
Latent and overt maternal risks and outcomes of insufficient fetal growth
Ziyadinov A.A., Novikova V.A., Radzinsky V.E.
Objective. To investigate the associations between latent and overt maternal risk factors, timing of delivery, and the need for neonatal intensive care in pregnancies complicated by fetal growth restriction (FGR) or small-for-gestational-age (SGA) fetuses.
Materials and methods. A prospective cohort study was conducted at N.A. Semashko Republican Clinical Hospital Perinatal Center from 2018 to 2023. The study included 611 women with insufficient fetal growth (IFG): 435 with FGR and 176 with SGA.
Results. Maternal comorbidity associated with IFG was predominantly cardiometabolic in nature. However, in 45.5% of patients, the cause remained unclear (idiopathic), and occurred more frequently in FGR. Preeclampsia (PE) and type 1 diabetes mellitus (type 1 DM) were exclusive markers of FGR, whereas gestational and chronic arterial hypertension (GAH and CAH) and gestational diabetes mellitus (GDM) were more characteristic of SGA. FGR was exclusively associated with emergency delivery for fetal indications in cases of severe PE, unknown causes of IFG, and GAH. Precipitous labor was an absolute marker of FGR, whereas dysfunctional labor was a characteristic of SGA. Delivery within the recommended optimal gestational interval was achieved in only 37.64% of patients with IFG, more frequently in SGA cases, and may have occurred before the third ultrasound screening. Prematurity was exclusive to the FGR group. Iatrogenic prematurity accounted for 86.49% of all preterm births and was primarily associated with PE and CAH. An unknown cause of IFG was associated with delivery outside the optimal gestational interval in 46.76% of patients with FGR; in 9.9% of these cases, delivery occurred before the recommended interval. Neonatal intensive care (IC) was required in 73.16% of newborns, and 20.95% of these infants required respiratory support (RS). The need for IC combined with RS was observed exclusively in the FGR group. SGA, as a constitutional fetal characteristic, did not preclude the need for IC in the absence of a RS. Delivery before 39 weeks in SGA was predictive of neonatal IC requirements, whereas delivery before 35 weeks in FGR predicted the need for IC combined with RS.
Conclusion. In addition to maternal cardiometabolic disorders, latent IFG-related risks may emerge in 45.5% of patients either before the third ultrasound screening or at term. This contributes to missed opportunities for delivery within the optimal gestational window, particularly in the case of FGR. Patients with IFG are at an increased risk of emergency delivery and prematurity (34.02%, including extreme prematurity), of which 86.49% is iatrogenic. SGA, often regarded as a constitutional fetal characteristic, may be associated with GAH, CAH, and GDM. Neonatal IC was required in 73.16% of cases, with 20.95% additionally requiring RS, exclusively among infants with FGR. Prematurity is unequivocally associated with the need for IC. Timely identification of chronic and gestational maternal cardiometabolic disorders may facilitate the early detection of FGR and SGA and help determine the optimal timing and location of delivery, thereby minimizing neonatal risks.
Authors' contributions. Ziyadinov A.A. – conception and design of the study, data analysis, drafting and editing of the manuscript, interpretation of results, approval of the manuscript for submission; Novikova V.A. – conception and design of the study, statistical analysis and interpretation of results; Radzinsky V.E. – conception and design of the study, editing of the manuscript, approval of the manuscript for submission.
Conflicts of interest. The authors have no conflicts of interest to declare.
Funding. There was no funding for this study.
Ethical Approval. The study was reviewed and approved by the Research Ethics Committee of the Peoples' Friendship University of Russia named after Patrice Lumumba.
Generative Artificial Intelligence. No artificial intelligence tools were used in the preparation of this manuscript.
Patient Consent for Publication. All patients provided informed consent for the publication of their data.
Authors' Data Sharing Statement. The data supporting the findings of this study are available upon request from the corresponding author after approval from the principal investigator.
For citation: Ziyadinov A.A., Novikova V.A., Radzinsky V.E. Latent and
overt maternal risks and outcomes of insufficient fetal growth.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (6): 68-81 (in Russian)
https://dx.doi.org/10.18565/aig.2026.62
Keywords
pregnancy
fetal growth restriction
small-for-gestational-age fetus
gestational age at delivery
latent risks of insufficient fetal growth
idiopathic cause of insufficient fetal growth
classification trees
Insufficient fetal growth (IFG), whether manifested as a small-for-gestational-age fetus (SGA) or fetal growth restriction (FGR), necessitates timely medical care for the mother [1], although such care is not always feasible. According to published data, the prevalence of SGA ranges from 10 to 27%, while FGR affects 3–9% of pregnancies in high-income countries and up to 25% in low- and middle-income countries [2]. Estimating the prevalence of FGR and SGA in Russia remains challenging because of limited national data, which are primarily restricted to regional studies.
Fetal prognosis is largely determined by the FGR phenotype: late-onset FGR, diagnosed after 32 weeks of gestation, or early onset FGR, diagnosed before 32 weeks of gestation, and associated with a less favorable prognosis. Early onset FGR is less prevalent than late-onset disease (1% versus 5–10%), and the recurrence of FGR or SGA occurs in approximately 20% of subsequent pregnancies [2]. Some investigators have proposed the concept of early onset SGA (eoSGA) in non-anomalous fetuses, defined as an estimated fetal weight and/or abdominal circumference below the 10th percentile between 16+0 and 31+6 weeks’ gestation [3].
A major challenge in diagnosing IFG is that the underlying causes of FGR are not always apparent, and approximately 40% of SGA fetuses have no associated maternal disease or gestational complications. Although etiological factors are conventionally categorized as fetal, placental, or maternal, their pathophysiological pathways frequently overlap [4]. The specific IFG phenotype (FGR or SGA) determines the timing of delivery and influences the subsequent risk of either iatrogenic prematurity or delayed delivery, which can result in progressive fetal compromise that may reach critical severity [5]. Timely identification of growth-restricted fetuses, the anticipated need for early delivery, and the risk of adverse perinatal outcomes necessitate referral of the mother to a healthcare facility with appropriate neonatal expertise, adequate resources, and access to qualified neonatal intensive-care specialists. Persistent failures in antenatal IFG diagnosis and challenges in determining the optimal timing of delivery continue to jeopardize neonatal outcomes.
This study aimed to evaluate the association between latent risks and maternal comorbidity with the timing of delivery and the need for neonatal intensive care (IC) among infants with FGR or SGA.
Materials and methods
A prospective cohort study was conducted at the N.A. Semashko Republican Clinical Hospital Perinatal Center between 2018 and 2023. The study cohort was assembled using a consecutive sampling approach that involved a retrospective review of all deliveries at the perinatal center during 2018–2023 (n=24,282), followed by the prospective enrollment of eligible patients. A total of 611 women were selected and stratified according to the type of IFG – FGR or SGA – including 435 women with FGR and 176 with SGA.
