
Exploration of bacterial biofilm formation on mesh implants used in surgical treatment of pelvic organ prolapse
Shalepo K.V., Khusnutdinova T.A., Budilovskaya O.V., Krysanova A.A., Rusina E.I., Tsypurdeeva A.A., Yarmolinskaya M.I., Savicheva A.M.
Objective. To explore in vitro bacterial biofilm formation on mesh implants used in surgical treatment of pelvic organ prolapse.
Materials and methods. The study used six fragments of medical mesh implants: polypropylene meshes Reperen, Russia (KS1), Gynemesh PS, USA (KS2), and titanium mesh Titanium Silk, Russia (KS3). Clinical bacterial isolates were obtained from the vaginal biotope. Biofilm forming bacteria were Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Streptococcus agalactiae, and Candida albicans. Biofilm formation capacity was determined in polystyrene flat-bottom plates. After co-cultivation of bacterial isolates and mesh fragments for 24 and 48 hours, biofilm formation on the bottom of the plate well and on the mesh surface was determined in optical density (OD) units.
Results. Bacterial biofilm formation did not occur on the surface of the investigated mesh implants within 24 or 48 hours. Optical density of the eluent during co-cultivation of polypropylene mesh and S. aureus was 0.174 and 0.179 after 24 and 48 hours, respectively, that was similar to OD of the negative control. Similar results were obtained for other investigated mesh implants.
Conclusion. Polypropylene and titanium mesh materials are highly resistant to microbial colonization and biofilm formation on their surfaces.
Authors' contributions. Shalepo K.V. – methodology, the study design and coordination, manuscript writing and editing; Khusnutdinova T.A., Budilovskaya O.V., Krysanova A.A. – participation in manuscript writing and editing; Rusina E.I. – study coordination, participation in manuscript writing and editing; Tsypurdeeva A.A., Yarmolinskaya M.I. – manuscript editing, approval of the final manuscript version; Savicheva A.M. – the study concept and coordination, manuscript editing, approval of the final manuscript version. The authors declare their authorship in compliance with the ICMJE criteria. The authors have made a significant contribution to the analytical search and preparation of the manuscript, read and approved the final version for publication.
Conflicts of interest. The authors confirm that they have no conflict of interest to declare.
Funding. The study was conducted within the framework of Fundamental scientific research topic No. 1024032800068-4-3.2.2 “Development of treatment strategies aimed at active longevity of women”.
Ethical Approval. The study was approved by the Expert Commission of D.O. Ott Research Institute of Obstetrics, Gynecology and Reproductology on January 13, 2026.
Authors' Data Sharing Statement. The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Shalepo K.V., Khusnutdinova T.A., Budilovskaya O.V., Krysanova A.A., Rusina E.I.,
Tsypurdeeva A.A., Yarmolinskaya M.I., Savicheva A.M. Exploration of bacterial biofilm formation
on mesh implants used in surgical treatment of pelvic organ prolapse.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (5): 99-106 (in Russian)
https://dx.doi.org/10.18565/aig.2026.17
Keywords
bacterial biofilms
vaginal microorganisms
mesh implant
Medical implants that are made of synthetic material have gained widespread use in reconstructive surgery. This has led to a serious medical and biological problem – increasing incidence of postoperative infectious complications [1]. In the pathogenesis of chronic, recurrent and treatment-resistant infections, the central issue is biofilm formation, that determines its high clinical and scientific significance.
A biofilm is an organized aggregate of microorganisms living within a self-produced matrix of extracellular polymeric substances (EPS) that is attached to a biotic or abiotic surface [2, 3]. The structure of biofilm provides bacterial survival. Biofilm formation protects microorganisms from the host immune system (phagocytosis, antibody action) and has up to 100–1000 times higher resistance to antimicrobial agents [4–6]. Biofilm facilitates the exchange of broad‐host‐range plasmids between bacteria, some of which carry multiple antibiotic resistance genes. Therefore, biofilms also pose a risk for the spread of antibiotic-resistant bacteria [7, 8].
Both gram-positive and gram-negative bacteria can form biofilms on the surfaces of medical devices. Among them the most common bacteria are Staphylococcus aureus, Pseudomonas aeruginosa, Klebsiella pneumoniae, Enterococcus faecalis, Staphylococcus epidermidis, and Escherichia coli. It has been found that Staphylococcus aureus and Staphylococcus epidermidis are the most common cause of biofilm-related infections on the surface of prosthetic heart valves and catheters [9]. Moreover, most infections associated with implanted devices are caused by staphylococcal species of Staphylococcus aureus-related complex, as well as coagulase-negative staphylococci species [9]. The process of bacterial biofilm formation on biotic and abiotic surfaces encompasses adsorption of opportunistic pathogens on the implant surface, attachment and colonization, maturation and formation of three-dimensional structures and channels that enhance the transport of nutrients, and dispersal, in other words, certain areas of the biofilm dissolve, releasing bacterial cells that can disperse and establish new colonies [10].
