 kg/m2 to 25.90% in patients with BMI 25–29.99 kg/m2 and 33.13% in patients with BMI≥30 kg/m2, p=0.009). In addition to a higher percentage of women who underwent myomectomy (from 36.21% in patients with BMI<25 kg/m2 to 48.80% in patients with BMI 25–29.99 kg/m2 and 59.37% in patients with BMI≥30 kg/m2, p<0.001) and hysterectomy (from 19.54% in patients with BMI<25 kg/m2 to 31.93% in patients with BMI 25–29.99 kg/m2 and 39.37% in patients with BMI≥30 kg/m2, p<0.001).
In women with BMI 25–29.99 kg/m2, fibromatous nodes in most UF patients were located intramurally (56.03%) and had the largest size (18 (3.57; 442) cm3). Whereas in women with BMI<25 kg/m2 and BMI≥30 kg/m2, subserosal nodes were the most common (50.57% and 47.50%, respectively) and the size of the nodes was significantly smaller (7.9 (0.825; 183) cm3 and 0.5 (1.91; 985) cm3, respectively) than in UF patients with BMI 25–29.99 kg/m2. Similarly, in women with BMI<25 kg/m2, were found, with a fairly high frequency, pedunculated nodes (8.04%, which is 2.5–4 times more than in other analyzed patient groups), and a combination of subserosal and intramural nodes (4.02%, which is 2 times more than in other analyzed patient groups). At the same time, submucosal nodes were more than 4 times more common in UF patients with BMI≥30 kg/m2 (2.50%) compared with other studied groups (0.58–0.60%) (p=0.010), as shown in the table.
Discussion
The results of the present study concluded that there was statistical significance for a number of parameters in patients with UFs, with an increase in BMI, where a higher average age (p<0.001) was observed due to an increase in the proportion of women over 50 years of age. This was in line with results from earlier studies carried out on Saudi women by Moawad R. et al. [16], as well as with in Belgium and the United States, which suggested that 60% to 70% of women had one or more UFs by the age of 50 [18]. These studies attribute this to the accumulation of hormonal changes that occur in women during their reproductive years. One notable characteristic of UFs is their reliance on the ovarian hormones: progesterone and estrogen. It has been suggested by experimental and clinical research that progesterone and estrogen promote the development of UFs during the reproductive years [16, 19]. While it did not agree with a study conducted by Gürbüz T. et al., where they found no association between BMI and age [12].
A lower average age at first menstruation (p=0.026). The majority of research has demonstrated that an earlier menarche age raises the risk of UF [19]. Women who menarche early typically experience more menstruation throughout their lives, increasing their exposure to estrogens, which may encourage EH and cause UF to grow. Since the luteal phase of the menstrual cycle is when the myometrium's cell division rate is maximum, a longer history of cycling may raise the risk of UF. In the absence of progesterone, ongoing estrogen exposure appears to encourage the development of EH [20].
A lower average age at first birth (p<0.001), due to the increase in the percentage of women under 20 years old at the time of their first birth. Some studies have shown that older age at first birth is associated with a lower risk of developing UFs consistent with our results, unlike other studies [19].
A higher average time elapsed since the last birth (p<0.001), due to the increase in the percentage of women who have had their last birth for ≥ 20 years (p=0.021). This is consistent with the findings of the Stewart E.A. et al. study, which demonstrated that the risk of developing UFs was approximately two to three times higher for women who had given birth five years or more ago than for those who had given birth more recently in both the black and white populations [21]. Additionally, Nwonuma C et al. found that women who have just become pregnant are less likely to develop fibroids than those who have had births in the distant past [22]. Women with prior live births had a 20% to 50% reduced incidence of UF than nulliparous women [23].
A higher average number of births (p<0.001), and thus a higher average summary number of children (p<0.001), although the pathophysiology supporting the impact of labour or the number of gestations on the prevention of UFs is not fully understood, it is hypothesized that it may be because of the uterus's susceptibility to ischemia during labour [9, 11]. Pregnancy can have a significant impact on fibroid growth because of the abrupt increases and decreases in estrogen and progesterone levels that occur during the very early stages of pregnancy and the postpartum phase. A 3- to 6-month postpartum ultrasonography scan fails to detect almost 36% of fibroids that were present during the first trimester of pregnancy; those that did show up had a median diameter reduction of 0.5 cm [24].