The inclusion criteria were: singleton pregnancy; IFG (FGR or SGA) with subsequent postnatal confirmation after delivery; a single predominant cause of IFG, namely preeclampsia (PE) (severe or moderate), diabetes mellitus (DM) (gestational diabetes mellitus [GDM] or type 1 diabetes mellitus), chronic arterial hypertension (CAH), gestational arterial hypertension (GAH), or an unknown cause; and live birth. Patients with multiple pregnancies, discordance between antenatal and postnatal IFG diagnoses, or two or more competing causes of IFG of comparable significance were excluded. An unspecified cause of IFG was defined as idiopathic etiology characterized by the absence of verified maternal, fetal, and overt placental risk factors, including severe maternal extragenital comorbidity, PE, fetal chromosomal abnormalities and congenital malformations, and intrauterine infections.
The clinical outcomes (endpoints) assessed were the type of fetal growth impairment, its underlying cause, and the need for neonatal intensive care (IC), either with or without respiratory support (RS). The diagnostic criteria for FGR and SGA were consistent with national clinical guidelines, and the diagnosis of fetal smallness was based on the INTERGROWTH-21st standards [1].
The study was limited by its observational prospective design, the potential influence of latent confounding factors when identifying the predominant cause of IFG, and its conduct at a single tertiary-level perinatal center, which may have introduced selection bias toward more severe clinical cases.
Statistical analysis
Mathematical and statistical analyses were performed using Statistica 12.0 and Microsoft Excel 2016. Sample size (n), median (Me), and lower and upper quartiles (Q1, Q3) were calculated. Comparisons between two independent groups for continuous variables were conducted using the Mann–Whitney U test. The significance of differences in outcomes associated with the factor under investigation was assessed using the chi-square (χ²) test; when n<10, the Yates-corrected chi-square was applied. Associations between risk factors and categorical variables were evaluated using odds ratio (OR) with 95% confidence interval (CI), the standard measure for case–control studies.
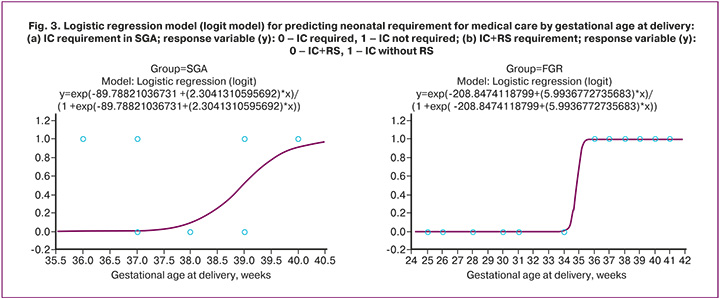
Binary logistic regression (logit model) was used to assess the prognostic significance of gestational age at delivery for neonatal complications, specifically the need for IC and RS. Categorical neonatal outcomes served as dependent variables, whereas gestational age in weeks was included as the independent predictor variable. Model adequacy was evaluated using the goodness-of-fit chi-square criterion and OR estimates. The results were presented as logit curves illustrating changes in the probability of a categorical outcome across values of the continuous predictor.
The Feature Selection module was used to identify highly informative risk factors (p<0.05) associated with FGR or SGA. Prediction of class membership for the categorical dependent variable was based on decision tree construction (classification and regression trees). Exhaustive CHAID (Exhaustive Chi-Squared Automatic Interaction Detection) analysis was performed using the Classification Trees module. Regression tree analysis was applied to model continuous predictors (e.g., gestational age at delivery) and to identify the hierarchy of influencing factors. Node splitting was based on the F statistic. The mathematical output for each node was expressed as the arithmetic mean (Mu) and variance (Var), reflecting the degree of homogeneity within the resulting subgroups. Predictors of the study outcome (categorical response variable) were also identified within the dataset.
Only valid models meeting the following predefined statistical reliability criteria were included: a risk estimate for the training sample not exceeding 0.11 (corresponding to an overall classification accuracy of 89% and minimization of classification error), and a difference between risk estimates for the training and cross-validation samples (V-fold) of no more than 0.005 during V-fold cross-validation, thereby excluding model overfitting.
Results
In the study cohort, the majority of etiological contributors to insufficient fetal growth (IFG) — six out of five identified categories – were cardiometabolic obstetric complications, encompassing hypertensive disorders (chronic arterial hypertension [CAH], gestational arterial hypertension [GAH], and preeclampsia [PE], both moderate and severe) and diabetes mellitus (DM) (Fig. 1a).
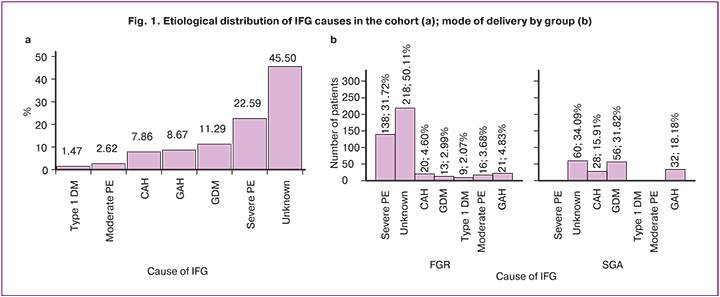
In 45.5% of patients, the underlying cause of IFG could not be identified and was classified as "unknown"; this category was more frequently associated with fetal growth restriction (FGR) than with small-for-gestational-age (SGA) (OR=1.94, 95% CI 1.35–2.80). Severe and moderate PE were exclusive markers of FGR (χ²=70.32, p<0.001 and χ²=5.28, p=0.02, respectively), whereas GAH (OR=4.38, 95% CI 2.45–7.84), CAH (OR=3.93, 95% CI 2.15–7.18), and gestational diabetes mellitus (GDM) (OR=15.15, 95% CI 8.02–28.63) were more strongly associated with SGA. Type 1 DM, despite its low prevalence (2.07%), was an exclusive marker of FGR (p=0.006) (Fig. 1b).
Just over half of all patients in the cohort were delivered by cesarean section (CS) (55.16%; 337/611), with CS occurring significantly more frequently in the FGR group than in the SGA group (273/435 vs. 64/176; χ²=35.03, p<0.001; OR=2.95, 95% CI 2.05–4.24). Certain etiological factors were found to influence the mode of delivery. Among patients with FGR, CS was exclusively associated with severe PE (138/435 vs. 0/176; χ²=7.32, p<0.001), CAH (20/435 vs. 0/176; χ²=6.98, p=0.009), and moderate PE (16/435 vs. 0/176; χ²=5.28, p=0.02). Among patients with SGA, CS was associated with GAH (32/176 vs. 21/435; OR=4.38, 95% CI 2.45–7.84), while an unknown etiology showed only a trend toward association (32/176 vs. 78/435; OR=1.02, 95% CI 0.65–1.60). Vaginal delivery in FGR, compared with SGA, was more commonly associated with an unknown IFG cause (140/435 vs. 28/176; OR=2.51, 95% CI 1.60–3.94); in SGA, it was associated with GDM (56/176 vs. 13/435; OR=15.15, 95% CI 8.02–28.63) and exclusively with CAH (28/176 vs. 0/435; χ²=68.94, p<0.001). In all cases of DM – including type 1 DM (n=9; χ²=2.41, p=0.12) – delivery was completed vaginally.
