
The contents of macro- and microelements in blood serum in pregnant and laboring women with weak contractions
Melnik E.V., Voskresensky S.L., Zhurko P.T.
Objective: To define the characteristics of the contents of macro- and microelements in blood serum before labor and in first stage of labor in women with weak contractions.
Materials and methods: The study included 86 women with full-term pregnancy, who were divided into 2 groups after delivery depending on the characteristics of the course of labor: the main group included the patients with weak contractions (n=46), the comparison group included the women, in whom labor and delivery happened without without anomalies labor contractions (n=40). Serum potassium, sodium, ionized calcium, total calcium, magnesium, inorganic phosphorus, and iron levels were analyzed before labor and in the first stage of labor.
Results: The women with weak contractions before labor have higher serum levels of potassium, iron, potassium-to-magnesium ratio and lower sodium-to-potassium ratio versus women with normal physiologic birth. In women with hypotonic uterine contractions in labor, magnesium levels are low and calcium to magnesium ratio and potassium to magnesium ratio is higher versus the comparison group.
Conclusion: In women with weak labor contractions, there are changes of macro- and microelement contents in blood serum. The obtained results may indicate the reasons for inadequate excitability and contractility of the myometrium in these patients.
Authors’ contributions: Melnik E.V. – the concept and design of the study, material collection, statistical data processing, writing the text of the article; Voskresensky S.L. – the concept and design of the study, article editing; Zhurko P.T. – organization and laboratory testing performance.
Conflicts of interest: The authors declare that they have no conflict of interests.
Funding: The study was carried out within the State program of scientific researches of the Republic of Belarus “Translational medicine”, assignment No. 3.47 “To develop a method for prevention of spontaneous abortion and preterm birth in pregnant women with connective tissue dysplasia,” state registration No. 20220318, implementation term 01.01.2022-31.12.2024.
Acknowledgements: The authors of the article express gratitude to Vladimir S. Kamyshnikov, MD, Professor, Head of the Department of Clinical Laboratory Diagnostics of Belarusian Medical Academy of Postgraduate Education, and to Tamara M. Yurage, the Head of the Department of Metabolic Diagnostics of the scientific research laboratory of Belarusian Medical Academy of Postgraduate Education for their consultative assistance.
Ethical Approval: The study was approved by the Ethics Committee of Belarusian Medical Academy of Postgraduate Education (extract from Protocol No 3 of April 15, 2021).
Patient Consent for Publication: The patients have signed informed consent for publication of their data.
Authors' Data Sharing Statement: The data supporting the findings of this study are available on request from the corresponding author after approval from the principal investigator.
For citation: Melnik E.V., Voskresensky S.L., Zhurko P.T. The contents of macro- and microelements in blood serum in pregnant and laboring women with weak contractions. Akusherstvo i Gynecologia/Obstetrics and Gynecology. 2023; (11): 96-103 (in Russian)
https://dx.doi.org/10.18565/aig.2023.181
Keywords
labor
weak labor contractions
potassium
magnesium
calcium
iron ions
To date, there is no common opinion on the causes and mechanisms of weak labor contractions. Obviously, the success of labor process is determined by the structural properties and functional activity of the uterus.
About 51–69% of the volume of the uterine body [1] and 10–15% the cervix [2] is composed of smooth muscle cells; the rest volume consists of the components of connective tissue. Consequently, impaired contractile activity of the uterus can be expected when there are changes in its structure, function of muscle tissue and/or connective tissue.
Macro- and microelements are essential in the construction and functioning of these tissues. So, iron ions are an integral part of myoglobin in myocytes and along with magnesium ions participate in the synthesis of the components of ground substance of connective tissue, and affect the structure of collagen [3–7]. Sodium and potassium ions are important for generation of membrane potential [8]. Calcium and magnesium ions regulate the interaction of actin and myosin in myocytes [8]. Iron participates in oxygen transportation and tissue respiration [3]. Phosphorus is a part of the content of adenosine triphosphoric acid and creatine phosphate that are energy sources for many processes, including muscle contraction [3].
Thus, the deficiency or excess of macro- and microelements, their imbalance may lead to metabolic breakdown of both muscle and connective tissues, and undoubtedly affect the course of labor.
The purpose of the study was to define the characteristics of the contents of macro- and microelements in blood serum before the onset of labor and in the first stage of labor in women with weak contractions.
