
Clinical and anamnestic predictors of implantation failures in women with diminished ovarian reserve: retrospective study
Dubinskaya E.D., Gasparov A.S., Mglinets A.P., Lukyanova Ya.S., Matskevich E.N.
Objective. To identify clinical and anamnestic predictors of implantation failures in women with diminished ovarian reserve, who underwent assisted reproductive technology (ART) cycles with good-quality embryo transfer.
Materials and methods. A retrospective analysis of medical records of 150 women of reproductive age
(20–35 years) with diminished ovarian reserve was performed. The women were divided into groups based on successful clinical pregnancies (n=58) or pregnancy failures (n=92) after two attempts of morphological good-quality embryo transfer. The data of reproductive and gynecological history, biomarkers of ovarian reserve, ovarian stimulation parameters, embryological characteristics, and endometrial sonographic parameters were analyzed. Statistical analysis included group comparisons, univariate logistic regression, calculation of odds ratios (OR) and 95% confidence intervals (95% CI).
Results. Significant predictors of implantation failure included primary infertility (OR=4.5), endometrial polyps (OR=4.6), previous surgery for ovarian endometriomas (OR=3.0), hypomenorrhea (OR=2.9), dysmenorrhea (OR=2.9), and adenomysosis (OR=2.3). Endometrial thickness <7.8 mm in the later stage of follicular phase was associated with a twofold increased risk of implantation failure (OR=2.7). There was no significant difference between the groups in ovarian response parameters and embryo quality.
Conclusion. In women of early and middle reproductive age with diminished ovarian reserve, implantation outcome after good-quality embryo transfer in ART programs can be determined by clinical and anamnestic factors. Decreased endometrial thickness in the later stage of the follicular phase of the menstrual cycle is a significant marker of implantation failure, indicating defective endometrial receptivity and displaced implantation window.
Authors' contributions. Dubinskaya E.D., Gasparov A.S. – the study concept and design, manuscript editing; Mglinets A.P., Lukyanova Ya.S., Matskevich E.N. – material collection and processing; Mglinets A.P., Dubinskaya E.D. – manuscript writing.
Conflicts of interest. The authors have no conflicts of interest to declare.
Funding. The study was carried out without any sponsorship.
Ethical Approval. The study was approved by the local Ethics Committee of Peoples' Friendship University of Russia named after Patrice Lumumba of the Ministry of Science and Higher Education of the Russian Federation.
Patient Consent for Publication. The patients have signed informed consent for publication of their data.
Authors' Data Sharing Statement. The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Dubinskaya E.D., Gasparov A.S., Mglinets A.P., Lukyanova Ya.S., Matskevich E.N. Clinical and anamnestic predictors of implantation failures in women with diminished ovarian reserve: retrospective study.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (5): 140-147 (in Russian)
https://dx.doi.org/10.18565/aig.2026.58
Keywords
diminished ovarian reserve
implantation
endometrium
assisted reproductive technologies
infertility
Implantation is the first step in interaction between embryo and endometrium and the starting point for successful pregnancy [1, 2]. Despite significant progress in the development of assisted reproductive technologies (ART), implantation success rate remains relatively low, and according to current reviews does not exceed 25–30% per embryo transfer [3].
Diminished ovarian reserve (DOR) means that the ovaries contain decreased quality and number of oocytes, and is clinically characterized by decreased anti-Müllerian hormone (AMH) level and antral follicle count (AFC), and elevated follicle-stimulating hormone (FSH) level. Diminished ovarian reserve is most often associated with age, but can be due to a number of other factors. Currently, about 20% of infertile patients have diminished ovarian reserve. At the same time, there is a trend toward progressive reduction in the ovarian reserve in the cohort of young women [4, 5].
The impact of DOR on clinical pregnancy rate remains disputable. For example, some authors reported that DOR has been found to reduce clinical pregnancy rate in women undergoing fresh embryo transfer [6]. At the same time, other studies showed that pregnancy rate is significantly lower in young patients with DOR than in young women with normal ovarian reserve [7].
Adequate good-quality embryo and endometrial receptivity are the factors for successful implantation [8]. There is published data on reduced chance of embryo implantation among young women with DOR, that is associated with concomitant mechanisms of endometrial aging [9].
The focus of research on the effectiveness of ART in patients with DOR is conventionally limited to embryo quantity and quality. At the same time, less attention is paid to the influence of endometrial factors and exploration of systemic changes in the reproductive system. It is most likely that DOR is both a result of some effect and a cause of systemic damage to the reproductive function, potentially leading to changes in endometrial receptivity.