Currently, various types of prosthetic meshes are frequently used in hernioplasty and reconstructive gynecology for native tissue repair.
Due to good physical and biological properties, such as porous structure of polymer matrix, the polypropylene mesh is the most common type of mesh. Based on synthetic polymers, alternative antimicrobial meshes that can provide long-lasting solutions have been developed to impede bacterial infection, including those that are multidrug-resistant [11]. In recent years, titanium meshes have been used, which possess good histocompatibility. The data show that they exhibit good antibacterial activity against Staphylococcus aureus, reducing bacterial colonization by 99.4% during hernia repair surgery [12]. However, currently there is an unmet clinical need to explore their antibacterial activity in surgical treatment of pelvic organ prolapse in women.
The use of meshes in surgical treatment of pelvic organ prolapse in women is associated with complications in some patients, and significantly reduce patients’ quality of life. This issue has recently become a topic of debates in public health involving national parliaments and regulatory bodies [1, 13]. It is believed that the occurrence of complications associated with mesh implants results from multifactorial processes, including the issues related to the materials used for surgical mesh, the use of surgical techniques, the diseases, and patient-related factors. However, infectious complications and the interaction between the mesh and microorganisms are less studied [14]. The study by Birolini C. et al. (2023) analyzed the use of mesh implants over two decades associated with the development of infectious complications. A total of 117 meshes were explanted from 100 patients, and 17 of them had more than one mesh inserted. Staphylococcus aureus, isolated in 64% of cultures, was the cause of most single bacterial infections, and it was a dominating bacteria in sinus surface of the mesh and infected seromas. Gram-negative bacteria of the Enterobacteriaceae family were found during implant removal in 35% of cases, that was a sign of polymicrobial infections [15].
Most implants were made of high-density polypropylene (112/117, 95.7%). Polyester implants were removed in 3 patients (2.6%), and composite meshes (polypropylene/ePTFEP) in 2 (1.7%) [15]. Most publications discuss predictors of infection, such as patient-related risk factors, mesh materials, location of mesh placement, and other operative and technical factors rather than microbiological data addressing treatment of chronic infection associated with mesh implants [16, 17]. Therefore, it is crucial to identify the infecting agents and their biofilm forming capacity to provide the best additional treatment and prevent reinfection after subsequent reconstructive surgeries [18–21]. There is a lack of studies on conventional assessment of implant properties related to their ability to form biofilms.
The objective of the study was to explore in vitro bacterial biofilm formation on mesh implants used in surgical treatment of pelvic organ prolapse.
Materials and methods
Three types of medical mesh implants were used in the study: polypropylene meshes Reperen, Russia (KS1), a non-porous mesh made of synthetic reinforced polymer and Gynemesh PS, Johnson&Johnson, USA (KS2); and titanium mesh Titanium Silk, Russia (KS3), which are used in pelvic prolapse surgery via vaginal or laparoscopic approach. Clinical isolates of pure cultures of microorganisms isolated from the vaginal biotope were used in the study. Biofilm forming bacteria were Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Streptococcus agalactiae, and Candida albicans. Semi-quantitative determination of biofilm formation was performed in polystyrene flat-bottomed plates (the modified method of Christensen G.D. et al., 1985) [22]. Solid and liquid nutrient media were used for culturing, storage, and further analysis: blood agar (BA) supplemented with 5% defibrinated blood, Sabouraud's Dextrose Agar and Broth (SDA and SDB), and trypticase soy broth (TSB) with 10% glycerol. Microorganism identification was performed using MALDI-TOF mass spectrometer (Bruker Microflex, Germany).
Solid nutrient medium was used for the growth of a 24-hour old pure culture of each clinical isolate of microorganisms. Then pure cultures were suspended in sterile saline using vortexing to break up all preexisting microbial cell clusters, achieving a turbidity of 0.5 McFarland standard corresponding to 108 CFU/mL.