Materials and methods
The study included 86 women with full-term pregnancy, who were admitted to the Clinical Maternity House of the Minsk Region before delivery. After delivery, depending on the characteristics of the course of labor the women were divided into 2 groups: the main group (n=46) included the patients with primary (n=31) and secondary (n=15) uterine inertia. The comparison group included the women (n=40), in whom the course of labor and delivery was normal.
Inclusion criteria in the study were women with full-term pregnancy (37 weeks–41 weeks and 6 days of gestation), singleton pregnancy, cephalic presentation of the fetus, spontaneous onset of labor, weakness of labor contractions (the main group), absence of labor abnormalities (the comparison group), informed consent to participate in the study.
Exclusion criteria were the women at > 37 or ≥ 42 week’s gestation, multiple pregnancy, contraindications for vaginal delivery, pre-induction and labor induction, acute genital and extragenital disorders.
The study was carried out in accordance with The Declaration of Helsinki of the World Medical Association, the Health Law of the Republic of Belarus. The extract from the protocol No. 3 of April 15, 2021 of the minutes of the Ethics Committee, the State educational institution "Belarusian Medical Academy of Postgraduate Education" of the Ministry of Health of the Republic of Belarus. All participants in the study signed informed consent.
The diagnosis of “hypotonic labor” and management strategy were defined in accordance with the Clinical protocol “Medical observation and provision of medical care for women in obstetrics and gynecology” (the Decree No. 17 of February 19, 2018, of the Ministry of Health of the Republic of Belarus). The diagnosis of “primary inertia” was made, when cervical dilation rate was less than 1 cm/hour for 2 hours with > 6 cm of cervical dilation. The diagnosis of “secondary inertia” was made when similar dilation rate for 2 hours with > 6 cm of cervical dilation.
Amniotomy was performed in women with primary inertia (in case of intact amniotic sac), and in the absence of dynamics of cervical dilation for 2 hours. Uterotonics were administered to facilitate labor contractions: dinoprostone was intravenously administered, when the cervix was 4 cm dilated; and oxytocin was intravenously administered, when the cervix was more than 4 cm dilated. Caesarean section was performed in the absence of treatment effect within 6 hours from the time of diagnosis and/or in case of acute fetal hypoxia. In women with secondary inertia, labor stimulation with oxytocin was performed for no longer than 3–4 hours. In the absence of the effect of labor stimulation, surgical delivery was performed.
The primary outcome measure was the content of macro- and microelements in blood serum in women before the onset of labor and in the first stage of labor. The secondary outcome measures included the anthropometric data of the newborns, assessment of the physical condition of neonates by Apgar test at 1 and 5 minutes, and the type of delivery.
Venous blood samples were collected and stored in Greiner Bio-One 6 ml Vacuette tubes with serum clot activator (Greiner Bio-One, Austria). Given by the fact that serum iron level can be deviated depending of the time of sampling, blood samples were collected in the morning on an empty stomach. After material collection, the tubes were centrifuged at 3500 rpm for 10 minutes. The resulting serum was used as the material for laboratory tests. Venous blood samples were collected for tests 1–8 days before the onset of labor (time 1 for material collection), as well as in the first stage of labor when the cervix was 5–6 cm dilated, before stimulation of uterine contractions with uterotonics (time 2 for material collection).
The levels of potassium K+, sodium (Na+), ionized calcium (Ca2+) were measured using the EasyLyte electrolyte analyzer (EasyLyte Calcium Na/K/Ca/pH, Medica Corp., USA). The levels of magnesium (Mg2+), total calcium (Са), inorganic phosphorus (P), iron (Fe) were measured using automatic biochemistry analyzer BA 400 (BioSystems S.A., Spain). The concentrations of macroelemends were measured in mmol/L, and macroelements in μmol/L.
Reference values for K+ were 3.5–5.1 mmol/L, Na+ – 136–145 mmol/L, Ca2+ – 1.16–1.32 mmol/L, Mg2+ – 0.70–1.0 mmol/L, Са – 2.15–2.58 mmol/L, P – 0.81–1.45 mmol/L, Fe – 9.0–30.4 μmol/L.