There is lack of systematized data in available literature on analysis of implantation failures in women with DOR undergoing good-quality embryo transfer in the absence of endometrial changes diagnosed using traditional diagnostic methods.
In view of the above, the objective of this study was to assess clinical and anamnestic predictors of implantation failures in women with diminished ovarian reserve.
Materials and methods
This study was a retrospective analysis of medical documentation of 150 patients with diminished ovarian reserve, who underwent fertility treatment using ART at the clinic «I am healthy», the Department of Obstetrics and Gynecology with a course in Perinatology of Peoples' Friendship University of Russia named after Patrice Lumumba from 2023 to 2025.
The patients who met the inclusion criteria were consecutively recruited in the study. The patients who did not meet the inclusion criteria or had incomplete medical records were excluded from the study. The main group consisted of 92/150 (61%) patients, who had pregnancy failures after two attempts of embryo transfer. The comparison group consisted of 58/150 (39%) patients with the diagnosed ectopic pregnancy, which occurred after not less than 2 attempts of embryo transfer.
Inclusion criteria for both groups were the following: reproductive age of patients from 20 to 35 years, diminished ovarian reserve, undergoing IVF and good-quality embryo transfer (3АА – 6BB), as well as complete medical documentation. Diminished ovarian reserve was diagnosed based on the Bologna criteria of the European Society of Human Reproduction and Embryology, that ensured international comparability of data and standardized assessment of reproductive potential [10].
Exclusion criteria for both groups were the following: verified chronic endometritis (N71.1) at the time of embryo transfer, uterine polyps (N84.0), glandular endometrial hyperplasia (N85.0), adenomatous endometrial hyperplasia (N85.1), intrauterine synechias (N85.6), submucosal uterine fibroids (D25.0), premature ovarian failure (E28.3), polycystic ovary syndrome (E28.2), ovarian endometriosis (N80.1), benign ovarian tumors (D27) and other contraindications to ART according to the Order of the Ministry of Health of Russia of July 31, 202 No. №803n «On the procedure for using assisted reproductive technologies (ART), contraindications and restrictions on use.»
To identify potential predictors of implantation failure in each patient, 45 clinical and anamnestic parameters were collected and analyzed:
- patient social and health history including socio-demographic data (8 parameters): woman’s and partner’s age, duration of marriage, the age of sexual debut, place of residence, smoking, patient’s body mass index, age of menarche;
- reproductive anamnesis (8 parameters): duration and type of infertility, number of births, miscarriages, ectopic pregnancies, artificial abortions, time interval after last pregnancy (in secondary infertility), the number of ART cycles in history;
- gynecological anamnesis (10 parameters): endometrial polyps, uterine fibroids, adenomyosis, pelvic surgery including a history of surgery for ovarian teratomas, endometriomas, serous and mucinous cystadenomas, a history of bilateral tubectomy for hydrosalpinx treatment, presence of hypomenorrhea, dysmenorrhea;
- ovarian reserve measures (3 parameters): AMH, FSH levels, and AFC;
- hormonal profile and the features of assisted reproductive treatment (7 parameters): the levels of luteinizing hormone (LH), prolactin, estradiol, thyroid-stimulating hormone, the type of stimulation protocol, total dose of gonadotropins, characteristics of partner’s spermogram parameters.
- embyological parameters (5 parameters): numbers of obtained oocytes and mature oocytes (MII), the day of embryo transfer (morula/blastocyst transfer), number of transferred embryos, embryo quality;
- endometrial characteristics (4 parameters): endometrial thickness in the late follicular phase of the menstrual cycle (day 12), endometrial thickness on the day of progesterone initiation, trilaminar endometrial pattern, endometrial thickness uniformity.
This approach provided a comprehensive assessment of patients’ condition and enabled to identify the factors influencing the results of ART programs. The primary outcome measure was the onset of clinical pregnancy verified by ultrasound imaging of the gestational sac in the uterine cavity, that ensured objective and standardized assessment.
Statistical analysis
Statistical analysis was performed using software program StatTech v. 4.11.0 manufactured by LLC «Stattech», Russia.
Two-step analysis was performed to identify risk factors for implantation failures. Step 1. Comparative analysis of pregnancy outcomes in the groups.
The first step was comparison between the groups with successful implantation and implantation failures based on 45 analyzed parameters. The normality of distribution of the quantitative data was assessed using the Kolmogorov–Smirnov test. The normal sampling distribution of quantitative data were described using arithmetic means (M) and standard deviations (SD). Non-normal distribution of quantitative data was described as median (Me) and lower and upper quartiles (Q1; Q3). Normality of distribution of quantitative data with unequal variances was compared between the two groups using Welch's t-test. Non-normal distribution of quantitative data with equal variances was compared between the two groups using the Mann–Whitney U test. Comparison of the percentages in four-fold contingency tables was performed using the Pearson’s chi-squared test. The purpose of Step1 was to identify the parameters which were statistically different between the groups with different pregnancy outcomes. The differences were considered statistically significant at p<0.05.
