
Photodynamic therapy as a contemporary treatment approach to Asherman’s syndrome
Pasman N.P., Selyunina N.A., Panova S.V., Karpets I.O., Sayapina S.I., Veretelnikova T.V., Shifon S.A., Zhdanova E.A., Serov V.N.
Objective: To assess the clinical and reproductive outcomes in patients with Asherman’s syndrome (AS) using hysteroscopic adhesiolysis (HA) in combination with photodynamic therapy (PDT).
Materials and methods: We analyzed case series of 16 patients aged 25–49 years (the median age – 31.6 years). The diagnosis of chronic endometritis was verified in the whole cohort of patients; 75% of patients experienced infertility. According to AFS classification Asherman’s syndrome stage I was in 43.8% of patients, stage II was in 37.5%, and stage III was in 18.8%. All patients underwent hysteroscopic adheolysis, endometrial biopsy, intracavitary photosensibilization with subsequent endometrial laser therapy (662 nm, ~30–40 J/cm²). Anti-adhesion barriers and hormonal balance support/IUD were used according to indications. Analysis of case series was performed according to the PROCESS guidelines.
Results: Menstrual function recovery was in 100% of patients after the first intervention. Repeat hysteroresectoscopy was performed in one patient due to recurrence of AS. Pregnancy occurred in 42% of patients within 2–9 months after HA in combination with or without PDT. No side effects of PDT were registered.
Conclusion: A combination of HA and PDT along with anti-adhesion barriers and hormonal balance support demonstrated positive dynamics of menstrual function recovery and promising reproductive outcomes in the small cohort of patients. Further randomized control trials as well as long-time observations are necessary to confirm the impacts of treatments on recurrence of AS/fertility.
Authors' contributions: Pasman N.M. – study concept and design, scientific editing of the manuscript; Selyunina N.A. – study design, manuscript editing; Panova S.V., Karpets I.O., Sayapina S.I. – colliection and analysis of published data and the clinical and anamnestic data, manuscript writing; Shifon S.A., Zhdanova E.A. – manuscript editing; Veretelnikova T.V. – submission of clinical and anmnestic data, and photographs; Serov V.N. – final editing of the manuscript.
Conflicts of interest: The authors declare that they have no conflicts of interest.
Funding: The study was carried out without any sponsorship.
Ethical Approval: The study was approved by the local Ethics Committee of V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of Russia.
Patient Consent for Publication: The patients have signed informed consent for participation in the study and publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Pasman N.P., Selyunina N.A., Panova S.V., Karpets I.O., Sayapina S.I.,
Veretelnikova T.V., Shifon S.A., Zhdanova E.A., Serov V.N. Photodynamic therapy as
a contemporary treatment approach to Asherman’s syndrome.
Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2026; (4): 143-148 (in Russian)
https://dx.doi.org/10.18565/aig.2025.379
Keywords
Asherman’s syndrome
cyclic hormone therapy
anti-adhesion barriers
hysteroscopic adhesiolysis
photodynamic therapy
Asherman’s syndrome (AS) is an acquired pathological condition caused by trauma to the endometrium and is characterized by the presence of intrauterine adhesions (IUA) resulting in partial or complete obliteration of the uterine cavity and/or cervical canal. Moreover, AS in patients can be manifested with one of the following signs: infertility, recurrent miscarriage, dysmenorrhea, pelvic pain (not associated with menstrual periods), abnormal placentation, menstrual irregularities (amenorrhea, hypomenorrhea or oligomenorrhea).
The endometrium is composed of two main layers: the deep basal layer and the superficial functional layer. Thickness of the superficial functional layer can vary from thick to thin [1]. The functional layer of the endometrium is shed during the menstrual period in the absence of embryo implantation and with a decrease in estrogen and progesterone levels. The process of shedding is regulated by a cascade of endocrine and paracrine signaling in the endometrium. The basal layer contains the stroma, the basal portion of the glands supporting the vasculature, and various immune cell populations, such as natural killer cells, neutrophils, macrophages, and lymphocytes. It remains unchanged during menstruation and serves as a source for renewal of the functional layer after menstruation [1]. Endometrial integrity can be impaired under the influence of different factors, including surgeries, the use of intrauterine contraceptives (hypoestrogenism), as well as infection (chronic endometritis) [2]. In most cases, the endometrium regenerates without complications. However, in some cases, regeneration is disrupted that leads to the formation of scar tissue.