The following ratios were calculated: the sodium (Na) to potassium (K) ratio as the quotient calculated by dividing Na+ concentration by the K+ concentration in blood serum; the calcium to magnesium ratio (Са2+/Mg2+ ratio) as the quotient calculated by dividing Са2+ concentration to Mg2+ concentration in blood serum; the potassium to magnesium ratio (K+/Mg2+ ratio) as the quotient calculated by dividing K+ concentration to Mg2+ concentration in blood serum.
Statistical analysis
Statistical analysis of the obtained results was performed using software program Statistica 8.0. Nonparametric statistics were used, since the distribution of most indicators obeyed nonparametric approach, that was confirmed by the Kholmogorov–Smirnov and Shapro–Wilk tests. The quantitative parameters were presented as Me (Q1; Q3), where Ме is a median, (Q1; Q3) – interquartile interval (25‰ and 75‰). The qualitative parameters are shown as the percentage (%) and absolute values (abs.) with indication of the numerator and denominator of the calculated percentage. The quantitative data of two independent groups were compared using Mann–Whitney U-test. The quantitative data of two dependent groups were compared using the Wilcoxon test. The qualitative parameters were compared using the Fisher’s exact test. The differences were considered to be statistically significant at p<0.05.
Results and discussion
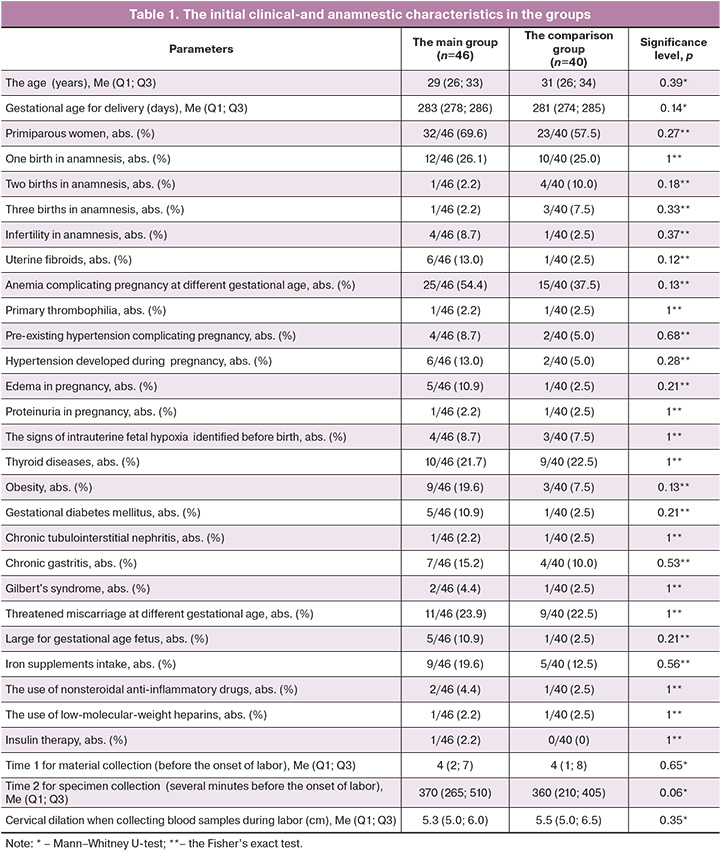
The groups in the study were comparable with regard to the initial clinical and anamnestic characteristics (Table 1). Apart from the parameters, such as the age of patients, the gestational age for delivery, the features of somatic and obstetric and gynecological anamnesis, the course of pregnancy, the temporary parameters of collected material were analyzed, as well as the frequency of using medications within 7–10 days before performing laboratory test, that could influence the level of macro- and microelements in the blood.
Assessment of newborns’ condition at birth was performed. The Apgar score at 1 minute of life was 8 (8; 8) and 8 (8; 8) in the main group and in the comparison group, respectively (р=005). At the same time, low Apgar score of 3–6 was in 4 newborns in the main group, and there was no low Apgar score in the comparison group: 4/46 (8,7%) and 0/40 (0%) (p=0.12).
Apgar score of 7–9 at 5 minutes was in all newborns. However, there was statistically significant difference in Apgar scores between the groups: the Apgar score in the main group was lower versus the comparison group – 8 (8; 9) and 9 (9; 9), (p<0.001).