Step 2. One factor regression analysis.
Each of 45 parameters as a potential predictor of implantation failure was tested using one factor logistic regression analysis. The relative variables were compared by calculation of the odds ratio (OR) as a quantitative measure of effect size with 95% confidence interval (95% CI). If contingency tables contained zero cells, the OR was calculated using the Haldane–Anscombe correction. ROC analysis was used to assess the ability of the parameters to differentiate between the groups with different outcomes. The ROC curve reflected the sensitivity and specificity ratios for various cutoff values, that made it possible to evaluate endometrial thickness and the occurrence of pregnancy. The cutoff value for the parameter was determined by the maximum value of the Youden index.
Results
The results of evaluation of the main characteristics of patients in the study groups is shown in Table 1.
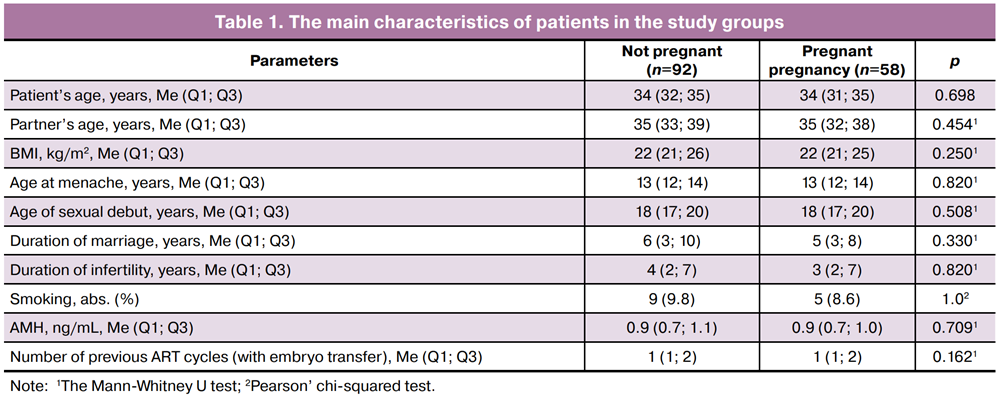
Analysis of social and demographic, clinical and anamnestic characteristics showed that the groups of patients who became pregnant and who had pregnancy failure were of comparable age, partners, body mass index, age at menarche, sexual debut, duration of marriage and infertility, number of previous ART cycles and smoking prevalence (Table 1). Also, there was no difference between the groups in ovarian reserve measures including AMH levels.
The results of ultrasound evaluation of endometrial characteristics in patients in the study groups are represented in Table 2.
Comparative analysis of sonographic characteristics of the endometrium showed that endometrial thickness in the late follicular phase of the menstrual cycle was significantly thinner in women who did not get pregnant (p<0.001) (Table 2). At the same time, there were no statistically significant differences in endometrial thickness on the day of progesterone initiation and echostructure parameters of the endometrium (trilaminar pattern, thickness uniformity). Ovarian stimulation parameters and ovarian response in patients in the study groups are represented in Table 3.
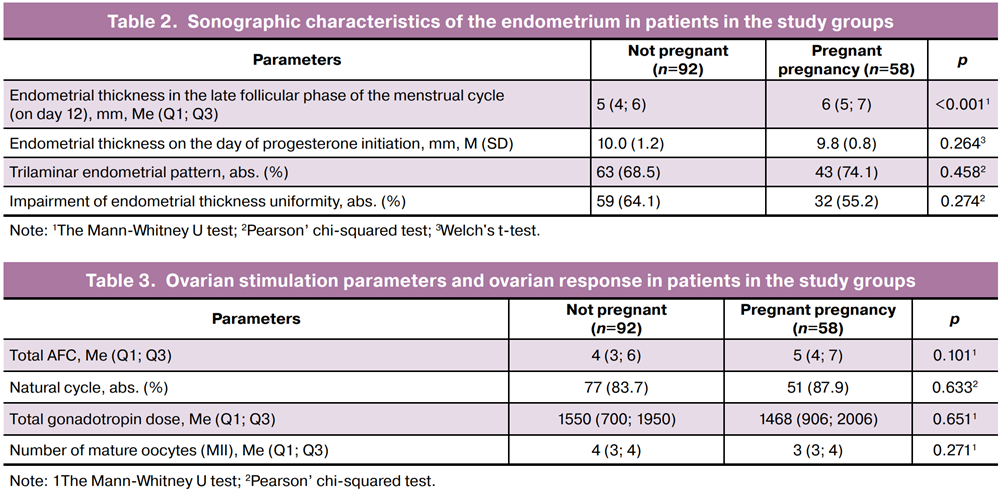
Comparative analysis of stimulation parameters and ovarian response found no statistically significant differences between the groups in AFC, the frequency of using natural cycle IVF, total gonadotropin dose, as well as the number of obtained mature oocytes. These data indicate that ovarian response and embryological potential in the study groups were comparable, suggesting that the differences in ART outcomes were not due to the characteristics of ovarian stimulation or oocyte number, but as a result of influence of other clinical and anamnestic factors.