It is noteworthy that emergency CS was more than twice as common as elective CS (69.14% [233/273] vs. 30.86% [104/273]), and maternal indications predominated over fetal indications (51.78% [175/273] vs. 48.22% [163/273]). FGR was distinguished from SGA by an exclusive and predominant association with emergency CS (233/273 vs. 0/64; χ²=173.02, p<0.001), driven by fetal indications (163/273 vs. 0/64; χ²=71.64, p<0.001), in the context of severe PE (68/273 vs. 0/64; χ²=18.46, p<0.001), unknown etiology (38/273 vs. 0/64; χ²=8.7, p=0.004), and GAH (21/273 vs. 0/64; χ²=4.02, p=0.046), but not CAH (20/273 vs. 0/64; χ²=3.76, p=0.053) or moderate PE (16/273 vs. 0/64; χ²=2.75, p=0.10). SGA was exclusively associated with elective CS for maternal indications (64/64 vs. 110/273), with two etiological contributors: unknown cause (32/64 vs. 40/273; OR=5.83, 95% CI 3.22–10.55) and GAH (32/64 vs. 0/273; χ²=145.06, p<0.001).
The indications for CS differed fundamentally between the two IFG phenotypes. Exclusive FGR-associated indications included: severe PE (70/273 vs. 0/64; χ²=19.18, p<0.001), PE with critical fetal compromise (68/273 vs. 0/64; χ²=18.46, p<0.001), progressive chronic placental insufficiency (95/273 vs. 0/64; χ²=29.32, p<0.001), and an unripe cervix at gestational age >40+6 weeks (20/273 vs. 0/64; χ²=3.76, p=0.053). Exclusive SGA-associated indications included: uterine scar after prior CS with an unripe cervix at term (32/64 vs. 0/273; χ²=145.06, p<0.001) and two or more uterine scars after prior CS (32/64 vs. 20/273; χ²=69.12, p<0.001).
Complications of vaginal delivery also differed between the IFG phenotypes. Precipitate labor was an absolute marker of FGR (16/162 vs. 0/112; χ²=10.02, p=0.002), whereas incoordinate uterine activity was exclusive to SGA (28/112 vs. 0/162; χ²=42.43, p<0.001). Rapid labor occurred at comparable rates in both groups (40/162 vs. 28/112; χ²=0.007, p=0.93). Notably, precipitate labor occurred exclusively in cases of unknown etiology with FGR (n=16); incoordinate uterine activity was confined to GDM with SGA (n=28); and rapid labor occurred in cases of unknown etiology with FGR (n=40) and CAH with SGA (n=28). Labor induction (amniotomy) was required in 5.06% (22/435) of patients with FGR and exclusively at term.
Gestational age at delivery ranged from 25 to 41 weeks across the cohort (Fig. 2), with a median at term (median = 39 weeks; IQR 37–39 weeks). Although the median was equal between groups, delivery occurred earlier in FGR than in SGA, with the first quartile at 34 weeks (median = 39 weeks; IQR 34–39 vs. 39–39 weeks; p<0.001). Gestational age at delivery of ≤37.5 weeks was exclusive to FGR (44.6%; 194/435).
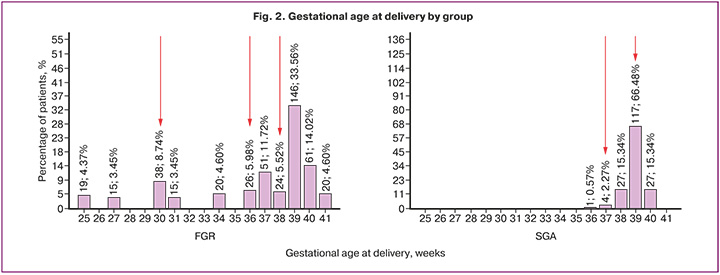
Delivery within the recommended optimal gestational window (37–39 weeks for SGA and 36–38 weeks for FGR) occurred in only 37.64% (230/611) of patients and was far more common in the SGA group (148/176 vs. 82/435; OR=22.75, 95% CI 14.22–36.41).
Delivery beyond the recommended optimal window occurred in 41.41% (253/611) of patients and was more frequent in the FGR group (51.72%; 225/435 [where 225=120+13+9+21+42+20]) than in the SGA group (15.91%; 28/176) (OR=5.66, 95% CI 3.63–8.84) (Fig. 2b).
Delivery prior to the optimal gestational window occurred in 20.95% (128/611) of patients and was exclusive to the FGR group (29.43%; 128/435 vs. 0/176; χ²=63.75, p<0.001).
Preterm birth was observed in 24.22% (148/611) of patients – including very preterm and extremely preterm births – exclusively in the FGR group (34.02%; 148/435 vs. 0/176; χ²=79.02, p<0.001). The early-onset phenotype corresponded to 24.83% of FGR cases (108/435). Particularly notable is that delivery in 5.89% of cohort patients (1+19+16=36/611) occurred even before the minimum gestational threshold (Fig. 2a) – a threshold defined in clinical guidelines as the earliest recommended gestational age for "elective referral of a high-risk patient for FGR surveillance ultrasound" (before 30–34 weeks of gestation) [1].
Analysis of gestational age at delivery revealed fundamental differences in the clinical course and etiological composition of the two IFG phenotypes (Table 1).
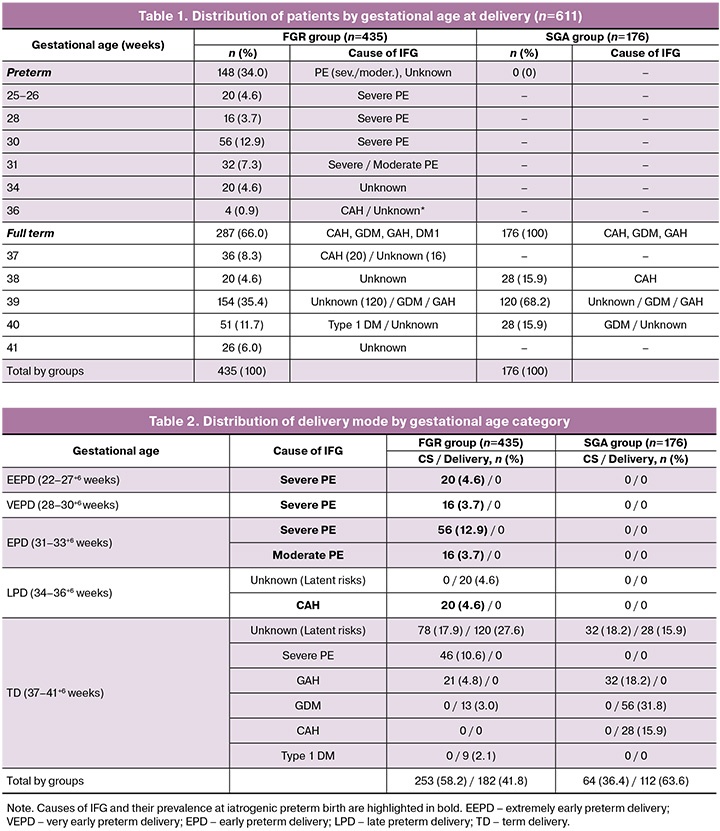
The distribution of patients by gestational age at delivery and etiological factor revealed substantial heterogeneity between the groups. In the FGR group, severe PE dominated deliveries between 25 and 34 weeks, while no early deliveries occurred in the SGA group. Between 37 and 41 weeks, maternal cardiometabolic comorbidity (CAH, GDM, GAH) and unknown etiology predominated in both groups. Of particular note is 39 weeks, which represented the peak of delivery in both groups and at which the etiological profile became identical between phenotypes, being composed predominantly of GDM, GAH, and – in the majority of cases – unknown etiology (latent risk factors). The predominance at 39 weeks of etiological factors unrelated to classical placental insufficiency confirms that, for these IFG phenotypes, maternal comorbidity and occult metabolic disturbances are the primary determinants of the decision to deliver at near-physiological gestational ages.