The analysis of the anthropometric data of newborns did not show statistically significant differences between the main and the comparison group in baby weight – 3405 (3200; 3730) g, respectively (p=0.32) and baby length at birth – 53 (52; 54) cm and 53 (51; 54) cm, respectively (p=0.74). The number of babies that were large for gestational age was 7/46 (15.2%) and 2/40 (5.0%) in the main group and in the comparison group, respectively (p=0.17).
The analysis of the type of delivery showed that emergency cesarean section was performed significantly more often in the main group versus the comparison group – in 16/46 (34.8%) women and 1/40 (2.5%) woman, respectively (p<0.001). The indications for cesarean section in the main group were acute fetal hypoxia (change in the fetal heart rate according to cardiotocography records and/or meconium staining of amniotic fluid) in 7/16 (43,8%) cases; failed induction of labor in 9/16 (56.2%) cases. In the comparison group, emergency cesarean section was performed due to clinical narrow pelvis.
The concentration of macro- and microelements in blood serum in women before the onset of labor is shown in Table 2.
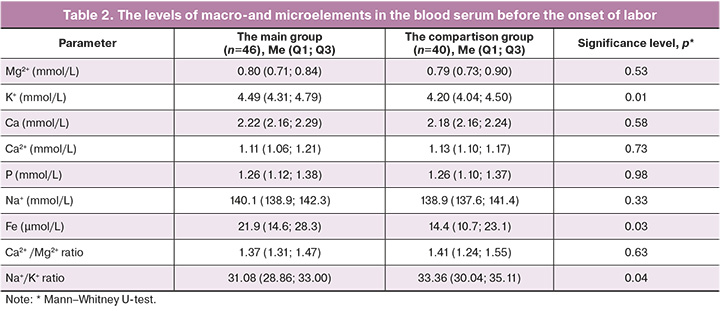
The analysis of the concentration of macro-and microelements in blood serum before the onset of labor, that the reference values were higher in women in the main group versus the comparison group, but did not exceed the reference values; the levels of K+ were 4.49 (4.31; 4.79) mmol/L and 4.20 (4.04; 450) mmol/L, respectively; as well as the levels of Fe were 21.9 (14.6; 28.3) μmol/L and 14.4 (10.7; 23.1) μmol/L, respectively. The Na+/K+ ratio characterizing the processes of excitation of cell membranes was significantly lower in the main group versus the comparison group due to increased level of K+ – 31.08 (28.86; 33.00) and 33.36 (30.04; 35.11), respectively.
The intracellular and extracellular balance of K+ creates the resting potential on cell membranes and ensures muscle and nerve fibers excitability. With excessive potassium channels activity, high concentrations of K+ leave the cell and are found in the extracellular space, that causes hyperpolarization of the membrane and reduced excitability. According to the results of some studies, activation of potassium channels leads to suppression of the coordinated myometrium contractile activity, which is necessary for labor contractions [8, 9]. It was reported that normally potassium channels activity reduces at late terms of pregnancy facilitating increased myometrial contractility and labor [9].
Moreover, K+ influences the synthesis of connective tissue by fibroblasts due to participation in the effects of calcium (Ca2+)-sensing receptor (CaSR) and renal tubular Са2+ reabsorption [10].
The level of K+ in blood serum may increase with acidosis, dehydration, protein and glycogen breakdown [3].
Higher serum potassium levels in pregnant women in the main group may indicate pronounced refractoriness of myometrial tissue before the onset of labor, meaning reduced uterine excitability to stimulation, as well as may reflect structural and functional disorders of connective tissue.
Iron ions are the components of myoglobin in myocytes, mitochondrial redox enzymes; therefore, they influence myometrial contractility [3]. In addition, Fe is cofactor of enzymes which are involved in formation of the triple helix of collagen, as well as in the synthesis of proteoglycans – the components of the ground substance of connective tissue [4].
Serum iron level decreases with systemic inflammation [3, 11]. This occurs due higher levels of pro-inflammatory cytokines: interleukin 1 (IL-1), IL-6 and IL-8, causing an increase in protein hepcidin production, which in turn stimulates iron deposition in macrophages, inhibits iron absorption and mobilization from the depot [12]. Changes before the onset of labor are due to the reactions that are local and systemic inflammatory-type responses, in which pro-inflammatory cytokines IL-1, IL-6, IL-8 are involved. Due to inflammatory-like processes before the onset of labor, the changes occur in the connective tissue framework of the cervix, leading to cervical ripening [13], increased prostaglandin production causes uterine contractile activity [14]. When these processes are insufficient or inadequate, both delayed onset of labor and abnormal labor can be expected.