ROC analysis was performed to assess the discriminatory ability of the endometrial thickness in the late follicular phase of the menstrual cycle in patients stratified by different pregnancy outcomes (Figure).
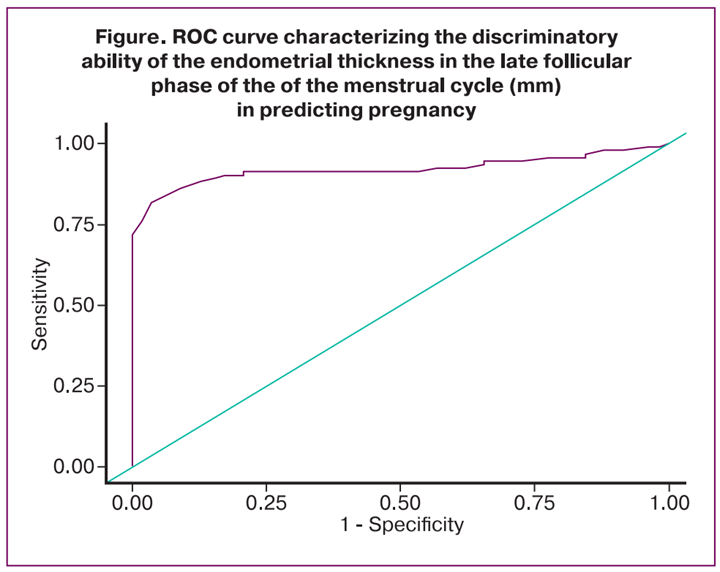
Figure. ROC curve characterizing the discriminatory ability of the endometrial thickness in the late follicular phase of the of the menstrual cycle (mm) in predicting pregnancy
Endometrial thickness in the late follicular phase of the menstrual cycle was significantly associated with the occurrence of pregnancy (AUC=0.920; 95% CI: 0.877–0.963, p<0.001). The threshold value of endometrial thickness in the late follicular phase of the cycle was 7.8 mm at the cut-off point associated with the maximum value of the Youden index (J=0.787). Endometrial thickness ≥7.8 mm was associated with the occurrence of pregnancy in the study groups. The sensitivity and specificity of the resulting predictive model were 81.5% and 96.6%, respectively.
One factor logistic regression analysis enabled to identify potential predictors of implantation failures and quantify their impact with the use of OR and 95% CI. The results of comparative analysis are represented in Table 4.
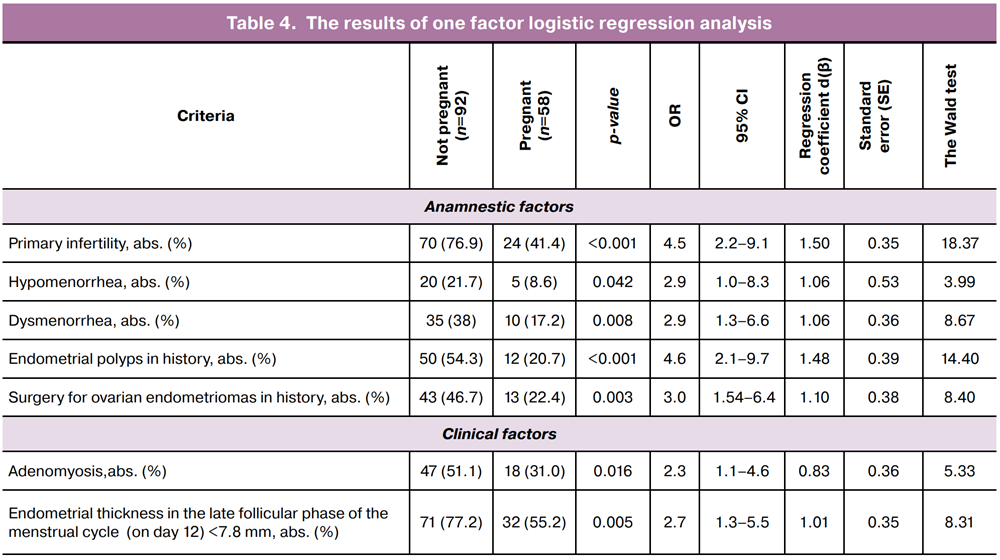
The results of analysis showed that the anamnestic factors of reproductive disorders were significantly more often in the group of patients who did not become pregnant. In particular, primary infertility significantly prevailed compared with the group of women who became pregnant (Table 4). Hypomenorrhea and dysmenorrhea showed similar trend, and were associated with reduced chances of getting pregnant. Endometrial polyps in history and past surgical history of ovarian endometriomas also were significantly more often observed in patients who did not become pregnant. In addition, endometrial thickness less than 7,8 mm in the late follicular phase of the menstrual cycle was significantly more often in the main group compared with the control group.