Two polystyrene 24-well sterile plates were used to conduct the experiment. The meshes were cut under sterile conditions into 1 x 1 cm fragments, and subsequently aseptically placed on the bottom of a polystyrene plate, adding 450 µl of Tryptic Soy Broth (TSB) medium supplemented with 1% glucose. Further, 50 μl of bacterial suspension at a concentration of 108 CFU/mL was added to each well. A well containing microorganisms (the positive control) was used to monitor the viability and purity of each culture. The cultures from this well were inoculated onto the solid nutrient medium optimal for each microorganism. Nutrient medium TSB supplemented with 1% glucose without microorganisms and TSB with and TSB with mesh implant were used as the negative control. The plates were incubated for 24 and 48 hours at 37°C. The fragments of the KS1 and KS3 meshes were examined for 24 and 48 hours, whereas the KS2 mesh was examined for 24 hours due to the limited number of mesh fragments. After incubation, the wells were emptied by aspirating the nutrient medium and washed three times at room temperature with phosphate-buffered saline (PSB), pH 7.2, to remove non-attached (planktonic) bacteria.
Mesh fragments were transferred to the new wells, air-dried, and fixed in 96% ethanol. Also, 96% ethanol was added to the wells with mesh fragments to fix the biofilms. After incubation for 20 minutes at room temperature, the alcohol was drained off from the wells, which were left to air dry. To visualize the biofilms, 350 µl of 2% gentian violet was added to each well. The staining time was 15 minutes. Then the wells were rinsed with water and air-dried. Subsequently, 24-well plates were filled with 96% ethanol to elute the dye (300 µl of 96% ethanol was added to each well, covered with a lid, and left for 30 minutes at room temperature without shaking). The eluate from the stained wells of the 24-well plate was transferred to the 96-well plate, and the biofilm biomass was quantified by measuring the optical density (OD) of the eluted dye at 570 nm using the Tecan® Sunrise spectrophotometer (Austria). The intact medium without microorganisms served as the negative control K (-)
Interpretation of the results:
OD was used as an integral indicator of biomass (with higher OD biofilm mass was greater).
1) Absence of biofilm showed that OD of the sample was equal to the value of the negative control.
2) Presence of biofilm showed that OD of the sample exceeded the value of OD of the negative control by more than 2 times.
Results
The results of biofilm formation by different microorganisms on the well bottom of the polystyrene plate after co-cultivation with the fragments of the studied implants are presented in Table 1.
Figure 1 shows visualization of biofilms formation with the fragments of studied implants after incubation for 24 hours in all wells of the polystyrene plate
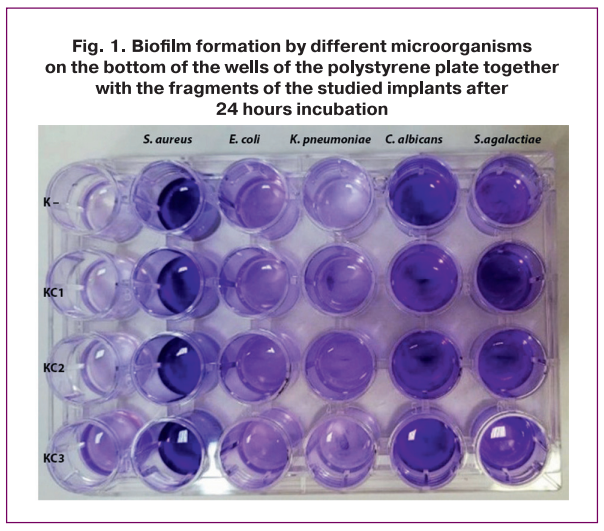
The result of semi-quantitative assessment of biofilm biomass on the bottom of the wells of the polystyrene plate after co-incubation of the fragments of three types of mesh implants with clinical isolates of pure cultures of microorganisms isolated from the vaginal biotope (Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Candida albicans and Streptococcus agalactiae) is presented in Table 1.
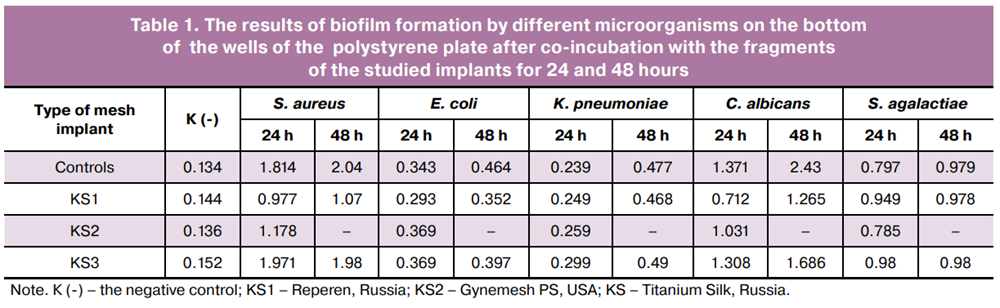
OD was used as an integral indicator of biomass (with higher OD biofilm mass was greater). Table 1 shows OD values for each of three implants: Reperen (KS1), Gynemesh PS (KS2), and Titanium Silk (KS3). Biofilm OD after co-cultivation of biofilm-forming microorganisms with the fragments of the studied implants for 24 and 48 hours are presented for the two types of implants. The fragments of the KS1 and KS3 meshes were examined for 24 and 48 hours, whereas the KS2 mesh was examined for 24 hours due to the limited number of mesh fragments.