Recently, it has been proven that previous pregnancy plays a significant role as the key factor that provokes AS [2, 3]. The main criterion for the disease severity is a combination with chronic endometritis, which is diagnosed in 34.9% of patients with the severe grade of the pathology [4, 5]. According to some authors, the pathogenesis of intrauterine adhesions is characterized by endometrial trauma, that involves activation of immune response and cytokine release leading to the development of the inflammatory process that results in changes in the anatomical integrity of the uterus and impaired function [5, 6]. In women with intrauterine adhesions, significant changes are observed in expression of the genes S100A8, VNN2, RGS2, ERAP2, AQP9, MNDA, FSGR3B, which are involved in the processes of fibrosis, apoptosis, immune response and inflammation [7]. The main histological feature of AS is endometrial fibrosis. The stroma is largely replaced by avascular fibrous tissue and spindle-shaped myofibroblasts, and the endometrial glands are replaced by inactive cuboidal epithelium [8]. AS presents a significant challenge in scar-free healing of the endometrium due to impairment of some key mechanisms that ensure scar-free healing and regeneration. These mechanisms include hypoxic injury, imbalanced inflammatory responses, decreased angiogenesis, impaired immune and molecular processes, abnormal differentiation of myofibroblasts, impaired regeneration of stem cell, and abnormal proliferation of the endometrial cells [9, 10]. Therefore, in-depth understanding of the pathophysiology of AS can help clarify defect corrections and possibly contribute to the development of improved strategies for prevention and treatment of AS.
Clinical manifestations of AS include menstrual disorders (amenorrhea, hypomenorrhea, oligomenorrhea), impaired implantation, abnormal placentation (placenta previa, placenta accreta) resulting in infertility, recurrent miscarriages or ectopic pregnancy.
Currently, hysteroscopic adhesiolysis (HA) is recognized as an optimal treatment method for AS. The main advantages of HA are minimal invasiveness and direct visualization of the surgical area. In cases of severe intrauterine adhesions, ultrasound-guided technique for HA is recommended to improve surgical safety and prevent uterine perforation, since in certain cases, laparoscopic assistance can be required [11]. Currently, no consensus has been achieved on comparative effectiveness of therapeutic approaches [12]. Estrogen monotherapy or combined estrogen–progesterone therapy is widely used in the postoperative management of intrauterine adhesions and is considered a key component of therapy aimed at stimulating endometrial proliferation [13]. Despite the widespread use of hormone therapy, currently, there are no comparative studies evaluating the effectiveness of estrogen monotherapy versus combined estrogen–progesterone therapy for AS. Furthermore, there are significant variations in the duration and treatment doses of postoperative estrogen therapy. According to the published data, the length of treatment ranges from not using hormone therapy to three 28-day cycles with daily dosages of estradiol valerate or conjugated estrogens ranging from 2 to 10 mg [14]. There are different methods to prevent the recurrence of adhesions, including balloon catheters, intrauterine devices, and hyaluronic acid-based gels [15–17]. Currently, there is no single solution regarding the optimal period of time during which intrauterine contraceptive can remain in the uterus after insertion, and it varies from 1 to 3 months [18]. Current data do not provide convincing evidence of benefits of using Foley catheter to improve clinical outcomes compared with not using postsurgical antiadhesive barriers after HA [19, 20].
Photodynamic therapy (PDT) is a promising therapeutic approach to treatment of AS. PDT is based on the synergistic interaction of three components: the photosensitizer, 662 nm light irradiation, and reactive oxygen species [21]. The photosensitizer (PS) absorbs the light of the appropriate wavelength and is excited into the triplet state upon irradiation. The PS then returns to the ground state and transfers energy to the oxygen molecules, generating highly reactive singlet oxygen. This initiates a cascade of oxidative reactions leading to selective apoptosis and/or necrosis of target cells with minimal damage to surrounding healthy tissues [22]. PDT can be used for treatment of chronic endometritis in patients with infertility. According to research results, the use of PDT in combination with intracavitary injections demonstrates high treatment effectiveness – rapid restoration of the morphofunctional state of the endometrium, and improved steroid hormone receptor expression both in the glands and the endometrial stroma [23, 24].