Discussion
Out study identified clinical and anamnestic factors associated with adverse outcomes of ART in women with diminished ovarian reserve, despite morphological good-quality embryo transfer and the absence of verified intrauterine pathology. This makes it possible to consider the identified factors as potential predictors of functional rather than morphological endometrial dysfunction. The obtained results are consistent with modern concepts of significant influence of previous gynecological pathology and the features of reproductive history on endometrial receptivity, and accordingly, a chance of successful implantation [11, 12]. It is well known that about one-third of all implantation failures are associated with embryo quality, while the remaining two-thirds are due to a decline in endometrial receptivity and compromised embryo-endometrial dialogue [13].
The endometrium is a unique and dynamic tissue that undergoes cyclical desquamation, regeneration and remodeling. These changes are regulated by estrogens and progesterone produced by the ovaries. Spatiotemporal changes in the endometrium are also controlled by paracrine mechanisms, cytokines, and growth factors generated by multiple endometrial cell including epithelial cells, stromal cells, local immune cells, and blood vessels [14]. It is obvious that any factors that disrupt paracrine and autocrine signaling pathways regulating endometrial function can lead to endometrial dysfunction. The purpose of our study was to identify these external factors in patients with diminished ovarian reserve.
Among the analyzed concomitant factors, primary infertility and endometrial polyps in history showed the strongest association with implantation failures. It is most likely that duration of infertility and primary infertility can reflect severe and long-term functional changes in the endometrium that leads to failed implantation. This is consistent with the data on a higher frequency of functional endometrial disorders in patients with a long history of infertility [15, 16]. At the same time, the data in other studies show that unification of ART protocols and taking into consideration concomitant factors, the difference between primary and secondary infertility in implantation rates can be smoothed. Actually, primary infertility reflects the accumulated reproductive risk in a broad sense, rather than endometrial quality [17, 18].
The results of our study are of particular interest indicating that decreased endometrial thickness (<7,8 mm) in the late follicular phase in the absence of evident differences in the sonographic characteristics of the endometrium in the secretory phase is an important sign, and is significantly associated with implantation rate. The obtained results are consistent with the data in literature, and confirm that endometrial thickness correlates with the frequency of clinical pregnancy, implantation and live birth rates in ART protocols for fresh and cryopreserved embryo transfer, and can serve as an available marker of functional receptivity [19, 20]. At the same time, other studies reported that successful implantation is possible even when endometrial thickness is less than 6–7 mm, since endometrial thickness reflects neither the molecular profile of the implantation window nor the state of the vascular bed and oxygen gradient in the endometrium. Therefore, thin endometrium is considered as a non-specific marker of reduced proliferative activity and impaired functional receptivity. Its informativeness increases significantly in combined assessment of echostructure, perfusion, and clinical and anamnestic characteristics [21].
Analysis of the impact of endometriosis highlighted indirect adverse effect of this disease on ART outcomes. Despite the fact that endometriosis is associated with chronic inflammation and changes in the endometrial immune microenvironment, the published data indicate that clinical pregnancy and live birth rates are preserved in patients who have no ovarian damage following surgery [22]. At the same time, there are data on the negative impact of endometriosis on implantation potential of the endometrium. For example, in 2024 one study demonstrated that endometriosis can impair endometrial receptivity by reducing the expression of KLF15, which is associated with impaired formation of the implantation window [23]. Another study found dysregulation of HOXA10/HOXA11, integrins, and proinflammatory cytokines leading to decreased implantation potential of the endometrium [24]. All this suggests a possible role of impaired molecular mechanisms in the endometrium and subsequent failed implantation, that is confirmed by the results of our study (the patients with adenomyosis were more common in the group of women who did not become pregnant).