Significantly increased values of OD were observed during the second day of incubation (from 24 to 48 hours), indicating the ongoing active process of biofilm formation by Candida albicans and Klebsiella pneumoniae on the surface of the wells of the polystyrene plate and biomass accumulation. Increased values of OD from 0.712 to 1.265 were registered for biofilm formation by Candida albicans in the wells with KS1, and from 1.308 to 1.686 in the wells with KS3 on the second day of incubation. The relative increase in biomass after 48 hours compared with incubation for 24 hours is 78% and 29%, respectively, indicating high metabolic activity and proliferative potential of yeast-like fungi in the studied time interval.
During Klebsiella pneumoniae biofilm formation in the wells with KS1, OD values increased from 0.249 after 24 hours to 0.468 after 48 hours and in the wells with KS3 from 0.299 to 0.490. The greatest relative increase in biofilm density was demonstrated after 48 hours compared with 24 hours (88 and 64%, respectively), that emphasizes the intensity of biofilm formation in this isolate after 48 hours.
During Escherichia coli biofilm formation in the wells with KS1, OD values slightly increased from 0.293 to 0.352 after 24 and 48 hours, and in the wells with KS3 from 0.369 to 0.397. No increase in biomass was noted for Streptococcus agalactiae and Staphylococcus aureus between 24 and 48 hours. Thus, assessment of biofilm formation in the wells with KS1 showed that OD values slightly changed – 0.949 and 0.978 for the Streptococcus agalactiae isolates, and 0.977 and 1.07 for the Staphylococcus aureus isolates. In wells with KS3, OD values did not change. OD values remained virtually constant, indicating that the biofilm entered a mature, stable plateau phase, where growth and division processes were balanced with cell lysis and desorption. In general, Table 1 shows that the examined microorganisms tenaciously formed dense biofilms on the polystyrene surface in the presence of mesh implants, while OD was slightly higher in the wells with the titanium material.
Visualization of biofilms on the surface of implants isolated from the plates after co-culturing is presented in Figure 2 and Table 2.
Figure 2 shows that the fragments of mesh implants are visualized in all wells.
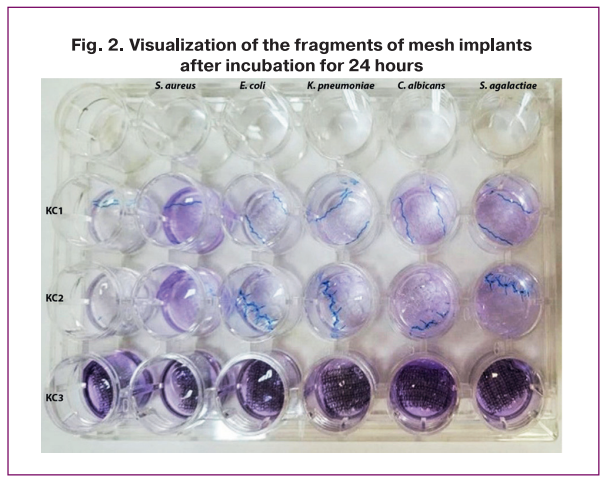
In each wells, we measured OD to determine whether biofilm remained on implant surfaces. The data are presented in Table 2.
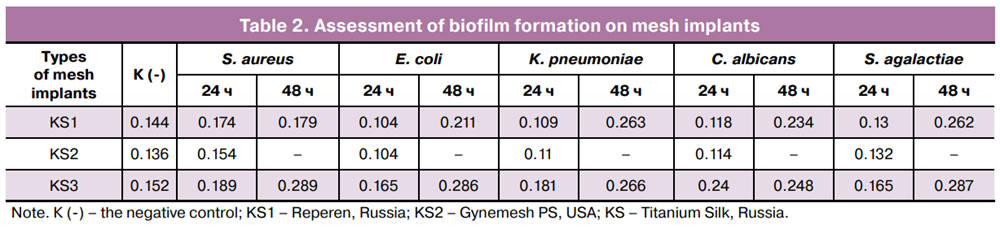
As is shown in Table 2, OD values for all microorganisms were within the range of values for the negative control. For example, for Reperen (KS1), OD of the eluate in the presence of Staphylococcus aureus was 0.174 and 0.179 after 24 and 48 hours, respectively, and almost did not differ from the control – 0.144. Similarly, OD values for titanium KS3 were in the range of 0.189–0.289, and were higher by 0.03 – 0.13 units compared with the control – 0.152. OD values of the eluate from the wells with mesh fragments after removal from culture medium after co-cultivation with microorganisms and OD in the control wells after 24 and 48 hours were almost similar, demonstrating the absence of biofilms on the surface of mesh implants.