It was also noticed that a higher percentage of women who used intrauterine devices (IUDs) as a method of contraception (p=0.012), whereas most studies conducted on samples of women with uterine fibroids used the IUDs for therapeutic purposes in the treatment of menorrhagia rather than for contraception [25].
Furthermore, there has been an increase in the percentage of women suffering from hypertension (p<0.001), this is consistent with the results of a study conducted on Saudi women with UFs had a significantly higher prevalence of obesity and hypertension [16]. Moreover diabetes (p<0.001), based on the results of a study conducted by Muawad R. et al., diabetes was associated with an 11% lower risk of developing UFs[16]. In some studies, diabetes was inversely associated with the risk of developing UFs, and this association contradicts previous studies [8]. The molecular explanation for this inverse association, according to some study, may be the high levels of insulin-like growth factor-1 (IGF-1) in the blood, which raise SHBG and lower levels of circulating estradiol [26, 27]. In contrast, women without diabetes typically have low levels of IGF-1, a crucial growth factor for UF cells. Diabetes medications may also help reduce the impact of IGF-1 on the UFs growth by reducing the proliferative effects of UF cells relative to normal cells [16].
Also, EH (p=0.009), in line with a study by Ponomarenko M.S. et al., the incidence of atypical EH was almost four times higher in obese women with a BMI≥30 kg/m2 than in non-obese women [20]. The conversion of androgens by the ovaries and adrenal glands into estrogens in the adipose tissue explains this link. The development of insulin resistance and decreased production of globulin, which binds sex hormones, are both facilitated by excess fat. Because of this, there are more free circulating estrogens in obese women, which may encourage the development of UF and EH [20, 28]. Additionally, one of the primary components of metabolic syndrome, hyperinsulinemia, is linked to elevated serum levels of insulin-like growth factor-1 and epidermal growth factor [3], which in turn cause the ovaries to secrete estrogen or encourage the growth of cells in the endometrium and myometrium [16, 29].
In addition to a higher percentage of women who underwent myomectomy (p<0.001) and hysterectomy (p<0.001). Some studies found more clinical usage of less invasive approaches such as laparoscopic myomectomy which can be performed safely for the obese patients [12]. As for a study by Pavone D. et al., African-American women have a 6.8-fold higher risk of having a uterine-sparing myomectomy and a 2.4-fold higher risk of having a hysterectomy [24].
As for the size (p<0.001) and the location of the fibroid nodes (p=0.010), in women with BMI 25-29.99 kg/m2, fibromatous nodes in most UF patients were located intramurally and had the largest size. Whereas in women with BMI<25 and BMI≥30 kg/m2, subserosal nodes were the most common and the size of the nodes was significantly smaller than in UF patients with BMI 25–29.99 kg/m2. Similarly, in women with BMI<25 kg/m2, were found, with a fairly high frequency, pedunculated nodes, and a combination of subserosal and intramural nodes. At the same time, submucosal nodes were more than 4 times more common in UF patients with BMI≥30 kg/m2 compared with other studied groups.
In contrast to our findings, Harmon Q.E. et al. study revealed that obese women had bigger uterine fibroids [30], while another study found no discernible difference in leiomyoma size between obese and non-obese women [12]. The majority of patients had solitary intramural (or submucosal) fibroids, indicating that the myometrium is the primary source of UFs, according to research by Sharami S.H. et al. [9].
Considering the results of a study conducted on women undergoing hysterectomies that observed postmenopausal women had smaller and fewer fibroids compared to premenopausal women [31], it is possible that the results of our study are consistent with the fact that the largest percentage of women were >50 years old. Furthermore, a research by Bray M.J. et al. found no correlation between BMI and fibroid size or number [31]. However, rising BMI was linked to fibroid risk but not to the biggest fibroid dimension in prior research of women who underwent a hysterectomy. This lack of correlation between BMI and the size or number of fibroids may indicate that BMI affects fibroid risk rather than progression. This might imply that larger or more numerous fibroids are not caused by the increased estrogen exposure brought on by rising obesity [32].
