
A historical analysis of Tsovyanov’s and Bracht’s manoeuvres for breech birth
In Russia vaginal breech deliveries are performed according to theTsovyanov method (1928). Practically the same method is used in many European and South American countries, but is named after Bracht (1935) .van Grinsven.Dmitrieva N.N., Verhoeven A.T.M
We performed a historical analysis of the method and manoeuvres of Tsovyanov and Bracht. The source texts of both methods were examined to see if there were any similarities and/or differences and to see who might have been first if they were completely identical. The main purpose of Tsvyanov ‘s manoeuvre is to try to preserve the physiological position of the foetus (legs extended and pressed against the trunk like a splint, arms crossed in front of the chest), and ensure that the foetus is guided in the direction of the axis of the birth canal. After crowning of the breech, the gynaecologist grasps the buttocks of the foetus with both hands, so that the thumbs are placed on the thighs, while the other four fingers of both hands lie on the surface of the sacrum of the foetus.
Bracht's philosophy was as follows: ‘Gravity drastically disturbs the birth in supine position in humans from the moment that about half of the child's trunk is born. The sensible arrangement of the individual foetal parts is disturbed and leads to complications. This disintegration is prevented by the manual manoeuvre introduced by me (= Bracht)’. This is a case of a "classic multiple discovery".
Conclusion: The theory of both methods is the same. But Tsovyanov, unlike Bracht, did not use expression.
Keywords
breech birth
Bracht's method
Tsovyanovs method
history of medicine
N.N.van Grinsven–Dmitrieva worked as a gynaecologist at the Medical Academic Hospital in Kazan from 1994 to 2001. Vaginal breech deliveries were performed there according to the Tsovyanov method. Practically the same method is used in the Netherlands and many European and South American countries, but is named after Bracht, who demonstrated his method in 1935 for the Berlin Association of Gynaecologists [1] .
The leading textbook by Martius (1958), in contrast to his textbook of 1940, mentions that the Russian Tsovyanov had recommended a method similar to Bracht in 1928 [2]. Dutch dissertations on breech deliveries from the years 1930–1956 made no mention of this [3–5]. We compared the texts of both methods to see if there were similarities and/or differences and to assess who was the first.
Technique of vaginal birth according to Tsovyanov in frank breech presentation [1928] [6]
The main purpose of this method is to try to preserve the physiological position of the foetus (legs extended and pressed against the trunk like a splint, arms crossed in front of the chest), and ensure that the foetus is guided in the direction of the axis of the birth canal (Fig. 1).
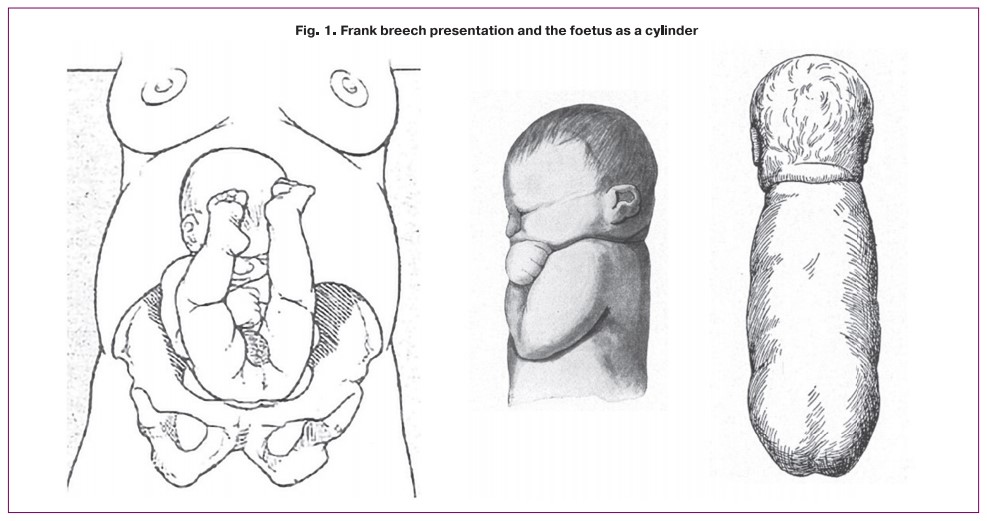
This ensures proper preparation of the birth canal for the birth of the shoulder girdle and unmolded head.