Most combinations between 24 and 48 h showed a slight increase in OD (for example, OD of Klebsiella pneumonia on KS3 was from 0.181 to 0.266 and did not exceed the two-fold threshold specific for biofilm formation.
Optical density measurements of bacteria on Gynemesh PS were conducted only after 24 hours; OD values of Staphylococcus aureus – 0.154, Candida albicans – 0.114, Streptococcus agalactiae – 0.132 were comparable with the control – 0.136. Bacterial OD on the titanium implant was slightly higher than on the polypropylene implant, but did not exceed more than twofold. Thus, no biofilm formation was observed on implants made of the tested materials.
. In contrast to the data presented in Table 1, there were virtually no differences between the biofilm-forming microorganisms. Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Candida albicans, and Streptococcus agalactiae demonstrated similar levels of adherence to the mesh (OD ≈ 0.1–0.26). This indicates that the chemical and structural parameters of mesh implants prevent bacterial adherence, and the biofilm observed in the wells of the polystyrene plate formed predominantly on the plastic bottom.
Summarizing the data presented in Table 2, it is important to note that all examined mesh implants studied – Reperen, Gynemesh PS, and titanium mesh did not contribute to in vitro formation of stable biofilms on their surfaces. This is confirmed by the fact that OD of the stained eluate after removal of mesh fragments was virtually identical to the control, indicating the absence of significant bacterial and fungal adherence.
Thus, the results of this in vitro study showed no biofilm formation on mesh implants, such as Reperen (Reperen, Russia), a nonporous polypropylene mesh made of synthetic reinforced polymer, Gynemesh PS (Johnson & Johnson, USA), and titanium mesh (Titanium Silk, Russia), which are used in surgical treatment of pelvic organ prolapse via vaginal and laparoscopic approach. These results indicate high resistance of polypropylene and titanium mesh materials to bacterial colonization in vitro and confirm their biocompatibility when properly and sterilely implanted.
Discussion
Complications associated with the use of synthetic implants in surgical treatment of pelvic organ prolapse, such as chronic pelvic pain, vaginal mesh erosion, and recurrent infections, are largely mediated by biofilm formation. Bacterial biofilm formation on implantable and reusable medical devices significantly impacts surgical outcomes and patient’s quality of life, and in the occurrence of inflammatory complications leads to significant economic costs [1]. Using real-time PCR and next-generation sequencing (NGS), the study by Slade A. et al. (2022) found complex polymicrobial colonization of synthetic implants in patients with complications predominantly by Staphylococcus spp. (including Staphylococcus epidermidis), Escherichia coli, and anaerobic bacteria [23]. Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Candida albicans and Streptococcus agalactiae are commensal microbes that colonize vaginal microbiota of women before or during surgery, where they can subsequently contaminate the implants. Bacterial biofilm not only promotes sustained inflammation leading to erosion but also contribute to the development of fibrosis and contracture around the mesh fibers, that clinically manifests as chronic pelvic pain and dyspareunia [24]. Understanding therapeutic strategies against biofilm infection is an extremely complex issue. Antibiotics are effective against planktonic (free-living) forms and pure bacterial cultures, but do not penetrate the deep layers of polymicrobial biofilms. This leads to temporary symptom suppression and relapse after withdrawal of treatment [5]. Therefore, removal of implants remains the gold standard for treatment of confirmed biofilm-associated infections [1, 25, 26].
There are still lack of studies investigating infections associated with implants used for surgical correction of pelvic organ prolapse. The main diagnostic challenge in these studies is the difficulty in biofilm detection using the standard culture methods, that leads to false-negative results. Verification of biofilms requires more sophisticated methods: confocal laser scanning microscopy, real-time polymerase chain reaction, 16S rRNA gene sequencing, and mass spectrometry [27].
Our study is one of the first evaluating bacterial adherence and biofilm formation on implants using the method of culturing in polystyrene plates. Different modifications of this assay have been used to assess the ability of a wide range of microorganisms, including, but not limited to, pseudomonads, Vibrio cholerae, Escherichia coli, staphylococci, enterococci, mycobacteria, and fungi to form biofilms in the specific environment [22]. This method can be adapted to a wide range of microorganisms. Washing the wells with buffer removes most planktonic microorganisms. The optimal conditions for biofilm formation (growing medium, temperature, incubation time) should be determined empirically for each microbe [22].