Higher iron levels in blood serum in women in the main group may indicate a lower severity of inflammatory-like processes before the onset of labor.
The concentration of macro-and microelements in blood serum in the first stage of labor in women in the study is shown is Table 3.
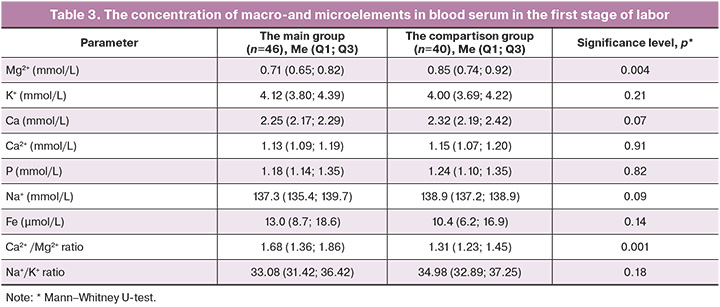
The analysis of concentration of macro- and microelements in the groups under study at the onset of labor showed, that statistically significant differences were in the values of Mg2+ and Са2+/Mg2+ ratio.
Thus, the level of Mg2+ was lower in the main group versus the comparison group: 0.71 (0.65; 0.82) mmol/L and 0.85 (0.74; 0.92) mmol/L, respectively, and Са2+/Mg2+ ratio characterizing the process of myocyte contraction, was higher: 1.68 (1.36; 1.86) and 1.31 (1.23; 1.45), respectively. At the same time, there was no significant difference in the level of Ca2+ in the groups.
There are different opinions regarding the optimum level of Mg2+ in the blood. The reference values vary depending on the author: 0.65–1.10 mmol/L [3], 0.75–0.95 mmol/L [15, 16], 0.70–1.0 mmol/L [17]. However, most recent studies consider the level of Mg2+ in blood serum equal to 0.80 mmol/L as a threshold below which the risk of developing various pathologies increases [18, 19]. The concentration of Mg2+ in the blood does not definitely reflect its concentration in tissue and most commonly is significantly lower. There is an opinion, that the level of Mg2+ lower than 0.80 mmol/L conforms the presence of tissue magnesium deficiency [19]. Most sensitive indicator for Mg2+ deficiency may be Mg2+/Ca2+ ratio in blood serum [16].
Mg2+ has antagonistic properties to Ca2+ and plays a leading role in myocyte relaxation. In clinical practice, magnesium preparations are used to prevent convulsive syndrome and for tocolysis. Based on this, Mg2+ deficiency will lead to increase in myometrial contractility, therefore, to miscarriage, preterm birth, and will not cause pathology – weak labor contractions due to reduction of uterine contractile activity.
Low levels of Mg2+ in blood serum and high values of Са2+/Mg2+ratio in puerperant women in the main group, in contrast with no difference in the levels of Са2+ in the groups under study may indicate participation of Mg2+ ions in the pathogenesis of labor activity, but not due to antagonism to Са2+.
Thus, Mg2+ regulates the activity of ion channels for Na+, K+, participates in production of adenosine triphosphate [6, 15]. Mg2+ deficiency Mg2+ deficiency disrupts sodium-potassium adenosine triphosphatase activity leading to reduction of K+ uptake by cells and increased concentration in the extracellular space [20], that was noted in our study in women in the main group before the onset of labor. Ion imbalance reduces the excitability of myometrial muscle cells.
Moreover, Mg2+ ions are an integral part of enzymes that synthesize and degrade hyaluronic acid, an element of the extracellular matrix of connective tissue [5]. Also, Mg2+ inhibits enzyme activity that provide collagen and elastin cross-linking [7]. Mg2+ deficiency is accompanied by connective tissue disorders, vascular dysfunction [6, 21]. Consequently, with Mg2+ deficiency, there is a likelihood for impaired uterine hemodynamics, which plays an important role in the process of labor according to the discrete wave mechanism of labor [22].