The main purpose is to prevent the legs from being born loose from the torso, i.e. hanging down. And also to maintain the normal physiological position of the foetus.
In addition, the aim is to achieve full dilation and engagement of the breech into the pelvis so that the breech descends as far as possible before starting active pushing.
After crowniong of the breech, Tsovyanov's manoeuvre is applied.
There are 4 key stages during a breech delivery:
- the birth of the foetus up to the umbilicus;
- the birth from the umbilicus to the shoulder blade;
- the birth of the shoulders and arms;
- the birth of the head.
From the time the child is born to the umbilicus, the shoulders are at the entrance to the pelvis and compression of the umbilical cord may occur.
If the child is not born within 5 minutes of umbilical delivery, suffocation may occur.
If the birth of the child from the navel takes longer than 10 minutes, the child will die.
Tsovyanov's manoeuvre for delivery in a frank breech position
After crowning of the breech, the gynaecologist grasps the buttocks of the foetus with both hands, so that the thumbs are placed on the thighs, while the other four fingers of both hands lie on the surface of the sacrum of the foetus (Fig. 2).

This prevents the premature birth of the legs and the downward (= dorsal) movement of the torso.
It is necessary to make every effort to ensure that the legs are not born separate from – i.e. not connected to – the torso before the shoulder girdle.
After appearance of the shoulder girdle, the arms are usually born spontaneously. If the arms are not born spontaneously after the birth of the scapulae, the infant's torso is guided dorsally so that the bi-acromial axis of the foetus lies in the vertical direction of the pelvic outlet.
First the forearm is born, later the hind arm and simultaneously both legs are born. If the contractions are good, the head will be born spontaneously.
For the birth of the head, it is important that the occiput is below the symphysis and in a flexed position. If the birth of the head is delayed, the aftercoming head is developed with the manoeuvre of Mauriçeau–Levret.
During trunk birth, it is very important that the foetus' legs remain clamped against the child's abdominal wall like a splint.
This is accomplished by the doctor moving his hands slowly along the sacrum and thighs toward the woman's vulva, while continuing to gently press the extended legs against the child's abdominal wall. In doing so, it is essential not to pull, but to lead in the direction of the mother's abdomen as a continuation of the axis of the birth canal.
First the child is born up to the umbilicus and then during the next contraction up to the shoulder blades. Make sure the umbilical cord is not under tension after birth by loosing the umbilical cord. So you should never pull, to prevent premature birth of the legs by transformation of the usual physiological position of the foetus.
This technique prevents premature birth of the legs and extension of the arms and deflexion of the foetus' head. With the first expulsive contraction, the torso is born up to the umbilicus and with the next expulsive contraction up to the scapulae.
Discussion
In modern obstetrics, breech presentation remains an urgent problem, since it is combined with a high frequency of complications and surgical delivery.