Materials and methods
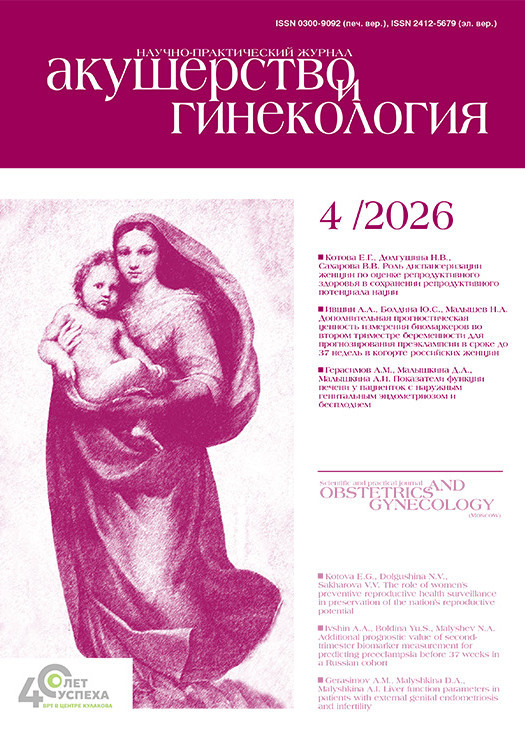
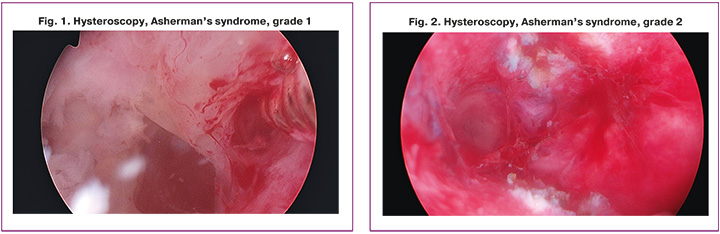
Case series analysis involving 16 patients aged from 25 to 49 years (the mean age 31,6 years) was performed. It should be noted that the majority of participants in the sample were 12/16 (75%) patients with infertility duration from 1 to 10 years, whereas the remaining 4/16 (25%) patients did not plan parenthood or were perimenopausal women. According to American Fertility Society classification based on the extent of cavity involved and menstrual pattern, the patients had mild, moderate and severe Asherman’s syndrome. According to this classification 7/16 (43.75%) patients had AS grade I, 6/16 (37.5%) – grade II, 3/16 (18.75%) – grade III (Fig. 1). Case series was analyzed in compliance with the PROCESS guidelines [25].
Most patients – 10/16 (62,5%) complained of inability to conceive after regular unprotected sexual intercourse. Moreover, 3/16 (18.75%) patients had oligomenorrhea; 1 patient (6.25%) had dysmenorrhea, and 1 (6.25%) had amenorrhea. Three patients needed preconception care in the absence of complaints (18.75%). One patient complained of abdominal pain in the right iliac fossa (6.25%).
All patients (100%) had a burdened medical history of intrauterine surgical interventions.
Hysteroscopy-assisted curettage was previously performed once in 2/16 women (12.5%) once, twice in 5/16 (31.25%), and thrice in 3/16 (18.75%). Two patients with a history of multiple interventions underwent hysteroscopy-assisted uterine and cervical canal curettage 7 and 8 times, respectively. These interventions were performed for polypectomy (50%) or dissection of adhesions.
Traditional curettage for elective abortion was previously performed in 6/16 women (37.5%) – once in 3/16 (18.75%), and twice in 3/16 (18.75%).
Gravidity and parity was the following: 3/16 (18.75%) were pregnant one time, 3/16 (1875%) – two times, 3/16 (1875%) – 4 times and 1/16 (6.25%) – five times. In the studied cohort, 3/16 (18.75%) patients underwent 1 cesarean section with laparotomy using the Pfannenstiel incision technique, 1/16 (6.25%) women had two cesarean deliveries. In addition, each of 2/16 (12.5%) patients had a history of 2 ectopic pregnancies with subsequent tubectomy.
AS occurred after abortion including vacuum aspiration, instrumental curettage in 7/16 (43.75%) patients. One case was in 2/16 (12.5%), 2 cases in 3/16 (18.75%), and 3 cases in 2/16 (12.5%) patients.