In addition, hypomagnesemia significantly correlates with the imbalance between the sympathetic and parasympathetic systems, impaired catecholamine metabolism, development of chronic endothelial inflammation, and changes in metabolism of neurotransmitters in the central nervous system [6, 16, 18, 21]. These processes can also be pathogenetic mechanisms of weakness of labor contractions.
Therefore, the data obtained by us indicate the complexity and ambiguity of the theory of etiopathogenesis of weak labor contractions. At the same time, lower levels of Mg2+ in blood serum and higher Са2+/Mg2+ ratio in women of the main group may indicate the presence of Mg2+ deficiency in tissues, which is accompanied by a wide range of biological effects that can negatively affect labor.
Given the fact that before the onset of labor and in the first stage of labor, statistically significant differences were found between the levels of K+ and Mg2+, that play an important role in excitation and contraction of myometrial myocytes, it was decided to calculate the K+/Mg2+ ratio in the groups under study. K+/Mg2+ ratio in the groups before the onset of labor and in the first stage of labor is shown in the Figure.
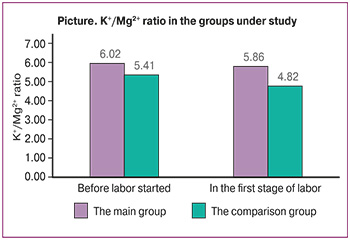
K+/Mg2+ ratio was significantly higher in the main group versus the comparison group, both before the onset of labor 6.02 (5.56; 6.39) and 5.41 (4.72; 5.63), respectively (р=0.01), and in the first stage of labor: 5.86 (4.89; 6.44) and 4.82 (4.42; 5.58), respectively (р=0.01). The detected changes may indicate impaired excitation and contraction in myometrium in women with poor uterine contraction not only during labor, but also before the onset of labor.
With purpose of investigation of the dynamics of macro- and microelements in blood serum from pregnancy to childbirth, the above indicators were compared before the onset of labor and in the first stage of labor. Statistically significant changes were observed for К+, Mg2+, Fe levels in blood serum. At the same time, К+ level reduced both in the main group (p=0.02) and in the comparison group (p=0.01); also, Fe level reduced both in the main group (p=0.003), and in the comparison group (p=0.03); but Mg2+ level significantly reduced only in the main group (p=0.03), while there were no statistically significant changes in level of Mg2+ in the comparison group (p=0.34).
Decreased К+ levels in dynamics may reflect a reduction in potassium channel activity prior to labor and delivery [9], as well as may be associated with increased production of glucocorticoids, aldosterone, insulin, with changes in acid-base status [3], that requires further research. Decreased Fe level may indicate increased activity of inflammatory-like processes in dynamics leading to the start. The identified features of changes in Mg2+ level may indicate its deficiency in tissue, that was manifested by decreased Mg2+ level in blood serum with increased Mg2+ consumption with the onset of labor.
From pregnancy to labor and delivery, there were no statistically significant changes in the levels of macroelements between the main group and the comparison group – Са (p=0.94 and p=0.07, respectively), Ca2+ (p=0.33 and p=0.59, respectively), P (p=0.87 and p=0.75, respectively), Na+ (p=0.07 and p=0.23, respectively).
Conclusion
In women with weak labor contractions, there were changes of macro- and microelement concentration in blood serum. Before the onset of labor, higher K+, Fe levels and K+/Mg2+ ratio, and lower Na+/K+ ratio was observed compared to the women with normal labor. The women with uterine hypoactivity in labor have low Mg2+ level and higher Са2+/Mg2+ ratio and K+/Mg2+ ratio versus the comparison group.
The obtained results may indicate the reasons for inadequate excitability and contractility of the myometrium in women with weak uterine contractions.
Further research is necessary to investigate the possibility of developing prognostic criteria for weakness of labor contractions based on macro- and microelements concentration in the blood.
References
- Павлович Е.Р., Ботчей В.М. Морфология мышечного компонента миометрия первородящих женщин с физиологической родовой деятельностью. Вестник Российского университета дружбы народов. Серия: Медицина. 2016; 3: 46-52. [Pavlovich E.R., Botchey V.M. The morphology of a muscular component of myometrium of primipara women with physiological contractile activity. RUDN Journal of Medicine. 2016; 3: 46-52. (in Russian)].