Conclusion
This study showed that Syrian women with different body mass indexes have distinct clinical manifestations of uterine fibroids. That will provide further insight into how they are affected by variations in BMI, and consequently, how these variations influence the risk and prevalence of UFs, which is helpful in their diagnosis, prevention, and symptom relief.
References
- Алали О.М., Чурносов М.И. Полногеномные исследования миомы матки. Акушерство и гинекология. 2023; 7: 28-38. [Alali O.M., Churnosov M.I. Genome-wide studies of uterine leiomyomas. Obstetrics and Gynecology. 2023; (7): 28-38 (in Russian)]. https://dx.doi.org/10.18565/aig.2023.156
- Ponomarenko I., Reshetnikov E., Polonikov A., Verzilina I., Sorokina I., Yermachenko A. et al. Candidate genes for age at menarche are associated with uterine leiomyoma. Front. Genet. 2021; 11: 512940. https://dx.doi.org/10.3389/fgene.2020.512940
- Алали О.М., Хаддам В.М., Чурносов М.И. Клинические характеристики сирийских женщин с лейомиомой матки. Акушерство и гинекология. 2025; 7: 76-83. [Alali O.M., Khaddam W.M., Churnosov M.I. Сlinical characteristics of Syrian women with uterine leiomyoma. Obstetrics and Gynecology. 2025; (7): 76-83 (in Russian)]. https://dx.doi.org/10.18565/aig.2025.59
- Пономаренко И.В., Полоников А.В., Чурносов М.И. Полиморфные локусы гена LHCGR, ассоциированные с развитием миомы матки. Акушерство и гинекология. 2018; 10: 86-91. [Ponomarenko I.V., Polonikov A.V., Churnosov M.I. Polymorphic LHCGR gene loci associated with the development of uterine fibroids. Obstetrics and Gynecology. 2018; (10): 86-91 (in Russian)]. https://dx.doi.org/10.18565/aig.2018.10.86-91
- Qin H., Lin Z., Vásquez E., Luan X., Guo F., Xu L. Association between obesity and the risk of uterine fibroids: a systematic review and meta-analysis. J. Epidemiol. Community Health. 2021; 75: 197-204. https://doi.org/10.1136/jech-2019-213364
- Maghraby N., El Noweihi A.M., El-Melegy N.T., Mostafa N.A., Abbas A.M., El-Deek H.E. et al. Increased expression of fibroblast activation protein is associated with autophagy dysregulation and oxidative stress in obese women with uterine fibroids. Reprod. Sci. 2021; 29(2): 1-2. https://dx.doi.org/10.1007/s43032-021-00810-0
- Alali O.M., Churnosov M.I. The etiopathogenesis of uterine leiomyomas: a review. Gynecology. 2023; 25(1): 22-30. https://dx.doi.org/10.26442/20795696.2023.1.201827
- Пономаренко М.С., Решетников Е.А., Пономаренко И.В., Чурносов М.И. Факторы риска развития миомы матки. Акушерство и гинекология. 2024; 3: 20-7. [Ponomarenko M.S., Reshetnikov E.A., Ponomarenko I.V., Churnosov M.I. Risk factors for the development of uterine fibroids. Obstetrics and Gynecology. 2024; (3): 20-7 (in Russian)]. https://dx.doi.org/10.18565/aig.2023.275
- Sharami S.H., Fallah Arzpeyma S., Shakiba M., Montazeri S., Milani F., Kazemi S. et al. Relationship of uterine fibroids with lipid profile, anthropometric characteristics, subcutaneous and preperitoneal fat thickness. Arch. Iran. Med. 2019; 22(12): 716-21.