Preterm birth was associated in a specific manner with maternal comorbidity. Among cohort patients (n=611), severe PE showed the strongest association with preterm birth (92/148 vs. 46/463; OR = 14.89, 95% CI 9.49–23.37), followed – at a considerable distance – by CAH (20/148 vs. 28/463; OR=2.43, 95% CI 1.32–4.45), while moderate PE was not diagnosed at term in any case (χ²=47.25, p<0.001). FGR in the context of severe PE was diagnosed exclusively at 25 and 26 weeks (Fig. 2b).
Term delivery in the cohort was most strongly associated with unknown etiology (258/463 vs. 20/148; OR=8.06, 95% CI 4.86–13.36), while GDM (χ²= 3.40, p<0.001), type 1 DM (χ²=1.73, p=0.19), and GAH (χ²=18.55, p<0.001) were identified as its unique markers.
Preterm birth was iatrogenic in 86.49% (128/148) of patients who were delivered by CS, and spontaneous in only 13.51% (20/148) (Table 2). Iatrogenic prematurity was attributable to PE (both severe and moderate) and CAH.
In accordance with current clinical guidelines [1], delivery within the recommended optimal gestational window (37–39 weeks for SGA and 36–38 weeks for FGR) occurred in only 37.64% (230/611) of cohort patients, with far greater adherence in the SGA group (148/176 vs. 82/435; OR=22.75, 95% CI 14.22–36.41) (Table 3).
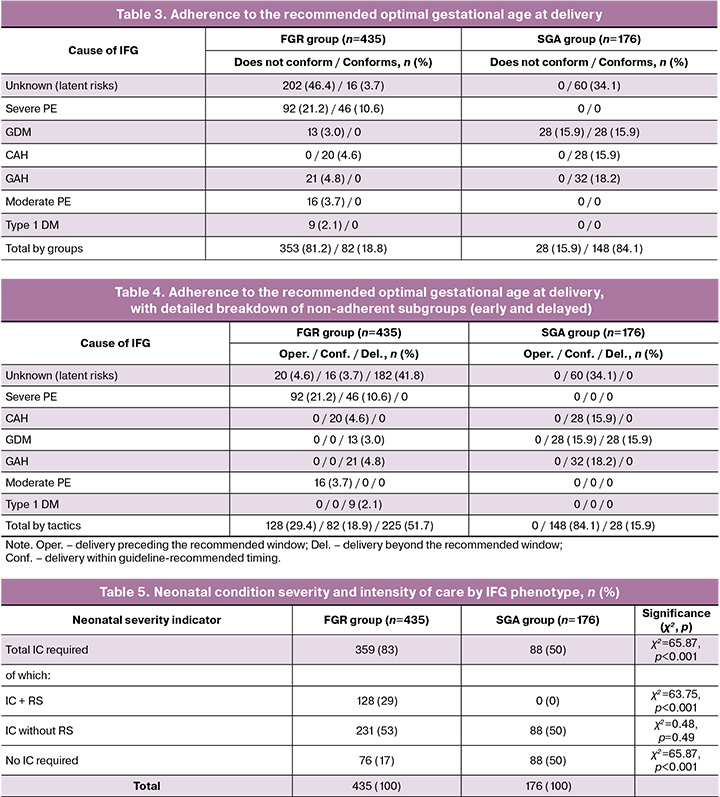
Delivery beyond the optimal window occurred in 41.41% (253/611) of patients, more commonly in the FGR group (51.72%; 225/435 [225=120+13+9+21+42+20]) than in the SGA group (15.91%; 28/176) (OR=5.66, 95% CI 3.63–8.84) (Table 4).
Delivery preceding the optimal gestational window occurred in 20.95% (128/611) of cohort patients and was exclusive to the FGR group (29.43%; 128/435 vs. 0/176; χ²=63.75, p<0.001).
Importantly, among patients with FGR delivered outside the optimal window (46.76%; 202/435), the IFG cause was unknown in the largest subgroup; in 9.9% of these patients (20/202), or 4.6% of all FGR patients (20/435), delivery occurred before the recommended window (Table 4). Among SGA patients, delivery outside the recommended window (delayed) occurred exclusively in the GDM subgroup (15.34%; 27/176).
Ultimately, neonatal intensive care (IC) was required by almost three-quarters (73.16%; 447/611) of neonates in the cohort; 20.95% (n = 128) required IC with respiratory support (RS) (IC+RS). The need for neonatal IC was significantly more common in FGR than in SGA (359/435 vs. 88/176; χ²=65.87, p<0.001; OR=4.72, 95% CI 3.21–6.95), and the requirement for RS was an exclusive marker of FGR (128/435 vs. 0/176; χ²=63.75, p<0.001) (Table 5).
IC without RS was required at comparable rates in FGR and SGA (53.10% [231/435] vs. 50.00% [88/176]; χ²=0.48, p=0.49). The need for neonatal IC was associated with IFG phenotype and its etiology (Table 6).
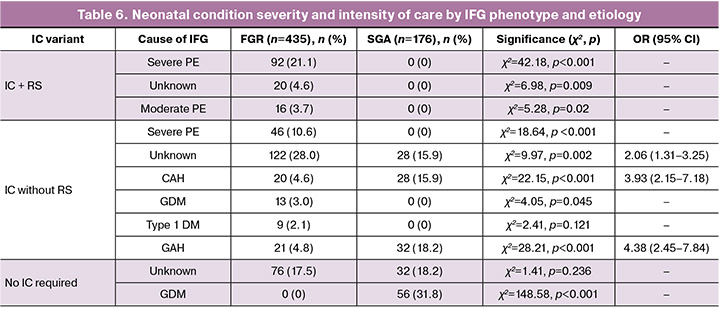
IC+RS was exclusive to FGR and was associated with severe PE (χ²=42.18, p<0.001), unknown etiology (χ²=6.98, p=0.009), and moderate PE (χ²=5.28, p=0.02). IC without RS was exclusive to FGR in the context of severe PE (χ²=18.64, p<0.001) and GDM (χ²=4.05, p=0.045), and more frequent with unknown etiology (OR=2.06, 95% CI 1.31–3.25). In the SGA group, IC without RS was more frequently associated with CAH (OR=3.93, 95% CI 2.15–7.18) and GAH (OR=4.38, 95% CI 2.45–7.84). The absence of IC requirement was exclusive to SGA with GDM (χ²=148.58, p<0.001), while with unknown etiology, IC was required at comparable rates in FGR and SGA patients (χ²=1.41, p=0.24).