- Кириленко В.П., Небышинец Л.М. Биохимические преобразования соединительной ткани шейки матки как фактор инициации прерывания беременности. Медицинские новости. 2020; 3: 13-20. [Kirilenko V.P., Nebyshinets L.M. Biochemical transformations of the connective tissue of the cervix as a factor оf initiation of termination of pregnancy. Medical news. 2020; 3: 13-20. (in Russian)].
- Камышников В.С., Денежкина Н.В. Лабораторная диагностика в акушерстве и гинекологии. МЕДпресс-информ; 2021. 480с. [Kamyshnikov V.S., Denezhkina N.V. Laboratory diagnostics in obstetrics and gynecology. MEDpress-inform; 2021. 480p. (in Russian)].
- Керимкулова Н.В., Торшин И.Ю., Громова О.А. Cеров В.Н., Никифорова Н.В. Систематический анализ молекулярно-физиологических эффектов синергидного воздействия железа, марганца и меди на соединительную ткань. Гинекология. 2012; 6: 51-60. [Kerimkulova N.V., Torshin I.U., Gromova O.A., Serov V.N., Nikiforova N.V. Systematic analysis of molecular and physiological synergic effects of iron, manganese and copper on connective tissue. Gynecology. 2012; 6: 51-60. (in Russian)].
- Mio K., Carrette O., Maibach H.I., Stern R. Evidence that the serum inhibitor of hyaluronidase may be a member of the inter-alpha-inhibitor family. J. Biol. Chem. 2000; 275(42): 32413-21. https://dx.doi.org/10.1074/jbc.M005428200.
- Громова О.А., Торшин И.Ю., Тапильская Н.И. Протеомный анализ магний-зависимых белков в системе «мать-плод-ребенок». Фармакокинетика и фармакодинамика. 2017; (1):27-39. [Gromova O.A., Torshin I.Yu., Tapilskaya N.I. Proteomic analysis of magnesium-dependent proteins and children's health. Pharmacokinetics and pharmacodynamics. 2017; (1):27-39. (in Russian)].
- Ahvazi B., Boeshans K.M., Rastinejad F. The emerging structural understanding of transglutaminase 3. J. Struct. Biol. 2004; 147(2): 200-7. https://dx.doi.org/10.1016/j.jsb.2004.03.009.
- Wray S., Arrowsmith S. Uterine excitability and ion channels and their changes with gestation and hormonal environment. Annu. Rev. Physiol. 2021; 83: 331-57. https://doi.org/10.1146/annurev-physiol-032420-035509.
- Brainar A.M., Korovkina V.P., England S.K. Potassium channels and uterine function. Semin. Cell Dev. Biol. 2007; 18(3): 332-9. https://dx.doi.org /10.1016/j.semcdb.2007.05.008.
- Huang C., Miller R.T. The calcium-sensing receptor and its interacting proteins. J. Cell. Mol. Med. 2007; 11(5): 923-34. https://dx.doi.org/10.1111/j.1582-4934.2007.00114.x
- Будкова А.И., Лапин С.В., Павлович Д., Богданов А.Н., Щербак С.Г. Диагностика дефицита железа при анемии хронического воспаления. Лабораторная служба. 2022; 11(1): 16-21. [Budkova A.I., Lapin S.V., Pavlovich D., Bogdanov A.N., Shherbak S.G. Diagnosis of iron deficiency in anemia of chronic inflammation. Laboratory service. 2022; 11(1): 16-21. (in Russian)]. https://dx.doi.org/10.17116/labs20221101116.
- Сарсания С.И., Тихомиров А.Л., Ночевкин Е.В., Тускаев К.С. Нюансы диагностики и лечения железодефицитной анемии. Трудный пациент. 2012; 10(2): 23-34. [Sarsaniya S.I., Tihomirov A.L., Nochevkin E.V., Tuskaev K.S. Nuances of diagnosis and treatment of asiderotic anemia. Difficult patient. 2012; 10(2): 23-34. (in Russian)].
- Ludmir J., Sehdev H.M. Anatomy and physiology of the uterine cervix. Clin. Obstet. Gynecol. 2000; 43(3): 433-9. https://dx.doi.org/10.1097/00003081-200009000-00003.