- Pan H., Qin F., Deng F. Clinical value of body mass index and waist-hip ratio in clinicopathological characteristics and prognosis of uterine leiomyomata. Evid. Based Complement. Alternat. Med. 2021; 2021: 8156288. https://dx.doi.org/10.1155/2021/8156288
- Пономаренко М.С., Решетников Е.А., Пономаренко И.В., Чурносов М.И. Этиопатогенетические механизмы развития миомы матки. Акушерство и гинекология. 2024; 1: 34-41. [Ponomarenko M.S., Reshetnikov E.A., Ponomarenko I.V., Churnosov M.I. Etiopathogenetic mechanisms of uterine fibroids development. Obstetrics and Gynecology. 2024; (1): 34-41 (in Russian)]. https://dx.doi.org/10.18565/aig.2023.241
- Gürbüz T., Yardımcı O., Udum S., Günay T. The relationship between body mass index and clinical complications among patients undergoing myomectomy. J. Surg. Med. 2020; 4(11): 1027-30. https://dx.doi.org/10.28982/josam.805122
- Lee J.E., Song S., Cho E., Jang H.J., Jung H., Lee H.Y. et al. Weight change and risk of uterine leiomyomas: Korea Nurses’ Health Study. Cur. Med. Res. Opin. 2018; 34(11): 1913-9. https://dx.doi.org/10.1080/03007995.2018.1462783
- Haan Y.C., Diemer F.S., Van der Woude L., Van Montfrans G.A., Oehlers G.P., Brewster L.M. The risk of hypertension and cardiovascular disease in women with uterine fibroids. J Clin Hypertens (Greenwich). 2018; 20(4): 718-26. https://dx.doi.org/10.1111/jch.13253
- Пономаренко И.В., Чурносов М.И. Современные представления об этиопатогенезе и факторах риска лейомиомы матки. Акушерство и гинекология. 2018; 8: 27-32. [Ponomarenko I.V., Churnosov M.I. Current views on the etiopathogenesis and risk factors of uterine leiomyoma. Obstetrics and Gynecology. 2018; (8): 27-32 (in Russian)]. https://dx.doi.org/10.18565/aig.2018.8.27-32
- Muawad R., Dabbagh R., Sabr Y. Association of health and lifestyle factors with uterine fibroids among Saudi women: a case–control study. J. Taibah Univ. Med. Sci. 2022; 17(6): 1039-46. https://dx.doi.org/10.1016/j.jtumed.2022.06.005
- Keizer A.L., Semmler A., Kok H.S., van Kesteren P.J., Huirne J.A., Hehenkamp W.J. Modifiable prognostic factors in uterine fibroid development: a systematic review of literature. J. Obstet. Gynaecol. 2024; 44(1): 2288225. https://dx.doi.org/10.1080/01443615.2023.2288225
- Donnez J., Dolmans M.M. Uterine fibroid management: from the present to the future. Hum. Reprod. Update. 2016; 22(6): 665-86. https://dx.doi.org/10.1093/humupd/dmw023
- Wise L.A., Laughlin-Tommaso S.K. Epidemiology of uterine fibroids – from menarche to menopause. Clin. Obstet. Gynecol. 2016; 59(1): 2-24. https://dx.doi.org/10.1097/GRF.0000000000000164
- Ponomarenko M.S., Reshetnikov E.A., Churnosova M.M., Reshetnikova Y.N., Churnosov V.I., Ponomarenko I.V. Comorbidity and syntropy of benign proliferative diseases of the female reproductive system: non-genetic, genetic, and epigenetic factors (review). Research Results in Biomedicine. 2023; 9(4): 544-56. https://dx.doi.org/10.18413/2658- 6533-2023-9-4-0-9
- Stewart E.A., Cookson C.L., Gandolfo R.A., Schulze‐Rath R. Epidemiology of uterine fibroids: a systematic review. BJOG. 2017; 124(10): 1501-12. https://dx.doi.org/10.1111/1471-0528.14640
- Nwonuma C., Irokanulo E., Bamgboye F., Akinduko A., Okeniyi F., Eigbe C. Uterine fibroid: risk factors and therapeutic interventions. In: International conference on science, engineering and business for driving sustainable development goals (SEB4SDG), 2024 Apr. 2-4. Omu-aran;2024: 1-10.