The distribution of hypoestrogenism in the sample of patients was the following: premature ovarian failure in 1/16 (6.25%) patient, a history of ovariectomy in 1/16 (6.25%), hyperprolactinemia in 2/16 (12.5%) patients.
All 16 patients (100%) had chronic endometritis according to histological and immunohistochemical examination.
The distribution of the incidence of other gynecological diseases was the following: polycystic ovary syndrome in 5/16 (31.25%) patients, the frequency of concomitant adenomyosis in 8/16 cases (50%), congenital uterine anomalies in 3/16 patients: the saddle shaped uterus in 2/16 (12.5%), and the incomplete intrauterine septum in 1/16 (6.25%).
Extragenital pathology in the sample of patients included the following: diagnosed dyslipidemia in 7/16 women (43.75%), arterial hypertension in 3/16 (18.75%), disorders of carbohydrate metabolism in 4/16 (25%). According to body mass index (BMI), pre-obesity (BMI 25.0–29.9 kg/m2) was in 2/16 (12.5%) patients, obesity Class 1 (BMI 30–34.9 kg/m2) in 1/16 (6.25%), obesity Class 2 BMI 35.0–39.9 kg/m2) in 1/16 (6.25%).
Results
All patients underwent hysteroscopic adhesiolysis, endometrial biopsy and photosensitization of the uterine cavity after preliminary transcervical instillation of radachlorin 0.35%, 1.0 ml dissolved in saline 3 ml with an exposure time of 60 – 90 minutes. The inner walls of the uterine cavity were irradiated with laser light of wavelength 662 nm in continuous, non-contact mode for 11–13 minutes to reach light energy density of 30–40 J/cm2 with radiated power of 0.3–0.4 W using a quartz polymer-based light guide connected to the Latus semiconductor laser device. After surgical intervention, the patients were injected with anti-adhesive solution into the uterine cavity.
After hysteroscopy, 9/16 patients (56.25%) received hormone therapy (dydrogesterone and estradiol) in a cyclic regimen, 3/16 (18.75%) received progestogens (dydrogesterone) in a cyclic regimen, and 4/16 (25%) patients underwent insertion of the levonorgestrel intrauterine device. Menstrual cycle restored after the first hysteroresectoscopy combined with PDT in 16 patients (100%). One patient underwent repeat hysteroresectoscopy due to recurrent adhesions.
After treatment at the clinic, 5/16 patients got pregnant (31.25% of all patients, and 42% of those planning pregnancy). Following the first hysteroresectoscopy combined with PDT, pregnancy occurred in three patients within 2 – 8 months; after repeat hysteroresectoscopy combined with PDT, pregnancy occurred in two patients within 4 – 9 months.
Conclusion
Analysis of pathogenetic factors indicates the key role of repeated intrauterine interventions, unfavorable reproductive history, and endometrial insufficiency against the backdrop of hypoestrogenic state in the occurrence of AS, that necessitates the need for a comprehensive approach to prevention and treatment.
Reproductive outcomes showed promising results, that indicates the potential of combination therapy (hormone therapy and PDT) in fertility restoration.
PDT proved to be a safe treatment method, since there were no cases of complications and side effects in the studied group of patients.
Limitations of the study. Limitations of the study include small sample size, absence of the control group and short-term observation period.
Therefore, there is a need to conduct randomized comparative studies with inclusion of standard protocols for prevention of recurrence (anti-adhesion barrier, cyclic hormone therapy, repeat hysteroscopy) to objectively assess contribution of PDT to improvement of menstrual and reproductive outcomes.
References
- Torres-De La Roche L.A., Campo R., Devassy R., Di Spiezio Sardo A., Hooker A., Koninckx P. et al. Adhesions and anti-adhesion systems highlights. Facts Views Vis. Obgyn. 2019; 11(2): 137-49.