Our experimental analysis of currently used monofilament polypropylene mesh implants and titanium thread implant (Titanium Silk), showed no biofilm formation on implant surfaces. Furthermore, no differences were observed between three types of implants made from different materials. Previous studies investigating different types of implants, which differed both in polymer type and the thread design yielded similar results. The study by Verhorstert K.W.J. et al. (2020) evaluated Escherichia coli biofilm formation on knitted polypropylene implants with different knitting designs and showed no biofilm formation on their surfaces. This was shown in images obtained using a scanning electron microscope, where only individual Escherichia coli bacteria were observed on fiber coating of the implant. The same study found that Staphylococcus aureus formed biofilms on the surfaces of all implants. The researchers explain it by the impact of human plasma in nutrient medium enhancing Staphylococcus aureus biofilm formation [28].
The limitation of our experiment is that we examined only one isolate of each bacteria Staphylococcus aureus, Escherichia coli, Klebsiella pneumoniae, Candida albicans, and Streptococcus agalactiae, while there are differences between clinical isolates of each species in adhesion capacity and biofilm formation. Furthermore, vaginal microflora is polymicrobial, and interspecies microbial interactions may influence biofilm formation. However, we have chosen these clinical bacterial isolates and yeast-like fungi for in vitro examination, since they form bacterial films with high OD, that allowed the appropriate assessment of bacterial adhesion and biofilm formation on the tested implants.
Thus, modern implants used in surgical treatment of pelvic organ prolapse in women showed resistance to biofilm formation on their surfaces.
Conclusion
Evolving views on the optimal approach to surgical treatment of pelvic organ prolapse are based on the latest data and events related to the use of synthetic implants. The problem of bacterial biofilm formation on gynecological implants is clinically significant. It underlies the majority of chronic and recurrent infectious complications, significantly reducing patients' quality of life and requiring complex and invasive interventions for their resolution. Current research is focused on development of new anti-biofilm strategies. Our experimental study demonstrated that modern monofilament polypropylene and titanium implants are associated with a low risk of bacterial adhesion and biofilm formation.
References
- Deffieux X., Perrouin-Verbe M.A., Campagne-Loiseau S., Donon L., Levesque A., Rigaud J. et al. Diagnosis and management of complications following pelvic organ prolapse surgery using a synthetic mesh: French national guidelines for clinical practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2024; 294(2): 170-9. https://dx.doi.org/10.1016/j.ejogrb.2024.01.015
- Donlan R.M., Costerton J.W. Biofilms: survival mechanisms of clinically relevant microorganisms. Clin. Microbiol. Rev. 2002; 15(2): 167-93. https://dx.doi.org/10.1128/CMR.15.2.167-193.20023
- Yin W., Wang Y., Liu L., He J. Biofilms: the microbial "protective clothing" in extreme environments. Int. J. Mol. Sci. 2019; 20(14): 3423. https://dx.doi.org/10.3390/ijms20143423
- Hall C.W., Mah T.F. Molecular mechanisms of biofilm-based antibiotic resistance and tolerance in pathogenic bacteria. FEMS Microbiol. Rev. 2017; 41(3): 276-301. https://dx.doi.org/10.1093/femsre/fux010
- Høiby N., Bjarnsholt T., Moser C., Bassi G.L., Coenye T., Donelli G. et al. ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin. Microbiol. Infect. 2015; 21 Suppl 1: S1-S25. https://dx.doi.org/10.1016/j.cmi.2014.10.024
- Roman S., Mangir N., Bissoli J., Chapple C.R., MacNeil S. Biodegradable scaffolds designed to mimic fascia-like properties for the treatment of pelvic organ prolapse and stress urinary incontinence. J. Biomater. Appl. 2016; 30(10): 1578-88. https://dx.doi.org/10.1177/0885328216633373