- Shabahat Ahmed A., Kiran Sharif M.A. Prevalence and clinical characteristics of uterine fibroids in women of reproductive age in district hyderabad. The Research of Medical Science Review. 2025; 3(1): 635-47.
- Pavone D., Clemenza S., Sorbi F., Fambrini M., Petraglia F. Epidemiology and risk factors of uterine fibroids. Best Pract. Res. Clin. Obstet. Gynaecol. 2018; 46: 3-11. https://dx.doi.org/10.1016/J.BPOBGYN.2017.09.004
- Zapata L.B., Whiteman M.K., Tepper N.K., Jamieson D.J., Marchbanks P.A., Curtis K.M. Intrauterine device use among women with uterine fibroids: a systematic review. Contraception. 2010; 82(1): 41-55. https://dx.doi.org/10.1016/j.contraception.2010.02.011
- Пономарева Т.А. Генетические варианты глобулина, связывающего половые гормоны, и гормональный профиль больных генитальным эндометриозом. Научные результаты биомедицинских исследований. 2025; 11(1): 75-90. [Ponomareva T.A. Genetic variants of sex hormone-binding globulin and hormonal profile in patients with genital endometriosis. Research Results in Biomedicine. 2025; 11(1): 75-90 (in Russian)]. https://dx.doi.org/10.18413/2658-6533-2025-11-1-0-4
- Ponomarenko M.S. The relationship between the genetic determinants of SHBG and the hormonal profile of patients with uterine fibroids. Research Results in Biomedicine. 2025; 11(4): 628-42. https://dx.doi.org/10.18413/2658-6533-2025-11-4-0-3
- Alsudairi H.N., Alrasheed A.T., Dvornyk V. Estrogens and uterine fibroids: an integrated view. Research Results in Biomedicine. 2021; 7(2): 156-63. https://dx.doi.org/10.18413/2658-6533-2021-7-2-0-6
- Чурносов В.И. Ассоциации полиморфных локусов генов-кандидатов с уровнем половых гормонов у больных гиперплазией эндометрия. Научные результаты биомедицинских исследований. 2025;11(2):243-262. [Churnosov V.I. Associations of polymorphic loci of candidate genes with the level of sex hormones in patients with endometrial hyperplasia. Research Results in Biomedicine. 2025; 11(2): 243-62 (in Russian)]. https://dx.doi.org/10.18413/2658-6533-2025-11-2-0-3
- Harmon Q.E., Patchel S., Denslow S., Wegienka G., Baird D.D. Body mass index and uterine fibroid development: a prospective study. The Journal of Clinical Endocrinology & Metabolism. 2024; 109(11): e2016-23. https://dx.doi.org/10.1210/clinem/dgae036
- Bray M.J., Torstenson E.S., Jones S.H., Edwards T.L., Edwards D.R. Evaluating risk factors for differences in fibroid size and number using a large electronic health record population. Maturitas. 2018; 114: 9-13. https://dx.doi.org/10.1016/j.maturitas.2018.05.003
- Ponomarenko M., Reshetnikov E., Churnosova M., Aristova I., Abramova M., Novakov V. et al. Genetic variants linked with the concentration of sex hormone-binding globulin correlate with uterine fibroid risk. Life (Basel). 2025; 15(7): 1150. https://dx.doi.org/10.3390/life15071150
Received 18.11.2025
Accepted 28.04.2026
About the Authors
Ola Mohamad Alali, PhD student, Belgorod State National Research University, 85 Pobedy str., 308015, Belgorod, Russia, alali@bsuedu.ru,https://orcid.org/0000-0003-4370-6719
Walid Khaddam, Doctor of Microbiology, Homs University, Homs, Syria, wkhaddam@homs-univ.edu.sy, https://orcid.org./0000-0001-6771-2211
Mikhail I. Churnosov, Dr. Med. Sci., Professor, Head of the Department of Medical and Biological Disciplines, Belgorod National Research University, 85 Pobedy str.,
308015, Belgorod, Russia, churnosov@bsuedu.ru, https://orcid.org/ 0000-0003-1254-6134
Similar Articles