The description in the case of frank breech presentation is practically identical to that of Bracht [8–12]. The only difference is that Tsovyanov makes no mention of expression or anaesthesia. Bracht did so later. There is great similarity both in the underlying philosophy and in the manoeuvre. Bracht's philosophy was as follows: ‘Gravity drastically disturbs the birth in supine position in humans from the moment that about half of the child's trunk is born. The sensible arrangement of the individual foetal parts is disturbed and leads to complications. When the breech child passes through the narrow pelvis, the arms and legs are arranged at the front of the child's torso, close together to form a mosaic with flat, smooth surfaces: both forearms are crossed transversely under the chin. The transverse soles of the feet lie against the forearms without interruption. The closely spaced feet and forearms fill the space between chin and chest, covering the angular chin opposite the vaginal wall and perineum as the child continues to descend. They create space for the chin and lead it out over the perineum like a shoehorn. The torso is thus formed with the extremities into a roll with smooth surfaces, which follows the pelvic axis exactly with its axis on descent: the part already born also naturally follows the virtual extension of the pelvic axis, which turns around the symphysis and turns towards the mother's abdomen. Now, due to the supine position, a dilemma undoubtedly arises. The part of the torso which is born obeys the law of gravity, leaves the curvature of the pelvic axis, and sinks into the delivery bed. This immediately disturbs the wonderfully harmonious arrangement of the individual parts of the body: the chest, sunk over the chin, pushes the arms to the side and away from the space under the chin. Since the strong lordosis of the back, curved around the symphysis, is lost in the sink down of the torso, the hyperextension of the legs is also transferred to an extended or slightly bent position at the knee, so that the feet reinforce the displacement of the arms from the space under the chin. If, however, one stone is broken from the miraculous mosaic of which the limbs are composed, the whole structure disintegrates. This disintegration is prevented by the manual manoeuvre introduced by me (= Bracht), which helps to maintain the physiological lordosis, firmly clasps the so imperfectly assembled foetal cylinder including all the limbs and enables it to rotate around the symphysis against the force of gravity, which is undoubtedly the intention. The emergence of this last third of the foetal element of the caput standing in the straight dimension on the pelvic floor with the arms drawn together beneath it into a conglomerate, seems to me to be capable of being supported essentially by expression’ (Fig. 3) [8]. In current practice, this expression is considered to be intrinsic to Bracht's method and is taught [13–16].

It remains speculative whether Bracht knew of Tsovyanov's method. New developments in science sometimes take place simultaneously and independently of each other. Think of Darwin and Wallace's theory of evolution (1858). And these were turbulent times. The period 1919–1929 was considered a time of isolation for Russia, marked by deep mistrust [17].
There are large culturally determined differences in the use of obstetric techniques. The Bracht method has hardly found acceptance in Anglo-Saxon countries such as the United States of America and the United Kingdom [18]. In the former Eastern Bloc countries, both names are mentioned in a bibliography [19–21].
In modern obstetrics, pelvic predisposition remains an urgent problem, as it is combined with a high rate of complications and prompt delivery [22, 23].
Conclusion
To some extent, this is a case of a "classic multiple discovery". The conclusion is that the theory of both methods is the same. But that Tsovyanov unlike Bracht, did not use expression.
Biography of Napoleon Arkadyevich Tsovyanov (1882–1965) [24–26]
N.A. Tsovyanov (Fig. 4) was born in 1882 in Tbilisi, Georgia. From 1902 to 1909 he studied medicine at Moscow State University, with an interruption in 1905, when he continued his studies in Leipzig due to the temporary closure of the university as a result of the First Russian Revolution. From 1909 to 1913 he specialised as a gynaecologist in the Obstetric Clinic of the Moscow Medical Faculty. He always combined scientific research with practical work in the gynaecological field. From 1913–1918 he worked in Obstetric Clinic No. 6 in Moscow. In 1914 he was called up for military service and worked in a military hospital during World War I. After demobilisation, he volunteered to work in the army as a doctor in wounded-transportation.
From 1921 to 1952 Tsovyanov was a gynaecologist and director of Obstetric Clinic No. 4 in Moscow. From 1952 to 1960, he was professor and head of the University Women's Clinic in Moscow. He published 22 scientific works.
In 1936 Tsovyanov was promoted to candidate in medical sciences and in 1944 to doctor (in Russia there are two forms of graduation: first the candidate title, then the doctoral title). He became known for two important publications: a dissertation on the manual manoeuvre in a breech delivery and a dissertation on forceps delivery.