Preterm birth was unconditionally associated with IC (148/148; 100%): in 86.49% of preterm neonates (128/148) as IC+RS – including 92/128 in the context of severe PE, 20/128 with unknown etiology, and 16/128 with moderate PE – and in 13.51% (20/148) in the context of CAH as IC without RS.
Neonatal condition severity and the need for IC are determined by gestational age at delivery within the context of the specific IFG phenotype (FGR or SGA). For SGA, the critical risk threshold was 39 weeks (χ²=48.57, p<0.001; OR = 22.24) (Fig. 3a), whereas in FGR the threshold for adverse neonatal outcome shifted to earlier gestational ages – delivery before 35 weeks was associated with a 100% requirement for IC, including RS (χ²=535.21, p<0.001) (Fig. 3b).
The decision trees (classification/regression) constructed in this study allowed further characterization of the relationship between neonatal IC requirements (including RS) and maternal factors. First, we present the classification tree predicting neonatal IC requirement by IFG phenotype (FGR or SGA) and etiology (Fig. 4).
IC+RS was most probable in FGR with severe PE (Node 7) and moderate PE (Node 8). In the FGR subgroup (Node 2), the classification tree did not predict IC without RS as an outcome; IC without RS was more probable in patients with unknown etiology (Node 5) and was the exclusive outcome in CAH, GDM, type 1 DM, and GAH (Node 6). In the SGA subgroup (Node 3), IC without RS was predicted for CAH and GAH (Node 10), while absence of IC requirement was more probable with unknown etiology (Node 9) and unconditional with GDM (Node 11).
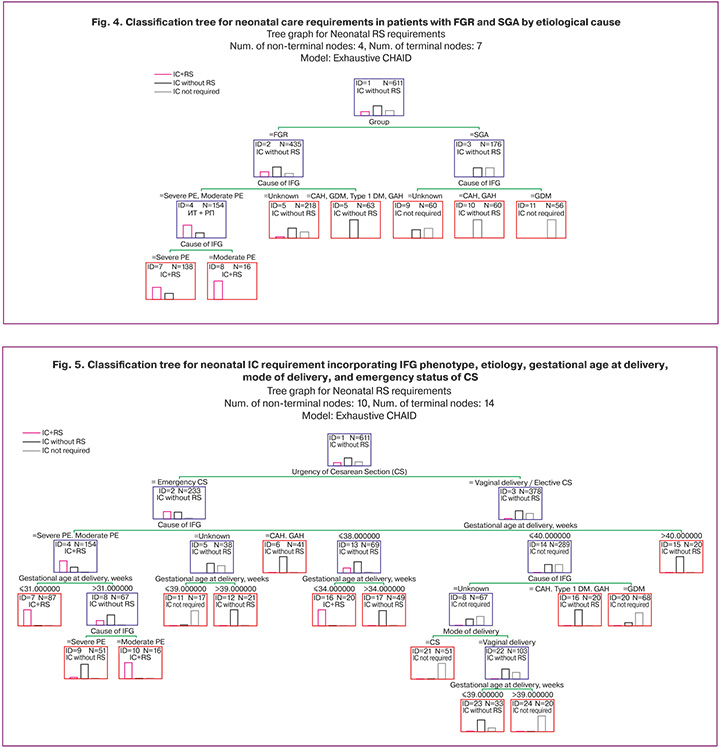
An attempt to predict neonatal IC requirement by incorporating additional variables – mode of delivery, emergency status of CS, indication for CS (maternal vs. fetal), intrapartum complications, and gestational age at delivery (Fig. 5) – yielded ambiguous results. During model construction, not all input variables were automatically selected; only IFG etiology, mode of delivery, emergency status of CS, and gestational age at delivery were retained. IFG phenotype, CS indication (maternal/fetal), and early or late postpartum complications were excluded by the algorithm.
Notably, the primary splitting rule was emergency CS status (Node 1). The requirement for IC+RS arises under the following conditions: gestational age ≤31.0 weeks (Node 7) + severe or moderate PE (Node 4) + emergency CS (Node 2); moderate PE (Node 10) + gestational age >31.0 weeks (Node 8) + emergency CS (Node 2); gestational age ≤34.0 weeks (Node 16) + vaginal delivery or elective CS (Node 3), regardless of IFG etiology. IC without RS is probable under the following conditions: severe PE (Node 9) + gestational age >31.0 weeks (Node 8) + emergency CS (Node 2); gestational age >39.0 weeks (Node 12) + unknown etiology (Node 5) + emergency CS (Node 2); CAH or GAH (Node 6) + emergency CS (Node 2), regardless of gestational age; gestational age >34.0 weeks (Node 17) + vaginal delivery or elective CS (Node 3), regardless of IFG etiology; gestational age ≤39.0 weeks (Node 23) + vaginal delivery (Node 22) + unknown IFG etiology (Node 18); CAH, type 1 DM, or GAH (Node 19) + gestational age 38.0–40.0 weeks (Node 14) + vaginal delivery or elective CS (Node 3); gestational age >40.0 weeks + vaginal delivery or elective CS (Node 3), regardless of IFG etiology. It is therefore evident that neonatal IC – both with and without RS – is not invariably linked to a specific IFG etiology or gestational age at delivery.
A regression tree (Fig. 6) further illustrates the expected probability of IC+RS not only in severe PE with extremely preterm or very preterm delivery – for both maternal indications (mean = 28.05 weeks; variance = 9.52 weeks) (Node 6) and fetal indications (mean = 29.76 weeks; variance = 5.10 weeks) (Node 7) – but also at or near term in the context of moderate PE (mean = 38.13 weeks; variance = 0.48 weeks) (Node 16) and severe PE (mean = 36.98 weeks; variance = 0.02 weeks) (Node 17) (highlighted with red dashed borders). Of concern is the probability of IC without RS associated with delayed delivery beyond the recommended window – for maternal indications at mean = 41.0 weeks (variance = 0.0 weeks) (Node 15), or for fetal indications at mean = 39.86 weeks (variance = 0.4 weeks) (Node 16) – in FGR (Node 11) with unknown etiology or GAH (Node 9).