In our opinion, the identified clinical characteristics of patients with diminished ovarian reserve and implantation failures, such as dysmenorrhea, hypomenorrhea and endometrial polyps in history, are the markers of functional dysregulation of the endometrium [25, 26]. It seems obvious that in addition to the morphological changes in the endometrium verified by endometrial histopathology results, the functional properties of the endometrium which are determined by the quality of the intrauterine environment, the immune response, a complex of molecular and cellular mechanisms, and hormonal balance, are of key importance. Due to the above, despite significant advances in ART, even in obtaining good-quality embryo and full-fledged blastocyst formation, embryo-endometrial interaction can be disrupted [27–29].
Also of interest are the data in literature indicating that dysmenorrhea is predominantly associated with increased levels of prostaglandins (PGF2α and PGE2), which are known as chemical stimulators of uterine muscle and artery contractility inducing endometrial hypoxia [30]. It is probably that critical hypoxic changes in the endometrium, that are clinically manifested by dysmenorrhea in patients with diminished ovarian reserve are one of the pathogenetic causes of implantation failures in a number of cases, that requires further study and quantitative assessment.
Conclusion
In women of early and middle reproductive age with diminished ovarian reserve, implantation outcome after good-quality embryo transfer in ART programs is determined by clinical and anamnestic factors. Decreased endometrial thickness in the late follicular phase of the menstrual cycle is a significant marker of implantation failure, indirectly indicating defective endometrial receptivity and displaced implantation window.
The obtained results indicate that it is prudent to take into account clinical and anamnestic predictors and necessity of individual consulting of patients with diminished ovarian reserve when discussing potential outcomes of ART programs.
Limitations of the study. The limitations of our single-center retrospective study include the following: the identified associations should be considered hypothesis-generating and require further validation, especially taking into consideration one factor logistic regression analysis using relatively small sample size. Future research should focus on multiple factor analysis having expansion cohort of patients, that will help clarify independent predictors and optimize individualized management strategies in ART.
References
- Ma J., Gao W., Li D. Recurrent implantation failure: a comprehensive summary from etiology to treatment. Front. Endocrinol. (Lausanne). 2023; 13: 1061766. https://dx.doi.org/10.3389/fendo.2022.1061766
- Karimi S., Baharaghdam S., Danaii S., Yousefi M. Embryo-maternal cross-talk: key players in successful implantation and live birth rates. Reprod. Biol. Endocrinol. 2025; 23(1): 136. https://dx.doi.org/10.1186/s12958-025-01477-x
- Bulletti F.M., Sciorio R., Conforti A., De Luca R., Bulletti C., Palagiano A. et al. Causes of embryo implantation failure: a systematic review and metaanalysis of procedures to increase embryo implantation potential. Front. Endocrinol. (Lausanne). 2025; 15: 1429193. https://dx.doi.org/10.3389/fendo.2024.1429193
- Erdoğan K., Şanlıer N., Utlu E., Güvey H., Kahyaoğlu İ., Neşelioğlu S. et al. Serum and follicular fluid thiol / disulfide homeostasis in diminished ovarian reserve patients undergoing in vitro fertilization / intracytoplasmic sperm injection treatment. Cureus. 2023; 15(2): e35476. https://dx.doi.org/10.7759/cureus.35476
- Choi R., Park W., Chun G., Lee S.G., Lee E.H. Investigation of the prevalence of diminished ovarian reserve in Korean women of reproductive age. J. Clin. Med. 2023; 12(15): 5099. https://dx.doi.org/10.3390/jcm12155099
- Zhu S., Jiang W., Liao X., Sun Y., Chen X., Zheng B. Effect of diminished ovarian reserve on the outcome of fresh embryo transfer in IVF / ICSI cycles among young women: a retrospective cohort study. BMC Womens Health. 2024; 24(1): 230. https://dx.doi.org/10.1186/s12905-024-03039-6