- Филиппов О.С., Павлов К.Д. Результаты анализа частоты и причин кесарева сечения, основанного на классификации Робсона, в акушерских стационарах Федерального медико-биологического агентства России. Российский вестник акушера-гинеколога. 2023; 23(5): 7‑12. [Filippov O.S., Pavlov K.D. Results of the analysis of the frequency and causes of caesarean section based on Robson’s classification in obstetric hospitals of the Federal medical and biological agency of Russia. Russian Bulletin of Obstetrician-Gynecologist. 2023; 23(5): 7 12 (in Russian)]. https://dx.doi.org/10.17116/rosakush2023230517
- Siferih M., Gebre T., Hunduma F., Abebe A., Gebremichael A., Sewunet H. et al. Review of Asherman syndrome and its hysteroscopic treatment outcomes: experience in a low-resource setting. BMC Womens Health. 2024; 24(1): 99. https://dx.doi.org/10.1186/s12905-024-02944-0
- Беспалова А.Г., Попов А.А., Федоров А.А., Тюрина С.С., Коваль А.А. Внутриматочные синехии в репродуктивном возрасте: комплексный подход к решению проблемы. Российский вестник акушера-гинеколога. 2021; 21(2): 62‑7. [Bespalova A.G., Popov A.A., Fedorov A.A., Tyurina S.S., Koval’ A.A. Intrauterine adhesion at reproductive age: an integrated approach to solving the problem. Russian Bulletin of Obstetrician-Gynecologist. 2021; 21(2): 62‑7. (in Russian)]. https://doi.org/10.17116/rosakush20212102162
- Оразов М.Р., Михалева Л.М., Исмаилзаде С.Я., Безуглова Т.В., Лагутина Е.В. Внутриматочные синехии и хронический эндометрит – есть ли причинно-следственная связь? Гинекология. 2022; 24(2): 144-9. [Orazov M.R., Mikhaleva L.M., Ismailzade S.Ya, Bezuglova T.V., Lagutina E.V. Title. Intrauterine synechiae and chronic endometritis – is there a causal relationship? Gynecology. 2022; 24(2): 144-9 (in Russian)]. https://dx.doi.org/10.26442/20795696.2022.2.201417
- Ремнева О.В., Бельницкая О.А., Игитова М.Б., Фадеева Н.И., Гаранин С.А. Синдром Ашермана: от этиологии до профилактики. Забайкальский медицинский вестник. 2024; 2: 122-34. [Remneva O.V., Belnickaya O.A., Igitova M.B., Fadeeva N.I., Garanin S.F. Ascherman syndrome: from etiology to prevention. Transbaikalian Medical Bulletin. 2024; (2): 122-34 (in Russian)]. https://dx.doi.org/10.52485/19986173_2024_2_122
- Хириева П.М., Кузнецова М.В., Быстрицкий А.А., Мартынов С.А., Бурменская О.В., Трофимов Д.Ю., Адамян Л.В. Исследование уровня мРНК генов в ткани эндометрия у женщин репродуктивного возраста с внутриматочными синехиями. Акушерство и гинекология. 2018; 2: 56-64. [Khirieva P.M., Kuznetsova M.V., Bystritsky A.A., Martynov S.A., Burmenskaya O.V., Trofimov D.Yu., Adamyan L.V. Investigation of the gene mRNA level in the endometrial tissue of reproductive-aged women with intrauterine synechiae. Obstetrics and Gynecology. 2018; (2): 56-64(in Russian)]. https://dx.doi.org/10.18565/aig.2018.2
- Dreisler E., Kjer J.J. Asherman’s syndrome: current perspectives on diagnosis and management. Int. J. Womens Health. 2019; 11: 191-8. https://dx.doi.org/10.2147/IJWH.S165474
- Wei C., Pan Y., Zhang Y., Dai Y., Jiang L., Shi L. et al. Overactivated sonic hedgehog signaling aggravates intrauterine adhesion via inhibiting autophagy in endometrial stromal cells. Cell. Death Dis. 2020; 11(9): 755. https://dx.doi.org/10.1038/s41419-020-02956-2