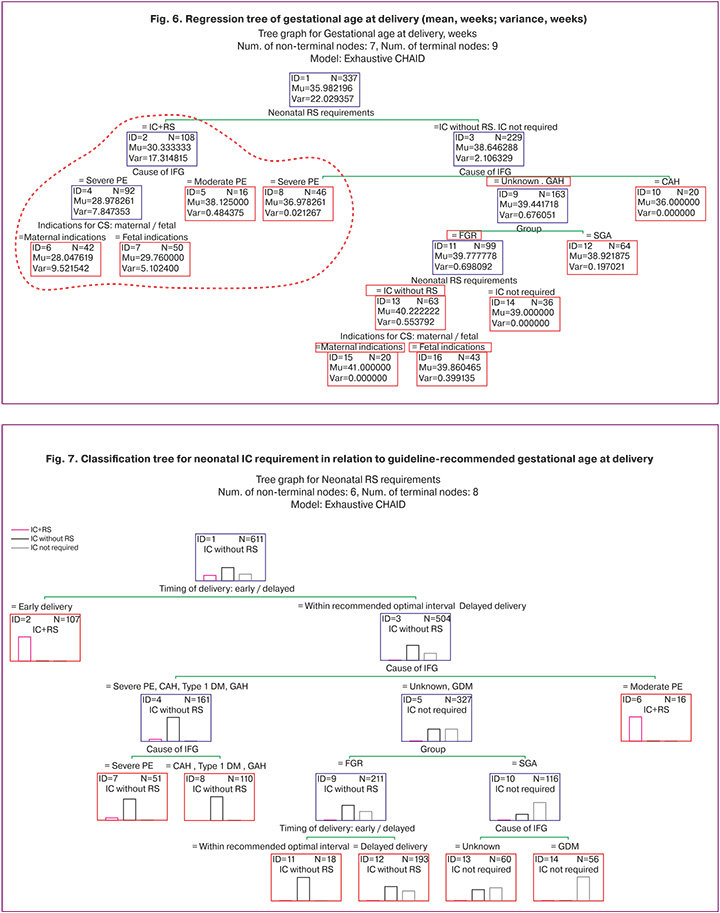
A further classification tree (Fig. 7) demonstrates the association between IC+RS and delivery preceding the "ideal" gestational window (Node 2), independent of IFG phenotype and etiology. Delivery within the recommended "normal" window – or beyond it – was highly probable for IC without RS in the context of severe PE, CAH, type 1 DM, and GAH (Nodes 7 and 8) and, critically, for IC+RS in the context of moderate PE (Node 6), regardless of IFG phenotype. With unknown etiology or GDM (Node 5) and FGR, IC without RS was highly probable both when delivery occurred within the recommended "normal" window (Node 11) and when it was delayed (Node 12); in SGA, IC was not required (Nodes 13 and 14).
Discussion
The clinical importance of IFG diagnosis stems from the difficulty in distinguishing between its phenotypes, FGR and SGA. The latent risks associated with each phenotype create uncertainty regarding pregnancy management and delivery timing. While the central role of placental pathology in FGR, including malperfusion and villitis, is well established [6], the SGA phenotype is often perceived as having a more favorable prognosis. For obstetricians and gynecologists, understanding the contribution of maternal factors to IFG pathogenesis and neonatal outcomes is critically important.
Established risk factors for FGR include maternal age, socioeconomic deprivation, smoking status, substance misuse, body mass index (BMI), and race. Additionally, chronic maternal comorbidities, such as pre-existing coagulopathies, pregestational diabetes mellitus, severe cardiopulmonary or renal disease, and anemia, as well as gestational complications such as PE, GAH, and GDM, are closely linked to placental insufficiency syndrome [2, 6, 7]. Consequently, comprehensive maternal history-taking remains a clinical priority for identifying potential placental and non-placental risk factors, preterm birth risk factors [9], and indicators warranting IFG screening and diagnostic evaluation [10]. The present study demonstrated that maternal comorbidity confers a substantial risk of SGA fetuses and newborns, comparable to that observed in FGR. These findings suggest that reduced fetal growth in the presence of maternal disease should not be regarded as a physiological variant.
Despite significant advancements in understanding IFG pathogenesis and the availability of sophisticated diagnostic technologies, many innovations remain inaccessible in routine clinical practice settings. This may partly explain the persistently high rates of missed antenatal diagnoses of SGA and FGR, reported as 78.7% in one study, including the absence of appropriate ultrasound evaluation in 47.1% of patients [8], and as high as 90% [7] or 95% [11] in others. In the present study, IFG was diagnosed in all cases; however, delayed delivery remained a significant issue, potentially reflecting a delayed diagnosis. Because FGR and SGA lack specific clinical manifestations, differential diagnoses rely primarily on ultrasonographic criteria established by the international Delphi consensus recommendations [1]. These criteria included the identification of abnormal cardiotocography findings from 32 weeks of gestation, absent end-diastolic umbilical artery flow from 32 weeks, reversed end-diastolic flow from 30 weeks, and abnormalities of ductus venosus blood flow, including absent or reversed a-wave, from 26 weeks of gestation on Doppler ultrasonography. Evaluation of maternal comorbidities and gestational complications, together with prompt delivery when indicated, is integral to management. Nevertheless, limited diagnostic resources and challenges in maternal referral pathways are not the only obstacles in managing pregnancies complicated by IFG.
Timely diagnosis is further complicated by the fact that placental insufficiency is idiopathic in approximately 60% of cases [12]. Idiopathic and unclassified FGR have long been recognized [13], with some studies suggesting that idiopathic cases account for up to 70% of all FGR diagnoses [14]. Missed SGA diagnoses occur most frequently among women considered to be at low risk; notably, 68.5% have no clear indication for screening ultrasound examinations [8].
Emerging approaches for the early detection of FGR include analyses of microRNA regulation [15], the systemic immune-inflammation index [16], and biomarkers of oxidative stress in neonatal cord blood. These include malondialdehyde, superoxide dismutase, catalase, ischemia-modified albumin, homocysteine, nitric oxide, and nucleated red blood cells [17]. Additionally, first-trimester biomarkers predictive of early onset FGR, such as soluble neuropilin-1 (sNRP-1), soluble platelet and endothelial cell adhesion molecule-1 (sPECAM-1), and platelet-derived growth factor (PDGF-AB/BB), are being investigated [18]. Other mechanisms being explored include impaired placental glucose transport mediated through the phosphatidylinositol 3-kinase/protein kinase B signaling pathway and regulated by peroxisome proliferator-activated receptor gamma (PPAR) [19]. However, these approaches remain largely inaccessible in routine clinical practice. Furthermore, although early onset FGR is defined as occurring before 32 weeks of gestation, no lower gestational age threshold has been established. Ideally, to avoid missed diagnoses, pregnant women should undergo the third screening examination at 30–31 weeks rather than after 32 weeks within the remaining recommended window extending to 34 weeks.