- Wi Y.M., Patel R. Understanding biofilms and novel approaches to the diagnosis, prevention, and treatment of medical device-associated infections. Infect. Dis. Clin. North Am. 2018; 32(4): 915-29. https://dx.doi.org/10.1016/j.idc.2018.06.009
- Francolini I., Donelli G. Prevention and control of biofilm-based medical-device-related infections. FEMS Immunol. Med. Microbiol. 2010; 59(3): 227-38. https://dx.doi.org/10.1111/j.1574-695X.2010.00665.x
- Khatoon Z., McTiernan C.D., Suuronen E.J., Mah T.F., Alarcon E.I. Bacterial biofilm formation on implantable devices and approaches to its treatment and prevention. Heliyon. 2018; 4(12): e01067. https://dx.doi.org/10.1016/j.heliyon.2018.e01067
- Omwenga E.O., Awuor S.O. The bacterial biofilms: formation, impacts, and possible management targets in the healthcare system. Can. J. Infect. Dis. Med. Microbiol. 2024; 2024: 1542576. https://dx.doi.org/10.1155/cjid/1542576
- Serrano-Aroca Á., Pous-Serrano S. Prosthetic meshes for hernia repair: state of art, classification, biomaterials, antimicrobial approaches, and fabrication methods. J. Biomed. Mater. Res. A. 2021; 109(12): 2695-719. https://dx.doi.org/10.1002/jbm.a.37238
- Calabrese G., Franco D., Petralia S., Monforte F., Condorelli G.G., Squarzoni S. et al. Dual-functional nano-functionalized titanium scaffolds to inhibit bacterial growth and enhance osteointegration. Nanomaterials (Basel). 2021; 11(10): 2634. https://dx.doi.org/10.3390/nano11102634
- Lin F.C., Gilleran J.P., Powell C.R., Atiemo H.O. To mesh or not mesh "apical prolapse," that is the question! Neurourol. Urodyn. 2024; 43(7): 1626-30. https://dx.doi.org/10.1002/nau.25469
- Mangir N., Roman S., Chapple C.R., MacNeil S. Complications related to use of mesh implants in surgical treatment of stress urinary incontinence and pelvic organ prolapse: infection or inflammation? World J. Urol. 2020; 38(1): 73-80. https://dx.doi.org/10.1007/s00345-019-02679-w
- Birolini C., Faro Junior M.P., Terhoch C.B., de Miranda J.S., Tanaka E.Y., Utiyama E.M. Microbiology of chronic mesh infection. Hernia. 2023; 27(4): 1017-23. https://dx.doi.org/10.1007/s10029-023-02747-6
- Cevasco M., Itani K.M. Ventral hernia repair with synthetic, composite, and biologic mesh: characteristics, indications, and infection profile. Surg. Infect. (Larchmt). 2012; 13(4): 209-15. https://dx.doi.org/10.1089/sur.2012.123
- Kao A.M., Arnold M.R., Augenstein V.A., Heniford B.T. Prevention and treatment strategies for mesh infection in abdominal wall reconstruction. Plast. Reconstr. Surg. 2018; 142(3S): 149S-55S. https://dx.doi.org/10.1097/PRS.0000000000004871
- Dipp Ramos R., O’Brien W.J., Gupta K., Itani K.M.F. Re-infection after explantation of infected hernia mesh: are the same micro-organisms involved? Surg. Infect. (Larchmt). 2021; 22(10): 1077-80. https://dx.doi.org/10.1089/sur.2021.142
- Birolini C., Tanaka E.Y., de Miranda J.S., Murakami A.H., Damous S.H.B., Utiyama E.M. The early outcomes of complex abdominal wall reconstruction with polyvinylidene (PVDF) mesh in the setting of active infection: a prospective series. Langenbecks Arch. Surg. 2022; 407(7): 3089-99. https://dx.doi.org/10.1007/s00423-022-02625-2
- Birolini C., de Miranda J.S., Tanaka E.Y., Utiyama E.M., Rasslan S., Birolini D. The use of synthetic mesh in contaminated and infected abdominal wall repairs: challenging the dogma-A long-term prospective clinical trial. Hernia. 2020; 24(2): 307-23. https://dx.doi.org/10.1007/s10029-019-02035-2
- Birolini C., de Miranda J.S., Utiyama E.M., Rasslan S. A retrospective review and observations over a 16-year clinical experience on the surgical treatment of chronic mesh infection. What about replacing a synthetic mesh on the infected surgical field? Hernia. 2015; 19(2): 239-46. https://dx.doi.org/10.1007/s10029-014-1225-9
- Christensen G.D., Simpson W.A., Younger J.J., Baddour L.M., Barrett F.F., Melton D.M. et al. Adherence of coagulase-negative staphylococci to plastic tissue culture plates: a quantitative model for the adherence of staphylococci to medical devices. J. Clin. Microbiol. 1985; 22(6): 996-1006. https://dx.doi.org/10.1128/jcm.22.6.996-1006.1985