- Liu F., Hu S., Wang S., Cheng K. Cell and biomaterial-based approaches to uterus regeneration. Regen. Biomater. 2019; 6(3): 141-8. https://dx.doi.org/10.1093/rb/rbz021
- Santamaria X., Isaacson K., Simón C. Asherman’s syndrome: it may not be all our fault. Hum. Reprod. 2018; 33(8): 1374-80. https://dx.doi.org/10.1093/humrep/dey232
- Yamamoto N., Takeuchi R., Izuchi D., Yuge N., Miyazaki M., Yasunaga M. et al. Hysteroscopic adhesiolysis for patients with Asherman's syndrome: menstrual and fertility outcomes. Reprod. Med. Biol. 2013; 12(4): 159-166. https://dx.doi.org/10.1007/s12522-013-0149-x
- Guo J., Li T.C., Liu Y., Xia E., Xiao Y., Zhou F. et al. A prospective, randomized, controlled trial comparing two doses of oestrogen therapy after hysteroscopic adhesiolysis to prevent intrauterine adhesion recurrence. Reprod. Biomed. Online. 2017; 35(5): 555-61. https://dx.doi.org/10.1016/j.rbmo.2017.07.011
- Liu L., Huang X., Xia E., Zhang X., Li T.C., Liu Y. A cohort study comparing 4 mg and 10 mg daily doses of postoperative oestradiol therapy to prevent adhesion reformation after hysteroscopic adhesiolysis. Hum. Fertil. (Camb). 2019; 22(3): 191-7. https://dx.doi.org/10.1080/14647273.2018.1444798
- Luo Y., Sun Y., Huang B., Chen J., Xu B., Li H. Effects and safety of hyaluronic acid gel on intrauterine adhesion and fertility after intrauterine surgery: a systematic review and meta-analysis with trial sequential analysis of randomized controlled trials. Am. J. Obstet. Gynecol. 2024; 231(1): 36-50.35. https://dx.doi.org/10.1016/j.ajog.2023.12.039
- Sroussi J., Bourret A., Pourcelot A.G., Thubert T., Lesavre M., Legendre G. et al. Does hyaluronic acid gel reduce intrauterine adhesions after dilation and curettage in women with miscarriage? A Multicentric randomized controlled trial (HYFACO Study). Am. J. Obstet. Gynecol. 2022; 227(4): 597.e1-e8. https://dx.doi.org/10.1016/j.ajog.2022.05.064
- Liu Y.R., Liu B., Yang B.P., Lan Y., Chi Y.G. Efficacy of hyaluronic acid on the prevention of intrauterine adhesion and the improvement of fertility: a meta-analysis of randomized trials. Complement Ther. Clin. Pract. 2022; 47: 101575. https://dx.doi.org/10.1016/j.ctcp.2022.101575
- Salma U., Xue M., Md Sayed A.S., Xu D. Efficacy of intrauterine devices in the treatment of intrauterine adhesions. Biomed. Res. Int. 2014; 2014: 589296. https://dx.doi.org/10.1155/2014/589296
- Lin X., Wei M., Li T.C., Huang Q., Huang D., Zhou F., Zhang S. et al. A comparison of intrauterine balloon, intrauterine contraceptive device and hyaluronic acid gel in the prevention of adhesion reformation following hysteroscopic surgery for Asherman syndrome: a cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013; 170(2): 512-6. https://dx.doi.org/10.1016/j.ejogrb.2013.07.018
- Konci R., Caminsky N., Tulandi T., Dahan M.H. Supplements to conventional treatment after hysteroscopic lysis of intrauterine adhesions: a systematic review. J. Obstet. Gynaecol. Can. 2020; 42(8): 984-1000. https://dx.doi.org/10.1016/j.jogc.2019.09.008
- Никонов С.Д., Пасман Н.М., Безденежных Е.И. Способ лечения хронического эндометрита. Патент № 2692999 C2 Российская Федерация. 2019. 10 с. [Nikonov S.D., Pasman N.M., Bezdenezhnykh E.I. Method of treating chronic endometritis. Patent No. 2692999 C2 Russian Federation. 2019. 10 p. (in Russian)].
