Узкий таз при родоразрешении per vias naturales является основным фактором риска разрывов мягких родовых путей, существенно повышает перинатальную заболеваемость и смертность. Ведение родов при анатомическом сужении таза требует от акушеров-гинекологов теоретических знаний и практических навыков [1, 2].
В настоящее время преобладают «стертые» формы узкого таза, что значительно усложняет своевременное установление диагноза. Наружная пельвиметрия не всегда отражает реальные размеры, оптимальное определение которых возможно с использованием лучевых методов диагностики (магнитно-резонансная (МР) пельвиметрия, рентгенопельвиметрия).
Недооценка истинных размеров таза и пропагандируемая активно-выжидательная тактика нередко завершаются затягиванием принятия решения о выполнении кесарева сечения. Правильная и своевременная интерпретация симптомов клинического несоответствия должна проводиться, не дожидаясь симптомов угрожающего разрыва матки.
Анатомическое сужение таза увеличивает вероятность оперативного родоразрешения в 2,8 раза, хотя оно не является обязательным в 100% наблюдений [3].
При оценке таза с функциональной точки зрения во внимание принимаются: предполагаемая масса плода, характер родовой деятельности, соответствие механизма родов типу сужения таза, причем последнему фактору придается решающее значение. Определенный механизм родов запускается при наличии препятствия продвижению головки. И способ, которым головка будет это препятствие преодолевать, свойственен только конкретной форме таза и подтверждает ее [4].
Отклонение от типичного механизма родов в затылочном предлежании при нормальных параметрах наружной пельвиметрии должно насторожить врача. Данные анамнеза, информация о течении и исходах предыдущих родов, здоровье и развитии ребенка дополнительно могут усилить подозрение о наличии анатомически узкого таза, для которого характерно также высокое стояние головки, преждевременный разрыв плодных оболочек
Сопряженность механизма родов с особенностями сужения таза, отсутствие страдания плода позволяют прогнозировать благоприятный исход вагинальных родов.
Для оценки родовой деятельности, характера вставления головки и динамики ее продвижения по родовому каналу в качестве «золотого стандарта» используется влагалищное исследование. Наряду с ним может быть применен и визуальный ультразвуковой метод. Эхография представляется безопасным и точным инструментом для оценки взаимоотношения предлежащей части плода с родовым каналом. Каждому положению головки соответствуют определенные ориентиры костного таза матери, что объективизирует как течение родов, так и диагноз слабости родовой деятельности или клинического несоответствия [5–7].
Ультразвуковое исследование (УЗИ) в родах повышает эффективность диагностики аномалий родового акта и помогает выработать оптимальную врачебную тактику, что подтверждает приводимое ниже собственное клиническое наблюдение.
Клиническое наблюдение
Пациентка Ц., 27 лет, в 10.00 госпитализирована с жалобами на излитие околоплодных вод.
Настоящая беременность вторая; первая закончилась в 2020 г. своевременными родами живой девочкой 3040 г, 50 см. Ребенок родился в легкой асфиксии, в дальнейшем диагностирована внутриутробная пневмония.
Антропометрические данные пациентки: рост 164 см, вес 79 кг, размеры таза: d. spinarum 25 см, d. cristarum 27 см, d. trochanterica 30 см, c. externa 20 см.
Влагалищное исследование: шейка матки расположена в центре малого таза, длиной 0,5 см, цервикальный канал проходим для 2 пальцев. Плодного пузыря нет, предлежит головка плода, прижата ко входу в малый таз. Характер вставления головки определить не удалось.
Диагноз при поступлении: Беременность 40 недель. Головное предлежание. Преждевременный разрыв плодных оболочек.
Проведена эхография на портативном аппарате LOGIQE с использованием конвексного датчика 5 МГц в положении пациентки лежа на спине. Датчик в защитной упаковке устанавливался на промежность ниже уровня симфиза в сагиттальной и поперечной плоскостях, изображение фиксировалось, по принятой методике выполнялись измерения:
- угла ротации с целью оценки поворота и вращения головки плода;
- угла прогрессии для оценки расположения головки плода относительно плоскостей малого таза.
Частота УЗИ составляла 1 раз в час.