The complex etiology of IFG limits both diagnostic capabilities and therapeutic options, thereby increasing the importance of appropriate delivery timing [6]. This challenge is compounded by the fact that FGR is historically classified as a major obstetric syndrome, along with PE, preterm birth, placental abruption, and stillbirth [20], all of which share common features, exhibit dynamic molecular alterations in early pregnancy [22], and frequently coexist. Consequently, selecting an appropriate delivery setting remains a key strategy for reducing perinatal mortality [7].
Respiratory distress syndrome, the need for mechanical ventilation, and necrotizing enterocolitis are characteristic components of composite adverse neonatal outcomes [11]. The challenge of delivery timing extends beyond prematurity in FGR, encompassing iatrogenic prematurity in patients with PE and CAH. Particularly concerning is the strong association between neonatal intensive care admission among infants with SGA and delivery before 39 weeks of gestation, despite the fact that this gestational age represents the recommended upper limit for delivery [1,22]. Compared with infants of appropriate gestational age, SGA newborns are at an increased risk of adverse neonatal outcomes due to hypothermia and hypoglycemia resulting from reduced fat stores, lower glycogen reserves, and decreased levels of free fatty acids and ketone bodies [23]. Moreover, perinatal complications may contribute to the development of long-term sequelae. Children with a history of FGR have an increased risk of neurodevelopmental impairment during childhood and of cardiovascular disease, metabolic syndrome, including obesity, insulin resistance, dyslipidemia, and type 2 diabetes later in life [19]. Likewise, SGA infants often require growth hormone therapy [24].
There is currently considerable interest in developing predictive models capable of capturing the interactions between maternal risk factors and perinatal morbidity. Such models may reveal latent relationships between IFG and maternal age, comorbidities, progesterone therapy, and other relevant variables [24]. The present study demonstrated that the interval between the second (18–20+6 weeks) and third (30–34 weeks) screening examinations represent a vulnerable period during which IFG may be missed. This missed window can lead to lost opportunities for prevention, targeted treatment of modifiable complications (PE, GAH, CAH, GDM, and type 1 DM), and timely deliveries. An unknown cause of IFG may warrant more comprehensive maternal evaluation, including the assessment of genetic, infectious, extragenital, environmental, and placental factors, as well as individualized management and delivery planning, particularly when severe fetal or neonatal outcomes are anticipated. Early prediction of IFG and accurate distinction between SGA and FGR may be a key step toward overcoming these challenges [25], and the classification tree models presented in this study may contribute to this goal.
Conclusion
Latent IFG-related risks, in addition to maternal cardiometabolic disorders, were present in 45.5% of patients. These risks complicate diagnosis both before the third screening examination and at term, contributing to missed opportunities for delivery within the optimal gestational window, particularly in the case of FGR. Patients with IFG are at increased risk of emergency delivery and prematurity (34.02%, including extreme prematurity), of which 86.49% is iatrogenic. They also face worsening fetal compromise associated with precipitous and dysfunctional labor. SGA, often considered a constitutional fetal characteristic, may occur in the presence of GAH, CAH, or GDM. Neonatal intensive care (IC) was required in 73.16% of cases, and 20.95% of these infants additionally required respiratory support (RS), exclusively among those with FGR. Prematurity was unequivocally associated with the need for IC (100%).
The second screening examination should play a central role in stratifying patients at high risk for early onset FGR, uteroplacental and fetoplacental blood flow abnormalities, and critical fetal compromise before 30 weeks of gestation, even in the absence of maternal comorbidity. Timely diagnosis of chronic maternal cardiometabolic disorders (CAH, GDM, and type 1 DM) and gestational complications (GAH, PE, and GDM) may facilitate the early identification of FGR and SGA. This, in turn, enables the determination of the optimal timing and location of delivery to minimize neonatal risks.
References
- Министерство здравоохранения Российской Федерации. Клинические рекомендации. Недостаточный рост плода, требующий предоставления медицинской помощи матери (задержка роста плода). M.; 2022. 73 c. [Ministry of Health of the Russian Federation. Clinical guidelines. Insufficient fetal growth that requires medical assistance for the mother (fetal growth retardation). Moscow; 2022. 73 p. (in Russian)].
- Chew L.C., Osuchukwu O.O., Reed D.J., Verma R.P. Fetal growth restriction. [Updated 2024 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls publ.; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562268
- Liauw J., Gordijn S.J., Ganzevoort W., Mayer C., Hutcheon J.A. Antenatal diagnosis of early–onset small for gestational age: absolute and relative risks of adverse outcomes. Am. J. Obstet. Gynecol. 2025; 233(4): 329.e1-e14. https://dx.doi.org/10.1016/j.ajog.2025.04.041
- Huang B., Wang H., An Z., Yang Z., Cao J., Wang L. et al. Compromised peroxisome proliferator-activated receptor γ-mediated impaired placental glucose transport via the phosphatidylinositol 3-kinase/protein kinase B signaling pathway is associated with fetal growth restriction. Lab. Invest. 2025; 105(4): 104103. https://dx.doi.org/10.1016/j.labinv.2025.104103
- Столярова Е.В., Холин А.М., Ходжаева З.С., Гус А.И. Допплеровская оценка церебрального кровотока в дифференциальной диагностике поздней задержки роста плода. Акушерство и гинекология. 2025; 8: 88-98. https://dx.doi.org/10.18565/aig.2025.184 [Stoliarova E.V., Kholin A.M., Khodzhaeva Z.S., Gus A.I. Doppler evaluation of cerebral blood flow in the differential diagnosis of late-onset fetal growth restriction. Obstetrics and Gynecology. 2025; (8): 88-98 (in Russian). https://dx.doi.org/10.18565/aig.2025.184].