- Slade E.A., Thorn R.M.S., Young A.E., Reynolds D.M. Real-time detection of volatile metabolites enabling species-level discrimination of bacterial biofilms associated with wound infection. J. Appl. Microbiol. 2022; 132(3): 1558-72. https://dx.doi.org/10.1111/jam.15313
- Ganj F.A., Ibeanu O.A., Bedestani A., Nolan T.E., Chesson R.R. Complications of transvaginal monofilament polypropylene mesh in pelvic organ prolapse repair. Int. Urogynecol. J. Pelvic. Floor Dysfunct. 2009; 20(8): 919-25. https://dx.doi.org/10.1007/s00192-009-0879-9
- Negut I., Albu C., Bita B. Advances in antimicrobial coatings for preventing infections of head-related implantable medical devices. Coatings. 2024; 14(3): 256. https://dx.doi.org/10.3390/coatings14030256
- Okui N., Okui M.A. Pathological insights on polypropylene mesh complications from laparoscopic sacrocolpopexy: a case series. Cureus. 2024; 16(3): e56354. https://dx.doi.org/10.7759/cureus.56354
- Franco-Duarte R., Černáková L., Kadam S., Kaushik K.S., Salehi B., Bevilacqua A. et al. Advances in chemical and biological methods to identify microorganisms-from past to present. Microorganisms. 2019; 7(5): 130. https://dx.doi.org/10.3390/microorganisms7050130
- Verhorstert K.W.J., Guler Z., de Boer L., Riool M., Roovers J.W.R., Zaat S.A.J. In vitro bacterial adhesion and biofilm formation on fully absorbable poly-4-hydroxybutyrate and nonabsorbable polypropylene pelvic floor implants. ACS Appl. Mater. Interfaces. 2020; 12(48): 53646-53. https://dx.doi.org/10.1021/acsami.0c14668
Received 11.01.2026
Accepted 23.04.2026
About the Authors
Kira V. Shalepo, PhD, Senior Researcher at the Experimental Microbiology Group, D.O. Ott Research Institute of Obstetrics, Gynecology and Reproductology, 3 Mendeleyevskaya Line, 199034, St. Petersburg, Russia, +7(911)247-41-51, 2474151@mail.ru, https://orcid.org/ 0000-0002-3002-3874Tatiana A. Khusnutdinova, PhD, Senior Researcher at the Experimental Microbiology Group, D.O. Ott Research Institute of Obstetrics, Gynecology and Reproductology, 3 Mendeleyevskaya Line, 199034, St. Petersburg, Russia, husnutdinovat@yandex.ru, https://orcid.org/0000-0002-2742-2655
Olga V. Budilovskaya, PhD, Senior Researcher at the Experimental Microbiology Group, D.O. Ott Research Institute of Obstetrics, Gynecology and Reproductology, 3 Mendeleyevskaya Line, 199034, St. Petersburg, Russia, o.budilovskaya@gmail.com, https://orcid.org/0000-0001-7673-6274
Anna A. Krysanova, PhD, Senior Researcher at the Experimental Microbiology Group, D.O. Ott Research Institute of Obstetrics, Gynecology and Reproductology, 3 Mendeleyevskaya Line, 199034, St. Petersburg, Russia, krusanova.anna@mail.ru, https://orcid.org/0000-0003-4798-1881
Elena I. Rusina, Dr. Med. Sci., Leading Researcher at the Experimental Microbiology Group, D.O. Ott Research Institute of Obstetrics, Gynecology and Reproductology, 3 Mendeleyevskaya Line, 199034, St. Petersburg, Russia, pismo_rusina@mail.ru, eLibrary SPIN: 3527-5104, https://orcid.org/0000-0002-8744-678X
Anna A. Tsypurdeeva, PhD, Senior Researcher at the Department of Gynecology and Endocrinology and Head of Gynecology Department I with an operating unit,
D.O. Ott Research Institute of Obstetrics, Gynecology, and Reproductology, 3 Mendeleyevskaya Line, 199034, St. Petersburg, Russia, tsypurdeeva@mail.ru,
eLibrary SPIN: 5208-9707, https://orcid.org/0000-0001-7774-2094
Maria I. Yarmolinskaya, Dr. Med. Sci., Professor, Professor of the Russian Academy of Sciences, Honored Scientist of the Russian Federation, Head of the Department of Gynecology and Endocrinology, Head of the Center of Diagnostics and Treatment of Endometriosis, D.O. Ott Research Institute of Obstetrics, Gynecology and Reproductology, 3 Mendeleyevskaya Line, 199034, St. Petersburg, Russia, m.yarmolinskaya@gmail.com, eLibrary SPIN: 3686-3605, https://orcid.org/0000-0002-6551-4147
Alevtina M. Savicheva, Dr. Med. Sci., Professor, Honored Scientist of the Russian Federation, Head of the Department of Medical Microbiology, D.O. Ott Research Institute
of Obstetrics, Gynecology and Reproductology, 3 Mendeleyevskaya Line, 199034, St. Petersburg, Russia, savitcheva@mail.ru, https://orcid.org/ 0000-0003-3870-5930
Corresponding author: Kira V. Shalepo, 2474151@mail.ru
Similar Articles