- Hu S., Xu B., Jin L. Perinatal outcome in young patients with diminished ovarian reserve undergoing assisted reproductive technology. Fertil. Steril. 2020; 114(1): 118-24.e1. https://dx.doi.org/10.1016/j.fertnstert.2020.02.112
- Mei Y., Wang Y., Ke X., Liang X., Lin Y., Wang F. Does endometrial receptivity array improve reproductive outcomes in euploid embryo transfer cycles? A systematic review. Front. Endocrinol. (Lausanne). 2023; 14: 1251699. https://dx.doi.org/10.3389/fendo.2023.1251699
- Liu F.X., Ming H.X., Huang K.L., Yi S.J., Liang X.F., Luo W.W. et al. Clinical pregnancy outcomes in young women with diminished ovarian reserve undergoing frozen embryo transfer: a comprehensive analysis with exploratory insights into endometrial aging. Front. Endocrinol. (Lausanne). 2025; 16: 1608200. https://dx.doi.org/10.3389/fendo.2025.1608200
- Ferraretti A.P., La Marca A., Fauser B.C.J.M., Tarlatzis B., Nargund G., Gianaroli L. ESHRE consensus on the definition of “poor response” to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum. Reprod. 2011; 26(7): 1616-24. https://dx.doi.org/10.1093/humrep/der092
- Maziotis E., Kalampokas T., Giannelou P., Grigoriadis S., Rapani A., Anifantakis M. Commercially available molecular approaches to evaluate endometrial receptivity: a systematic review and critical analysis of the literature. Diagnostics (Basel). 2022; 12(11): 2611. https://dx.doi.org/10.3390/diagnostics12112611
- Hiraoka T., Hirota Y., Osuga Y. How does adenomyosis impact endometrial receptivity? An updated systematic review of clinical and molecular insights. F&S Reviews. 2023; 4(1): 15-25. https://dx.doi.org/10.1016/j.xfnr.2022.11.004
- Lacconi V., Massimiani M., Carriero I., Bianco C., Ticconi C., Pavone V. et al. When the embryo meets the endometrium: identifying the features required for successful embryo implantation. Int. J. Mol. Sci. 2024; 25(5): 2834. https://dx.doi.org/10.3390/ijms25052834
- Wu J.X., Lin S., Kong S.B. Psychological stress and functional endometrial disorders: update of mechanism insights. Front. Endocrinol. (Lausanne). 2021; 12: 690255. https://dx.doi.org/10.3389/fendo.2021.690255
- Opuchlik K., Pankiewicz K., Pierzyński P., Sierdziński J., Aleksejeva E., Salumets A. et al. Factors influencing endometrial receptivity in women with recurrent implantation failure. BMC Women's Health. 2025; 25(1): 15. https://dx.doi.org/10.1186/s12905-024-03531-z
- Simon A., Laufer N. Repeated implantation failure: clinical approach. Fertil. Steril. 2012; 97(5): 1039-43. https://dx.doi.org/10.1016/j.fertnstert.2012.03.010
- Alson S., Stenqvist A., Sladkevicius P. Cumulative live birth rates under three consecutive IVF / ICSI treatment cycles are reduced in women with endometriosis and/or adenomyosis diagnosed by ultrasonography. Hum. Reprod. 2025; 40(12): 2332-41. https://dx.doi.org/10.1093/humrep/deaf184
- Базина М.И., Сыромятникова С.А., Емельянова Е.Ю., Савалова Н.С. Эффективность программ вспомогательных репродуктивных технологий у пациенток с трубным бесплодием в Красноярском крае. Доктор.Ру. Гинекология. 2015; 11(112): 8-12. [Bazina M.I., Syromyatnikova S.A., Emelianova E.Yu., Savalova N.S. Tubal infertility: effectiveness of assisted-reproductive technologies in women living in Krasnoyarsk region. Doctor.Ru. Gynecology. 2015; 11(12): 8-12 (in Russian)].
- Pérez-Milán F., Caballero-Campo M., Carrera-Roig M., Domínguez-Arroyo J.A., Moratalla-Bartolomé E., Alcázar-Zambrano J.L. et al. Impact of endometrial thickness on reproductive outcome in fresh and frozen-thawed embryo transfer: systematic review and meta-analysis. Ultrasound Obstet. Gynecol. 2025; 66(3): 271-81. https://dx.doi.org/10.1002/uog.29270
- Исакова Э.В., Савина В.А. Тонкий эндометрий в циклах вспомогательных репродуктивных технологий. Влияние на исходы беременности и лечение (обзор литературы, часть 2). Проблемы репродукции. 2021; 27(2): 65-75. [Isakova E.V., Savina V.A. Thin endometrium in ART treatment and outcome (literature review, part 2). Russian Journal of Human Reproduction. 2021; 27(2): 65-75 (in Russian)]. https://dx.doi.org/10.17116/repro20212702165