- Kamphof H.D., Posthuma S., Gordijn S.J., Ganzevoort W. Fetal growth restriction: mechanisms, epidemiology, and management. Matern. Fetal. Med. 2022; 4(3): 186-196. https://dx.doi.org/10.1097/FM9.0000000000000161
- Mattioli K.P., Sanderson M., Chauhan S.P. Inadequate identification of small-for-gestational-age fetuses at an urban teaching hospital. Int. J. Gynaecol. Obstet. 2010; 109(2): 140-3. https://dx.doi.org/10.1016/j.ijgo.2009.11.023
- Relph S., Vieira M.C., Copas A., Alagna A., Page L., Winsloe C. et al. Characteristics associated with antenatally unidentified small-for-gestational-age fetuses: prospective cohort study nested within DESiGN randomized controlled trial. Ultrasound. Obstet. Gynecol. 2023; 61(3): 356-66. https://dx.doi.org/10.1002/uog.26091
- Bray G., Maksym K., Dilipkumar M., Spencer R.N., Ginsberg Y., Weissbach T. et al. Economic impact of severe early-onset foetal growth restriction: a multicentre prospective cohort study. BJOG. 2026; 133(1): 61-70. https://dx.doi.org/10.1111/1471-0528.18266
- Villalaín C., Herraiz I., Akolekar R., Figueras F., Crispi F., Rizzo G. et al. Clinical practice guidance for the management of fetal growth restriction: an expert review. J. Matern. Fetal. Neonatal. Med. 2025; 38(1): 2526111. https://dx.doi.org/10.1080/14767058.2025.2526111
- Pineles B.L., Mendez-Figueroa H., Chauhan S.P. Diagnosis of fetal growth restriction in a cohort of small–for–gestational–age neonates at term: neonatal and maternal outcomes. Am. J. Obstet. Gynecol. MFM. 2022; 4(5): 100672. https://dx.doi.org/10.1016/j.ajogmf.2022.100672
- Malhotra A., Allison B.J., Castillo-Melendez M., Jenkin G., Polglase G.R., Miller S.L. Neonatal morbidities of fetal growth restriction: pathophysiology and impact. Front. Endocrinol. (Lausanne). 2019; 10: 55. https://dx.doi.org/10.3389/fendo.2019.00055
- Chandra N., Mehndiratta M., Banerjee B.D., Guleria K., Tripathi A.K. Idiopathic fetal growth restriction: repercussion of modulation in oxidative stress. Indian. J. Clin. Biochem. 2016; 31(1): 30-7. https://dx.doi.org/10.1007/s12291-015-0487-z
- Chui A., Murthi P., Gunatillake T., Brennecke S.P., Ignjatovic V., Monagle P.T. et al. Altered decorin leads to disrupted endothelial cell function: a possible mechanism in the pathogenesis of fetal growth restriction? Placenta. 2014; 35(8): 596-605. https://dx.doi.org/10.1016/j.placenta.2014.05.009
- Забанова Е.А., Кузнецова Н.Б., Шкурат Т.П., Бутенко Е.В. МикроРНК регуляция в генезе задержки роста плода. Акушерство и гинекология. 2019; 12: 5-11. https://dx.doi.org/10.18565/aig.2019.12.5-11 [Zabanova E.A., Kuznetsova N.B., Shkurat T.P., Butenko E.V. MicroRNA regulation in the genesis of fetal growth delay. Obstetrics and Gynecology. 2019; (12): 5-11 (in Russian). https://dx.doi.org/10.18565/aig.2019.12.5-11].
- Aktemur G., Çakır B.T., Karabay G., Filiz A.A., Seyhanlı Z., Sucu S.T. et al. Second-trimester inflammatory markers in predicting fetal growth restriction: a retrospective analysis. Am. J. Reprod. Immunol. 2025; 93(1): e70047. https://dx.doi.org/10.1111/aji.70047
- Li L., Zhou L., Li W., Shi F., Feng X., Zhuang J. Oxidative stress biomarkers in fetal growth restriction: a systematic review and meta-analysis. Arch. Gynecol. Obstet. 2025; 312(4): 1063-84. https://dx.doi.org/10.1007/s00404-025-08133-0
- Bai X., Li W., Ding W., Chan O.K., Leung M.B.W., Lau S.L. et al. New first trimester circulating angiogenic biomarkers in predicting early-onset and late-onset fetal growth restriction: a case-control study. BMC Pregnancy Childbirth. 2025; 25(1): 562. https://dx.doi.org/10.1186/s12884-025-07558-4
- Soler M., Parke B., Kim S.H., Terzidou V., Ladame S. Emerging biomarkers and diagnostic tools for the early prediction of adverse prenatal outcomes. npj Womens Health. 2026; 4: 20. https://dx.doi.org/10.1038/s44294-026-00138-7
- Hoffman M.K. The great obstetrical syndromes and the placenta. BJOG. 2023; 130(Suppl. 3): 8-15. https://dx.doi.org/10.1111/1471-0528.17613
- Zeng X., Gan Y., Zhao J., Zhang L., Zhang Q., Shen L. et al. Molecular profiles of the great obstetrical syndromes reveal common features and dynamic changes in early pregnancy. Commun. Med. (Lond). 2025; 5(1): 369. https://dx.doi.org/10.1038/s43856-025-01103-2
- Kazemier B.M., Voskamp B.J., Ravelli A.C., Pajkrt E., Groot C.J., Mol B.W. Optimal timing of delivery in small for gestational age fetuses near term: a national cohort study. Am. J. Perinatol. 2015; 30(2): 177-86. https://dx.doi.org/10.1055/s-0034-1381724
- Hokken-Koelega A.C.S., van der Steen M., Boguszewski M.C.S, Cianfarani S., Dahlgren J., Horikawa R. et al. International consensus guideline on small for gestational age: etiology and management from infancy to early adulthood. Endocr. Rev. 2023; 44(3): 539-65. https://dx.doi.org/10.1210/endrev/bnad002
- Zimmerman R.M., Hernandez E.J., Yandell M., Tristani-Firouzi M., Silver R.M., Grobman W. et al. AI-based analysis of fetal growth restriction in a prospective obstetric cohort quantifies compound risks for perinatal morbidity and mortality and identifies previously unrecognized high risk clinical scenarios. BMC Pregnancy Childbirth. 2025; 25(1): 80. https://dx.doi.org/10.1186/s12884-024-07095-6
- Зиядинов А.А., Новикова В.А., Радзинский В.Е. Прегестационное нейросетевое прогнозирование задержки роста плода или малого к гестационному возрасту плода с последующей интенсивной терапией новорожденного. Акушерство и гинекология. 2024; 10: 60-73. https://dx.doi.org/10.18565/aig.2024.124 [Ziyadinov A.A., Novikova V.A., Radzinsky V.E. Pregestational neural network prediction of fetal growth restriction or small-for-gestational-age fetus with subsequent intensive care of the newborn. Obstetrics and Gynecology. 2024; (10): 60-73 (in Russian). https://dx.doi.org/10.18565/aig.2024.124].
Received 20.02.2026
Accepted 09.06.2026
About the Authors
Arsen A. Ziyadinov, PhD, Associate Professor at the Department of Obstetrics, Gynecology and Perinatology No. 1, S.I. Georgievsky Medical Institute of V.I. Vernadsky Crimean Federal University; Obstetrician-Gynecologist, Perinatal Center of N.A. Semashko Republican Clinical Hospital, 295017, Russia, Republic of Crimea, Simferopol, Semashko str., 8; Doctoral student at the Department of Obstetrics and Gynecology with the Course of Perinatology, Medical Institute of Peoples’ Friendship Universityof Russia named after Patrice Lumumba, ars-en@yandex.ru
Vladislava A. Novikova, Dr. Med. Sci., Professor at the Department of Obstetrics and Gynecology with the Course of Perinatology, Medical Institute of Peoples’ Friendship University of Russia named after Patrice Lumumba, 117198, Russia, Moscow, Miklukho-Maklaya str., 6, vladislavan@mail.ru
Victor E. Radzinsky, Dr. Med. Sci., Professor, Corresponding Member of the RAS, Head of the Department of Obstetrics and Gynecology with the Course of Perinatology, Medical Institute of Peoples’ Friendship University of Russia named after Patrice Lumumba, 117198, Russia, Moscow, Miklukho-Maklaya str., 6, kafedra-aig@mail.ru
Similar Articles