- Schäfer W.R., Zahradnik H.P. (Patho-)Physiologische Grundlagen des Geburtsbeginns. Gynäkologe. 2003; 37: 305-13. https://dx.doi.org/10.1007/s00129-004-1510-2.
- National Institutes of Health. Magnesium. Fact sheet for health professionals. June 2, 2022. https://ods.od.nih.gov/factsheets/Mg2+-HealthProfessional/
- Razzaque M.S. Magnesium: Are we consuming enough? Nutrients. 2018; 10(12):1863. https://dx.doi.org/10.3390/nu10121863.
- Workinger J.L., Doyle R.P., Bortz J. Challenges in the diagnosis of magnesium status. Nutrients. 2018; 10(9) :1202. https://dx.doi.org/10.3390/nu10091202.
- Громова О.А., Торшин И.Ю., Рудаков К.В., Грустливая У.Е., Калачева А.Г., Юдина Н.В., Егорова Е.Ю., Лиманова О.А, Федотова Л.Э, Грачева О.Н., Никифорова Н.В., Сатарина Т.Е., Гоголева И.В., Гришина Т.Р., Курамшина Д.Б., Новикова Л.Б., Лисицына Е.Ю., Керимкулова Н.В., Владимирова И.С. Чекмарева М.Н., Лялякина Е.В., Шалаева Л.А., Талепоровская С.Ю., Силинг Т.Б., Семенов В.А., Семенова О.В., Назарова Н.А., Галустян А.Н., Сардарян И.С. Недостаточность магния – достоверный фактор риска проявлений коморбидных состояний: результаты крупномасштабного скрининга магниевого статуса в регионах России. Фарматека. 2013; 6: 116-29. [Gromova O.A., Torshin I.Ju., Rudakov K.V., Grustlivaja U.E., Kalacheva A.G., Judina N.V. et al. Deficiency of magnesium - a significant risk factor for the manifestations of comorbid conditions: results of a large-scale screening of magnesium status in the regions of Russia. Farmateka. 2013; 6: 116-29 (in Russian)].
- Costello R.B. Nielsen F. Interpreting magnesium status to enhance clinical care: key indicators. Curr. Opin. Nutr. Metab. Care. 2017; 20: 504-11. https://dx.doi.org/10.1097/MCO.0000000000000410.
- Василевский И.В. Новая форма адъювантной терапии в клинической медицине. Международные обзоры: клиническая практика и здоровье. 2018; 1 (29): 70-8. [Vasilevski I.V. New form of advanced therapy in clinical medicine. International Reviews: Clinical Practice and Health. 2018; 1(29): 70-8 (in Russian)].
- Погожева А.В., Коденцова В.М. О рекомендуемом потреблении и обеспеченности населения калием и магнием. Русский медицинский журнал. 2020; 3: 8-12. [Pogozheva A.V., Kodentsova V.M. About recommended consumption and provision of population with potassium and magnesium. Russian Medical Journal. 2020; 3: 8-12. (in Russian)].
- Воскресенский С.Л. Биомеханизм родов: дискретно-волновая теория. Минск: ПолиБиг; 1996. 186 с. [Voskresensky S.L. Biomechanism of childbirth: discrete-wave theory. Minsk: PolyBig; 1996. 186 p. (in Russian)].
Received 31.07.2023
Accepted 24.10.2023
About the Authors
Elena V. Melnik, PhD, Senior Lecturer at the Department of Obstetrics and Gynecolog, Belarusian Medical Academy of Post-Graduate Education, +375(29)755-31-37, ew.melnik@mail.ru, https://orcid.org/0009-0004-5593-3868, 220013, Republic of Belarus, Minsk, P. Brovki str., 3-3.Sergey L. Voskresensky, Dr. Med. Sci., Professor at the Department of Obstetrics and Gynecology, Belarusian Medical Academy of Post-Graduate Education,
+375(29)706-80-09, slv5451@yandex.ru, 220013, Republic of Belarus, Minsk, st. P. Brovki str., 3-3.
Polina T. Zhurko, Researcher, Department of Metabolic Diagnostics, Research Laboratory, Belarusian Medical Academy of Post-Graduate Education, +375(44)792-48-14, pavlinats@mail.ru, 220013, Republic of Belarus, Minsk, P. Brovki str., 3-3.
Corresponding author: Elena V. Melnik, ew.melnik@mail.ru
Similar Articles