- Henderson B.W., Dougherty T.J. How does photodynamic therapy work? Photochem. Photobiol. 1992; 55(1): 145-57. https://dx.doi.org/10.1111/j.1751-1097.1992.tb04222.x
- Серебренникова К.Г., Арутюнян Н.А., Кацалап С.Н., Алехин А.И. Фотодинамическая терапия у пациенток с бесплодием при хроническом эндометрите. Российский вестник акушера-гинеколога. 2020; 20(3): 56‑61. [Serebrennikova K.G., Arutyunyan N.A., Katsalap S.N., Alekhin A.I. Photodynamic therapy in patients with infertility in chronic endometritis. Russian Bulletin of Obstetrician-Gynecologist. 2020; 20(3): 56-61 (in Russian)]. https://dx.doi.org/10.17116/rosakush20202003156
- Безденежных Е.И., Пасман Н.М., Никонов С.Д. Фотодинамическая терапия в лечении хронического эндометрита, ассоциированного с бесплодием. В кн.: Пасман Н.М., Денисов М.Ю., ред. Новые технологии в акушерстве, гинекологии, перинатологии и репродуктивной медицине. Новосибирск: Клиника профессора Пасман; 2017: 65-7. [Bezdenezhnykh E.I., Pasman N.M., Nikonov S.D. Photodynamic therapy in the treatment of chronic endometritis associated with infertility. In: Pasman N.M., Denisov M.Yu., eds. New technologies in obstetrics, gynecology, perinatology, and reproductive medicine. Novosibirsk: Professor Pasman clinic; 2017: 65-7 (in Russian)].
- Agha R.A., Sohrabi C., Mathew G., Franchi T., Kerwan A., O'Neil N. The PROCESS 2020 Guideline: updating consensus preferred reporting of CasESeries in surgery (PROCESS) guidelines. Int. J. Surg. 2020; 84: 231-5. https://dx.doi.org/10.1016/j.ijsu.2020.11.005
Received 22.12.2025
Accepted 13.02.2026
About the Authors
Natalia M. Pasman, Dr. Med. Sci., Professor, Head of the Department of Obstetrics and Gynecology, Institute of Medicine and Medical Technologies, Faculty of Medicine and Psychology, Novosibirsk National Research State University, 630090, Russia, Novosibirsk, Pirogova str., 2, +7(913)916-25-91, https://orcid.org/0000-0002-6095-1954Nadezhda A. Selyunina, obstetrician-gynecologist, Professor Pasman Clinic LLC; Teaching Assistant, Department of Obstetrics and Gynecology, Institute of Medicine and Medical Technologies, Novosibirsk National Research State University, 630090, Russia, Novosibirsk, Pirogova str., 2, Researcher ID Web of Science OAJ-2348-2025,
https://orcid.org/0009-0003-9958-6151
Sofya V. Panova, student at the Department of Obstetrics and Gynecology, Institute of Medicine and Medical Technologies, Faculty of Medicine and Psychology, Novosibirsk National Research State University, 630090, Russia, Novosibirsk, st. Pirogova, 2, https://orcid.org/0009-0005-6321-5652
Irina O. Karpets, student at the Department of Obstetrics and Gynecology, Institute of Medicine and Medical Technologies, Faculty of Medicine and Psychology, Novosibirsk National Research State University, 630090, Russia, Novosibirsk, Pirogova str., 2, https://orcid.org/0009-0008-6925-7388
Sofya I. Sayapina, student of the Department of Obstetrics and Gynecology, Institute of Medicine and Medical Technologies, Faculty of Medicine and Psychology, Novosibirsk National Research State University, 630090, Russia, Novosibirsk, Pirogova, 2, s.sayapina@g.nsu.ru, https://orcid.org/0009-0004-1174-1303
Tatyana V. Veretelnikova, obstetrician-gynecologist of the highest category, Professor Pasman Clinic LLC, Russia, Novosibirsk, https://orcid.org/0009-0007-1022-6985
Sofya A. Shifon, student at the Department of Obstetrics and Gynecology, Institute of Medicine and Medical Technologies, Faculty of Medicine and Psychology, Novosibirsk National Research State University, 630090, Russia, Novosibirsk, Pirogov str., 2, https://orcid.org/0009-0000-6461-5563
Elizaveta A. Zhdanova, student at the Department of Obstetrics and Gynecology, Institute of Medicine and Medical Technologies, Faculty of Medicine and Psychology, Novosibirsk National Research State University, 630090, Russia, Novosibirsk, Pirogova str., 2, https://orcid.org/0009-0001-9259-4840
Vladimir N. Serov, Dr. Med. Sci., Academician of the Russian Academy of Sciences, Professor, Chief Researcher, Academician V.I. Kulakov National Medical Research Center for Obstetrics, Gynecology and Perinatology, Ministry of Health of Russia, 117997, Russia, Moscow, Ak. Oparina str., 4, +7(495)438-72-87,
https://orcid.org/0000-0001-6640-1235
Corresponding author: Sofya I. Sayapina, s.sayapina@g.nsu.ru
Similar Articles