In 1928, he first lectured on his new method (manual manoeuvre) for breech deliveries at a meeting of the Society of Obstetrics and Gynaecology in Moscow. This was followed in 1929 by his publication on this manoeuvre in the Russian Journal of Obstetrics and Gynaecology [6]. In 1944 he received his doctorate for a dissertation on high forceps.
In 1949 Tsovyanov published an article on his method and manual manoeuvre for complete breech presentation [27]. Application of his techniques led to a sharp reduction in perinatal mortality.
References
- Bracht E. Zur Manualhilfe bei Beckenendlage. Z. Geburtsh. Gynäkol. 1936; 112: 271.
- Martius H. Die geburtshilflichen Operationen. 8th Aufl. Stuttgart: Georg Thieme Verlag; 1952.
- Freijer J.H.C. On breech positions. Diss. University of Amsterdam; 1930.
- Sikkel-Buffinga A.J. Breech presentation. Diss. University of Amsterdam; 1954.
- Hoogeveen A.J.A. About breech presentation, especially treatment using the Bracht method. University of Utrecht; 1956.
- Tsovyanov N.A. The course and treatment in breech presentation. Zhurnal akusherstva i jenskikh boleznei/ Journal of Obstetrics and Women's Diseases. 1929; 40(3): 372-9. (in Russian)].
- Bodyazhina V.I., Shmakin K.N., Kiryuschenkov A.P. Moscow; 1986. (in Russian).
- Bracht E. Zur Beckenendlage-Behandlung. Geburtsh. Frauenheilk. 1965; 25: 635-7.
- Verhoeven A.T.M. Method of Bracht – 70 years. Ned. Tijdschr. Obstet. Gynaecol. 2006; 119: 8-12.
- Verhoeven A.T.M., De Leeuw J.P. The theory of the Bracht method and its practical consequences. Ned. Tijdschr. Obstet. Gynaecol. 2008; 121: 58-60.
- Verhoeven A.T.M. Eponyms and history of breech delivery. Haarlem: DCHG; 2010.
-
Verhoeven A. De handgreep van Bracht. Een historische analyse van de onjuiste beschrijving in de verloskundige handboeken over stuitgeboorte. Ad fontes Cahier 3, TMGN. (Urk 2021) 37 pp. ISBN 978-90-831338-2-9.
Available at: https://tmgn.nl/uploaded_files/cahier3_Bracht.pdf
- Greenhill J.P., Friedman E.A., eds. Obstetrics. W.B.Saunders Company, Philadelphia: W.B.Saunders Company; 1974.
- Künzel W., ed. Breech Delivery - European Practice Gynaecology and Obstetrics. Series. Elsevier; 2003.
- Dörr P.J., Khouw V.M., Chervanak F.A., Grunebaum A., Jacquemyn Y., Nijhuis J.G., eds. Obstetric interventions. 2017, Cambridge University Press; 2017.
- Dudenhausen J.W., Pschyrembel W. Praktische Geburtshilfe mit geburtshilflichen Operationen. 22nd ed. Berlin: Verlag; 2019.
- Enno van Gelder H.A. Russia, Epos van leed en strijd, De geschiedenis van het Russische volk. Russia epos of song and strife. The history of the Russian people. Amsterdam: Elsevier; 1949.
- Cunningham F.G., Mac Donald P.C., Gant N.F. et al., eds. Williams obstetrics. 20th ed. Stamford: Appleton & Lange; 1997.
- Vajdík J., Fabian T., Sum L. Use of the Covjanov and Bracht method delivery technic in breech presentation. Gynekol. 1977; 42(9): 682-5.
- Cvajner J.P. Die Geburtsleitung bei Beckenendlagen nach der Methode von Covjanov. Sovetskaya Meditsina/ Soviet Medicine. 1952; 3: 40-1. (in Russian).