В 10:15 при трансабдоминальном УЗИ определен задний вид затылочного предлежания:
- лицевая часть черепа обращена кпереди;
- определяется профиль плода;
- визуализируется единственная орбита – передняя, отмечается вертикальное смещение глазниц.
С учетом обнаружения только правой орбиты в заднем виде затылочного предлежания, диагностировано асинклитическое вставление головки.
Трансперинеальное исследование: при поперечном сканировании определялась срединная линия, совпадающая со стреловидным швом головки плода, отклонена вправо, структуры головного мозга не визуализировались, что характерно для высокого расположения головки.
В 12:00 при трансперинеальном продольном сканировании: угол прогрессии 106°, уровень -1,5, -1, что соответствует плоскости входа в малый таз; при трансперинеальном поперечном сканировании: срединная линия совпадает с переднезадней осью таза роженицы – стреловидный шов установился в прямом размере входа в малый таз, визуализируются хориоидные сплетения, которые расходятся книзу – задний вид затылочного предлежания.
Принимая во внимание исход первых родов, преждевременный разрыв плодных оболочек в настоящих родах, механизм вставления головки во входе в малый таз, заподозрено анатомическое сужение таза – стертая форма поперечносуженного таза и высокое прямое вставление головки. Роды решено вести выжидательно под контролем УЗИ.
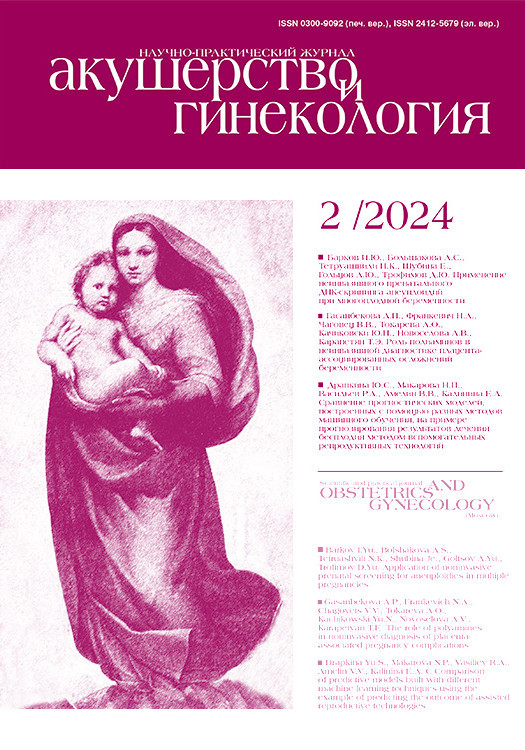
В 13:20 показателем продвижения головки стало увеличение угла прогрессии со 106° до 125° – голова на уровне +0,5, +1, или в плоскости широкой части полости малого таза, появилась родовая опухоль (рис. 1).
При трансперинеальном поперечном сканировании расположение срединной линии все также совпадало с переднезадней осью таза – стреловидный шов оставался в прямом размере.
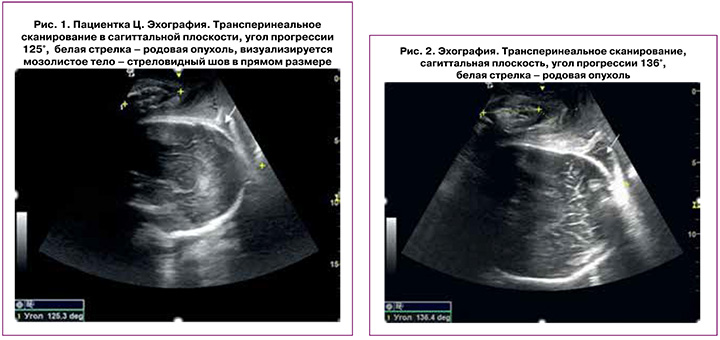
В 14:20 при влагалищном исследовании диагностировано полное открытие шейки матки. При трансперинеальном сканировании угол прогрессии 136°, положение стреловидного шва не изменилось (т.к. видно мозолистое тело) (рис. 2).