- Mathyk B., Schwartz A., DeCherney A., Ata B. A critical appraisal of studies on endometrial thickness and embryo transfer outcome. Reprod. Biomed. Online. 2023; 47(4): 103259. https://dx.doi.org/10.1016/j.rbmo.2023.103259
- Homer H.A. Effects of endometriosis on in vitro fertilisation - Myth or reality? Aust. N. Z. J. Obstet. Gynaecol. 2023; 63(1): 3-5. https://dx.doi.org/10.1111/ajo.13643
- Huang Y., Wang Z., Li B., Ke L., Xiong Y., Zhang Y. Loss of KLF15 impairs endometrial receptivity by inhibiting EMT in endometriosis. J. Endocrinol. 2024; 261(2): e230319. https://dx.doi.org/10.1530/JOE-23-0319
- Shan J., Li D.J., Wang X.Q. Towards a better understanding of endometriosis-related infertility: a review on how endometriosis affects endometrial receptivity. Biomolecules. 2023; 13(3): 430. https://dx.doi.org/10.3390/biom13030430
- Pîrlog L.M., Pătrășcanu A.A., Ona M.D., Cătană A., Rotar I.C. HOXA10 and HOXA11 in human endometrial benign disorders: unraveling molecular pathways and their impact on reproduction. Biomolecules. 2025; 15(4): 563. https://dx.doi.org/10.3390/biom15040563
- Gao Y., Hong X., Wang Z., Zhu Y. Endometrial receptivity and conception outcome among women with light menstrual bleeding of unidentified etiology. Int. J. Gynaecol. Obstet. 2018; 140(1): 37-41. https://dx.doi.org/10.1002/ijgo.12335
- Maldonado Rosas I., Mottola F., Palmieri I., Ibello L., Kalita J.C., Roychoudhury S. Molecular biomarkers of endometrial function and receptivity in natural and stimulated assisted reproductive technology (ART) cycles. Reprod. Med. 2026; 7(1): 2. https://dx.doi.org/10.3390/reprodmed7010002
- Жылкыбаева И.М., Клюев Д.А., Огизбаева А.В., Омертаева Д.Е., Камышанский Е.К. Маркеры рецептивности эндометрия: современные представления и клиническое значение. Репродуктивная медицина (Центральная Азия). 2025; 4: 31-44. [Zhylkybayeva I., Klyuyev D., Ogizbayeva A., Omertayeva D., Kamyshansky Y. Markers of endometrial receptivity: modern concepts and clinical significance (a literature review). Reproductive Medicine (Central Asia). 2025; 4: 31-44 (in Russian)]. https://dx.doi.org/10.37800/RM.4.2025.637
- Rackow B.W., Jorgensen E., Taylor H.S. Endometrial polyps affect uterine receptivity. Fertil. Steril. 2011; 95(8): 2690-2. https://dx.doi.org/10.1016/j.fertnstert.2010.12.034
- Obayashi S., Ideno Y., Kubota T., Takamatsu K., Hayashi K. Associations between lifestyle factors and primary dysmenorrhea in the Japan nurses’ health study. Women’s Health Rep. 2025; 6(1): 702-10. https://dx.doi.org/10.1177/26884844251362183
Received 16.02.2026
Accepted 17.03.2026
About the Authors
Ekaterina D. Dubinskaya, Dr. Med. Sci., Professor at the Department of Obstetrics, Gynecology and Perinatology, Medical Institute, Peoples’ Friendship University of Russia named after Patrice Lumumba, 8 Miklukho-Maklaya str., Moscow, 117198, Russia, +7(903)117-55-58, eka-dubinskaya@yandex.ru, https://orcid.org/0000-0002-8311-0381Alexander S. Gasparov, Dr. Med. Sci., Professor at the Department of Obstetrics, Gynecology and Perinatology, Medical Institute, Peoples’ Friendship University of Russia named after Patrice Lumumba, 8 Miklukho-Maklaya str., Moscow, 117198, Russia, +7(985)776-77-78, 13513520@mail.ru, https://orcid.org/0000-0001-6301-1880
Anna P. Mglinets, PhD Student, Department of Obstetrics, Gynecology and Perinatology, Medical Institute, Peoples’ Friendship University of Russia named
after Patrice Lumumba, 8 Miklukho-Maklaya str., Moscow, 117198, Russia, +7(906)056-49-98, mg.anna@mail.ru, https://orcid.org/0009-0001-3985-3954
Yana S. Lukyanova, Teaching Assistant at the Department of Obstetrics, Gynecology and Reproductive Medicine, Faculty of Postgraduate Education, Peoples’ Friendship University of Russia named after Patrice Lumumba, 8 Miklukho-Maklaya str., Moscow, 117198, Russia, +7(916)013-98-88, yana.lykuanova@gmail.com,
https://orcid.org/0000-0002-0083-9231
Elizaveta N. Matskevich, Teaching Assistant at the Department of Obstetrics, Gynecology and Reproductive Medicine, Faculty of Postgraduate Education, Peoples’ Friendship University of Russia named after Patrice Lumumba, 8 Miklukho-Maklaya str., Moscow, 117198, Russia, +7(911)176-66-94, liza151196chik@mail.ru,
https://orcid.org/0009-0000-3315-7408
Similar Articles