- Belyaev I.T. Zur Geburtsleitung bei Fusslagen nach der Methode von Covjanov. Akuš.ginek. 1952: 1: 39-41. (in Russian).
- Chernukha G.E., Puchko T.K. Should all women with breech presentation at full-term be delivered by caesarean section? Akusherstvo i ginekologija/ Obstetrics and Gynecology. 2007; 2: 8-14. (in Russian).
- Adamyan L.V., Artymuk N.V., Bayev O.R., Belokrinitskaya T.E., Krasnopolskiy V.I., Logutova L.S., Melnikov A.P., Petrukhin V.A., Puchko T.K., Smolnova T.Yu., Filippov O.S., Shmakov R.G., Malyshkina A.I. Breech presentation of the fetus. Clinical guidelines. Ministry of Health of the Russian Federation; 2020. Available at: https://cr.minzdrav.gov.ru/recomend/626_1 (in Russian).
- Tsvelev Yu.V., Ailamazyan E.K., Bezenar V.F. The connection of the times. Obstetricians-gynecologists of Russia for three centuries. Biographical reference book. St. Petersburg: N-L Publishing House; 2010. 575 p. (in Russian).
- Danilishina E.I. Life and work of N.A. Tsovyanov. Akusherstvo i ginekologiya/ Obstetrics and Gynecology. 1982; 2: 60. (in Russian).
- Napoleon Arkadyevich Tsovyanov (1882-1965). Obituary. Akusherstvo i ginekologiya/ Obstetrics and Gynecology. 1966; 1: 78. (in Russian).
- Tsovyanov N.A. A new method for performing a breech delivery. Akushtrstvo i ginekologiya. 1949: 2.
Received 21.10.2021
Accepted 01.12.2021
About the Authors
Nadejda N. van Grinsven-Dimitrieva, gynaecologist, Isala Klinieken loc. Sophia in Zwolle; Sworn translator/interpreter Russian-Dutch, n.van.grinsven@isala.nl, Scharten-Antinkstraat 4, 8023 CD, Zwolle, Netherlands.Dr. A.T.M. Verhoeven, gynaecologist n.p., formerly Rijnstate Ziekenhuis Arnhem, Working Group History of the Dutch Society of Obstetrics and Gynaecology, atmverhoeven1@gmail.com, Van Heemstralaan 9, 6814KA Arnhem, Netherlands.
Authors' contributions: van Grinsven-Dmitrieva N.N., Verhoeven A.T.M. - conception and design of the study, data collection and analysis, translation; Verhoeven A.T.M. - manuscript editing.
Conflicts of interest: The authors declare that there are no potential conflicts of interest.
Portions of the content overlap with published content of:
1. Verhoeven A. De handgreep van Bracht. Een historische analyse van de onjuiste beschrijving in de verloskundige handboeken over stuitgeboorte. Ad fontes Cahier 3, TMGN. (Urk 2021) 37 pp.
LINK: https://tmgn.nl/uploaded_files/cahier3_Bracht.pdf.
2. van Grinsven-Dmitrieva N.N., A.T.M. Verhoeven A.T.M. Stuitgeboorte volgens Bracht (1935) of Covjanov (1928) wie had de primeur? Ned Tijdschr Obst Gyn. 2013; 126: 245-250.
With permission of the editors of the Dutch Journal of Obstetrics and Gynaecology.
Funding: There are no sources of funding.
Acknowledgements: We express our acknowledgements to Tatyana I. Egorova for obtaining the original paper of Tsovyanov and Veronika Odintsova for help in translation.
For citation: van Grinsven.Dmitrieva N.N., Verhoeven A. T.M. A historical analysis of Tsovyanov's and Bracht's manoeuvres for breech birth. Akusherstvo i Ginekologiya/Obstetrics and Gynecology. 2022; 1:164-168 (in Russian) https://dx.doi.org/10.18565/aig.2022.1.164-168
Similar Articles