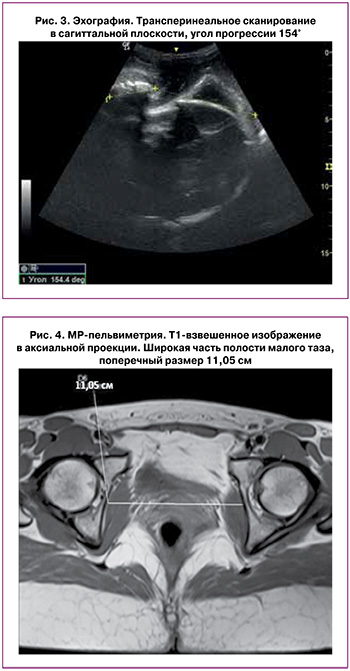
В 15:30 при трансперинеальном сканировании угол прогрессии 154°, что соответствует нахождению головки на уровне +3, плоскость выхода малого таза (рис. 3). При трансперинеальном сканировании в поперечной плоскости отмечено отклонение срединной линии от переднезадней оси таза вправо.
В 16:40 стреловидный шов установился в левом косом размере, началось вращение головки против часовой стрелки. В 17:15 в переднем виде затылочного предлежания произошли роды живым доношенным мальчиком 3240 г, 52 см, оценка по Апгар 8–9 баллов. Головка совершила поворот на 180°. Длительность второго периода 2 ч 55 минут.
В послеродовом периоде проведена МР-пельвиметрия, при которой диагностирован поперечносуженный таз I степени с увеличением прямых размеров плоскости входа и широкой части полости малого таза: прямой размер входа 12,3 см, поперечный размер входа 12,28 см, прямой размер широкой части 12,9 см, поперечный размер широкой части 11,05 см, прямой размер узкой части 11,2 см, межостное расстояние 11,0 см (рис. 4).
Обсуждение
Задний вид затылочного предлежания несет повышенный риск затрудненного течения I и II периодов родов. Больший размер проходящей по родовым путям окружности головки снижает вероятность самопроизвольных родов почти в 4 раза у первородящих и вдвое – у повторнородящих [1].
При затылочном предлежании плода и клиническом соответствии головка совершает поворот, переходя в узкую часть полости малого таза. Установлением стреловидного шва в прямом размере выхода таза заканчивается поворот головки, без которого самопроизвольные роды затруднены или вообще невозможны.
В описанном наблюдении изначально был диагностирован задний вид затылочного предлежания. С началом родовой деятельности стреловидный шов при эхографии определялся в прямом размере плоскости входа в малый таз, что типично для поперечносуженного таза.
Роды при уменьшенных поперечных размерах могут закончиться через естественные родовые пути только в переднем виде. При заднем виде появляются признаки клинического несоответствия.
Формирование асинклитизма при вставлении головки является наиболее характерным для механизма родов при поперечносуженном тазе. При нерезко выраженной степени клинического несоответствия асинклитическое вставление головки способствует преодолению препятствия со стороны таза [8, 9]. Если затылок обращен к симфизу (передний вид высокого прямого вставления), хорошая родовая деятельность способствует дополнительному сгибанию головки, стреловидный шов поворачивается в прямой размер, и в таком состоянии головка проходит через все плоскости таза, роды завершаются самопроизвольно.
При разгибательном положении головки в заднем виде затылочного предлежания роды могут произойти через естественные родовые пути только с условием поворота головки из прямого размера на 180° и перехода в передний вид. Сохранение высокого прямого стояния является показанием к кесареву сечению.
Внутренний поворот головки при первой позиции и заднем виде происходит таким образом, что стреловидный шов смещается против часовой стрелки: из левого косого в поперечный, потом в правый косой и затем в прямой размер. Малый родничок описывает дугу 135°, переходя в передний вид. В представленном наблюдении головке, учитывая расположение стреловидного шва в прямом размере, предстояло совершить поворот на 180°.
Заключение
При поперечносуженном тазе самопроизвольные роды возможны только в переднем виде затылочного предлежания. При изначально заднем виде роды завершатся через естественные родовые пути лишь при повороте головки на 180° и переходе в передний вид. Высокое прямое стояние головки сопровождается признаками клинического несоответствия.
Использование ультразвуковых критериев позволило установить вариант анатомически узкого таза, что было подтверждено МР-пельвиметрией, а также представить доказательства вероятности благополучных самопроизвольных родов.
Цель перинатальной медицины – рождение здорового ребенка. В современных условиях применение УЗИ облегчает функциональную оценку таза, которая становится возможной уже в I периоде родов.